Sleuthing The Swollen Optic Disk A nonspecific Finding





















 Disk Elevation & Thickening")
 #2) #3) #4) Disk Drusen Crowded Disk Tilted Disk")

 Metastasis - breast - lung #2) Primary Tumor #3)")





 on Fluorescein")









 Look carefully at BOTH disks!!! • Papilledema almost always present • Spontaneous Venous")
 Look carefully at SYMPTOMS! • • Headache Transient Visual Fluctuations Pulsatile Tinnitus Nausea")


 • DETECTS: –Large masses –Intracranial hemorrhaging (fresh blood) –Hydrocephalus")





- Slides: 57
Sleuthing The Swollen Optic Disk A non-specific Finding…. . Warrants a Thorough Evaluation
Speaker Disclaimers • Corporate Compensation: None • Investments/Interests: None
Critical First Test: • Unilateral or Bilateral? – Unilateral “optic neuropathy” – Bilateral “papilledema” • Until proven otherwise
Malignant Hypertension
“Post-op Vision Loss, OU”
Critical 2 nd Test: • TRUE Edema vs PSEUDOedema
Critical 3 rd Test: • Check Blood Pressure – Malignant Hypertension? • With or Without HTN retinopathy!
Critical 4 th Test: • REVIEW of SYSTEMS –Health Hx. –Medications Hx. –Symptoms
Polycythemia
Is there PAIN? ? ? • Ocular? • Head?
B. P. spike with N. A. I. O. N. “HURTS behind my eye”
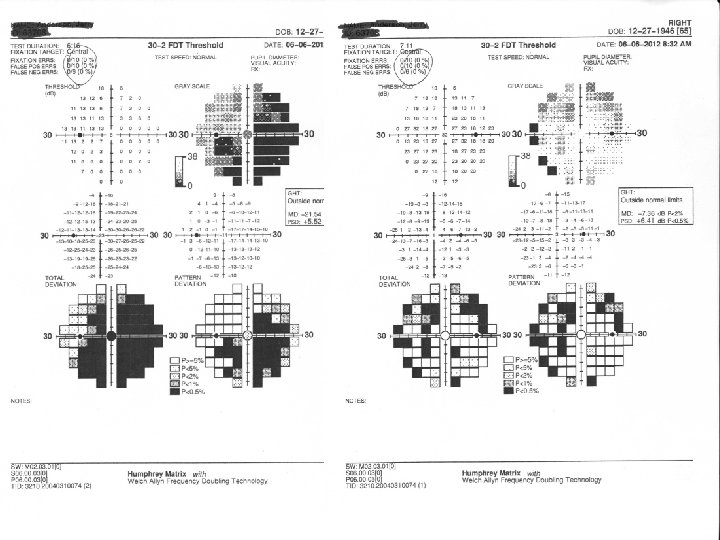
What Do The Visual Fields Look Like? • OD, OS, or OU? • RNFL “bundle defect” • Central or Ceco-central defect • Enlarged Blindspot and overall depression
Causes of TRUE Disk Edema
#1 ISCHEMIA 1 st Anterior Ischemic Optic Neuropathy 2 nd C. R. V. O. (venous stasis) 3 rd Malignant Systemic Hypertension 4 th Carotid-Cavernous Sinus Fistula (rare) 5 th Diabetic Papillopathy (rare)
“Healthy 23 y. o. male”
#2: BLOCKAGE of RETROGRADE FLUID FLOW 1 st Axonal and Intraneuronal C. S. F. - Raised intracranial pressure + Bilateral + “Papilledema” 2 nd Venous Blood - C. R. V. O. 3 rd Axonal and Intraneuronal C. S. F. - Optic Nerve Tumor - Orbital Mass Effect
#2: BLOCKAGE of RETROGRADE FLUID FLOW 4 th Bilateral Venous Outflow - C. C. S. F. - cerebral venous sinus thrombosis - right heart failure - pulmonary hypertension - sleep apnea - superior vena cava syndrome - jugular vein occlusion - dural fistula
#3: INFLAMMATION 1 st Papillitis st 1 Anterior Optic Neuritis
#4: OPTIC DISK TRAUMA • Optic Nerve Contusion
#5: TOXICITY and NUTRITIONAL NEUROPATHY • • “Moonshine Retinopathy” Drug Addiction Annorrhexia Bulimia
#6: DRAMATIC I. O. P. CHANGE • Acute Glaucoma • Ocular Hypotony
Causes of Non-Edematous (“without fluid”) Disk Elevation & Thickening
#1: OPTIC DISK IRREGULARITIES #1) #2) #3) #4) Disk Drusen Crowded Disk Tilted Disk Myelinated Nerve Fibers
#2: LEBER’S HEREDITARY OPTIC NEUROPATHY • Suspect in any case of BILATERAL “idiopathic” optic neuropathy • Inherited mitochondrial disease • Passed on by Mom • Affects both genders • Affects all ages • Diagnosis: Genetic Testing
#3: OPTIC DISK INFILTRATION #1) Metastasis - breast - lung #2) Primary Tumor #3) Leukemia #4) Lymphoma #5) Sarcoidosis
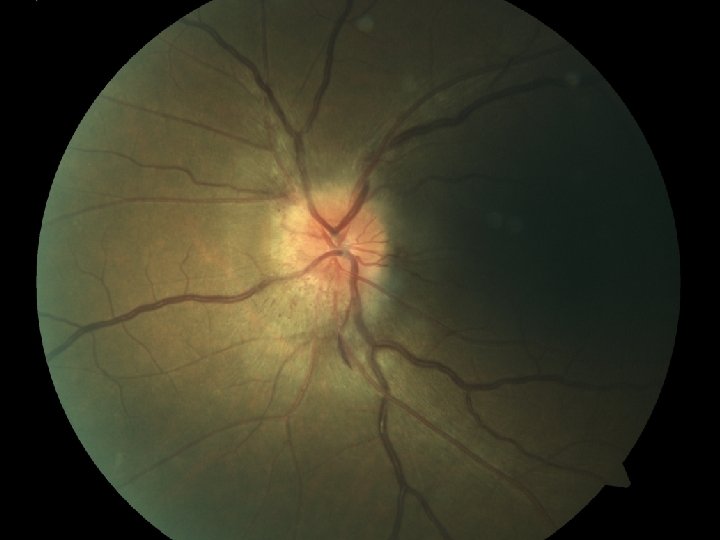
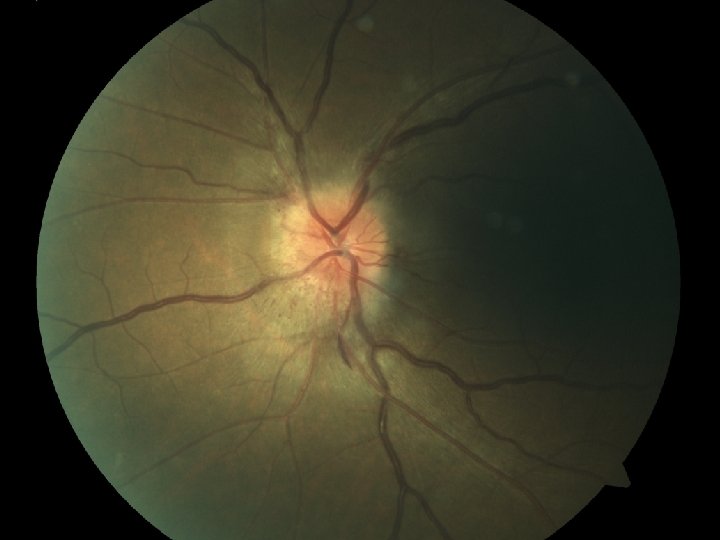
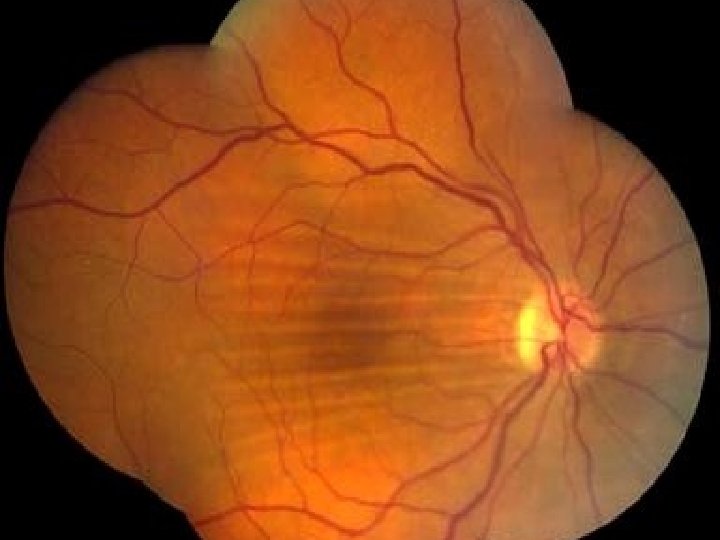
Key Findings TRUE DISK EDEMA
Look For: • Elevation • Peripapillary Retinal Sheen • Circumferential Retinal Folds • Radiating Retinal Folds • Whitening of the peripapillary retinal nerve fiber layer
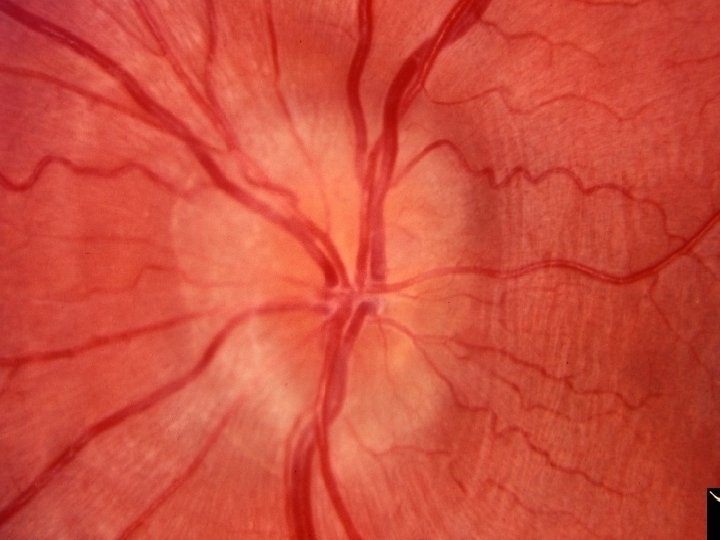
Retinal Folds?
• • Blurry Disk Margins Small Large Vessel Obscuration Venous Bloating & Tortuosity Peripapillary/Papillary Hemorrhages • Juxtapapillary Exudates
• Fluid Pockets/ “Bags” on OCT • Leakage (not “late staining”) on Fluorescein Angiography
TRUE Disk Edema…. . Now What? ?
Is it Papilledema Or Is it Optic Neuropathy ? ? ? ?
LATERALITY • Unilateral vs • Bilateral, Asymmetric
VISUAL ACUITY • Reduced “early on…” vs • Not reduced until late
COLOR VISION • Reduced “early on…. ” vs • Not reduced until late
CONTRAST SENSITIVITY • Grossly Reduced vs • NOT Reduced
VISUAL FIELDS • OPTIC NEUROPATHY – Central depression – Macular bundle depression – Arcuate pattern depression – Altitudinal pattern depression • PAPILLEDEMA – Enlarged blindspots – Scattered nasal field defects – Overall peripheral depression
T. V. O. ASSESSMENT • Transient Visual Obscurations – One eye? – Both eyes? • “How do changes in posture affect your vision? ” • “What if you bend over? ”
RAISED INTRACRANIAL PRESSURE SYNDROME
1) Look carefully at BOTH disks!!! • Papilledema almost always present • Spontaneous Venous Pulsation almost always absent
2) Look carefully at SYMPTOMS! • • Headache Transient Visual Fluctuations Pulsatile Tinnitus Nausea Vomiting Horizontal Diplopia—worse at Far Focal neurologic symptoms elsewhere in the body
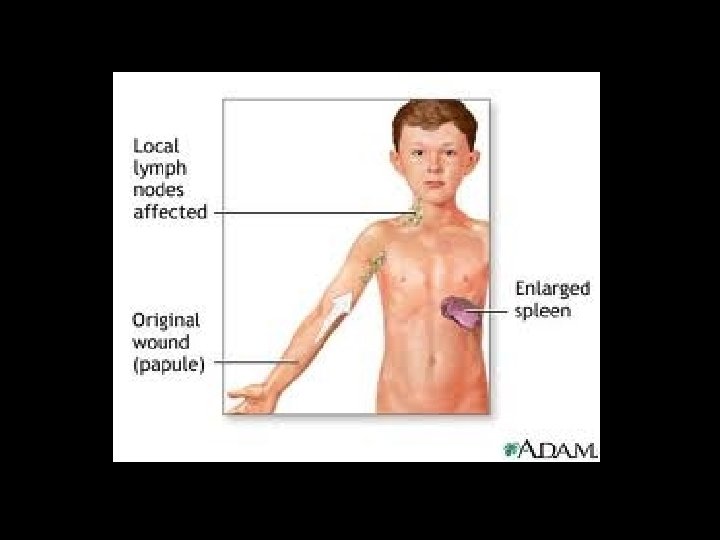
Compare that to: EDEMATOUS OPTIC NEUROPATHY • Symptoms primarily ocular/visual • Usually Hx of underlying disease • May be “classic symptoms” of that associated disease – Cranial arteritis – Lyme disease – Cat scratch disease
You now DO suspect Papilledema…. what next? Preferred Practice Patterns advise: IMAGING IS MANDATORY!
CT of Head (advisable) • DETECTS: –Large masses –Intracranial hemorrhaging (fresh blood) –Hydrocephalus
Uh, Oh. CT is “WNL” ……. But I still think my patient has papilledema……. Now What?
MRI of BRAIN with contrast • DETECTS: • • Intracranial masses Infiltrates Cerebral venous thrombosis (+/-) Meningeal pathologies
CT and MRI are Normal but Papilledema still suspected? • LUMBAR PUNCTURE – With CSF opening pressure • Normal < 200 mm • Questionable 201 -250 mm • Elevated > 250 mm – With CSF laboratory analysis • Normal = idiopathic intracranial hypertension likely • Abnormal: chronic meningitis, spinal cord tumor, etc.
Diagnosis still in Doubt? • R/O VENOUS SINUS THROMBOSIS – MRV of HEAD and NECK
Diagnosis still in Doubt? • Etiology must be a systemic venous return issue…… – Extensive cardiovascular workup indicated – “Emphasis on venous return pathologies”