Sleep Apnea Dr smr Azimi Otolaryngologist Incidence classification



.")






")
 gold standard treatment for")
 �Reducing the adenoid size and respiratory-related sleep")

- Slides: 23
Sleep Apnea Dr. smr. Azimi Otolaryngologist
Incidence & classification �Incidence: women: 20% men: 40% �Classification of Obstructive Sleep-Related Breathing Disorders: 1. Snoring 2. Upper air way resistance syndrome 3. Obstructive sleep apnea syndrome
Snoring �Snoring is sound generated by the vibration of the pharyngeal soft tissues � 40% of men and 20% of women �Types: 1. often accompanies sleep disordered breathing (SDB) 2. isolated and by definition is not associated with symptoms of excessive daytime sleepiness or insomnia habitual audible snoring occurs with an apnea hypopnea index (AHI) of less than five events per hour without daytime symptoms
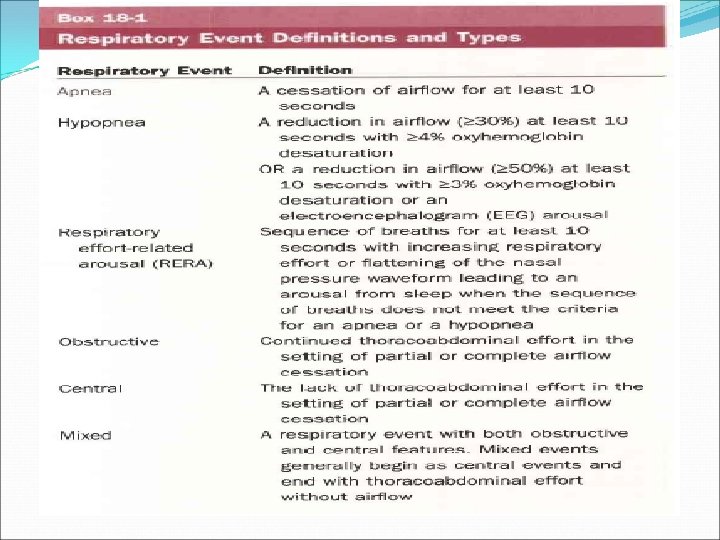
Upper air way resistance syndrome UARS is characterized by respiratory effort related arousals (RERAs). A RERA is defined as a sequence of breaths over at least 10 seconds with increasing respiratory effort that terminates with an arousal A RERA is detected using esophageal pressure manometer
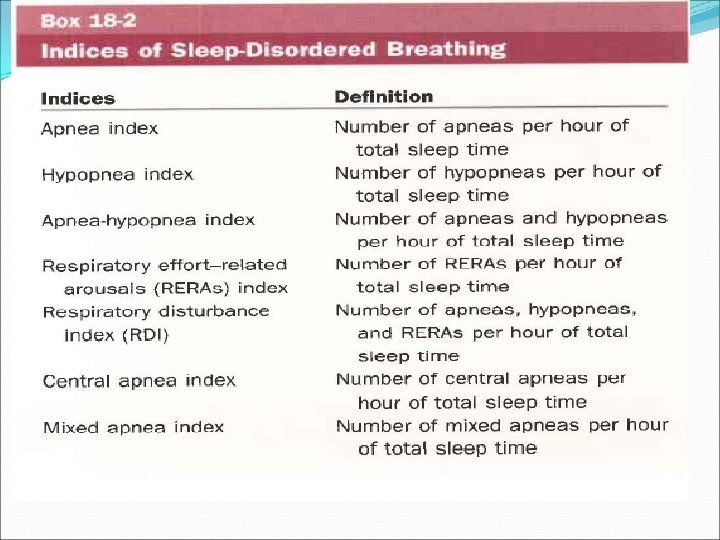
Obstructive Sleep Apnea Syndrome �OSA is defined by five or more respiratory events (apneas, hypopneas, or RERAs) in association with excessive daytime somnolence, waking with gasping, choking, or breath-holding, or witnessed reports of apneas, loud snoring, or both �Time duration: minimum of 10 seconds � commonly accompanied by reductions in blood oxygen saturation of at least 3% to 4% �usually terminated by brief, unconscious arousals from sleep
Exacerbating of OSAS Alcohol Sedative drugs Weight gain
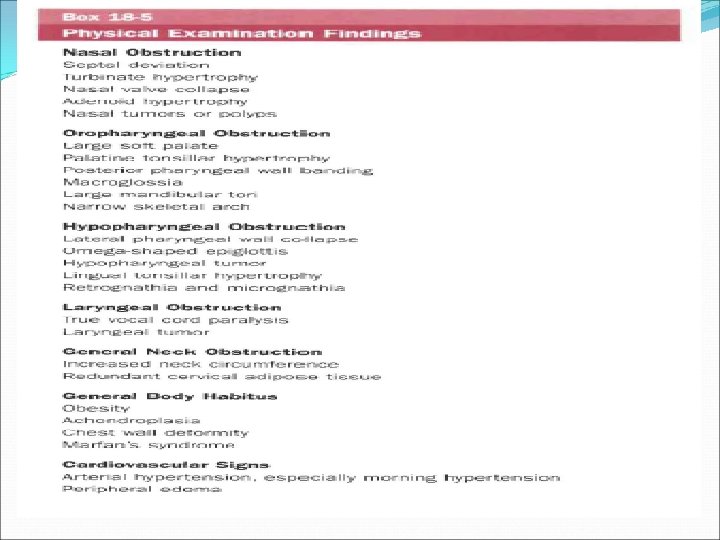
Pathophysiology �The three major areas of obstruction are the nose, the palate, and the hypo pharynx �obstructive sleep apnea associated with laryngeal obstruction from bilateral laryngeal paralysis, laryngomalacia, and obstructing laryngeal lesions �The obstruction that occurs in OSAS results from collapse of the pharyngeal airway during sleep 1. Obesity, 2. soft tissue hypertrophy, 3. craniofacial characteristics such as retrognathia add to this propensity for collapse by increasing the extraluminal tissue pressures surrounding the upper airway
�Obesity is a major risk factor for OSAS �Adenotonsillar hypertrophy is the major cause of obstructive sleep apnea in children
Fujita classification �type 1. collapse in the retro palatal region only �type II, collapse in both retro palatal and retro lingual regions �type III, collapse in the retro lingual region only
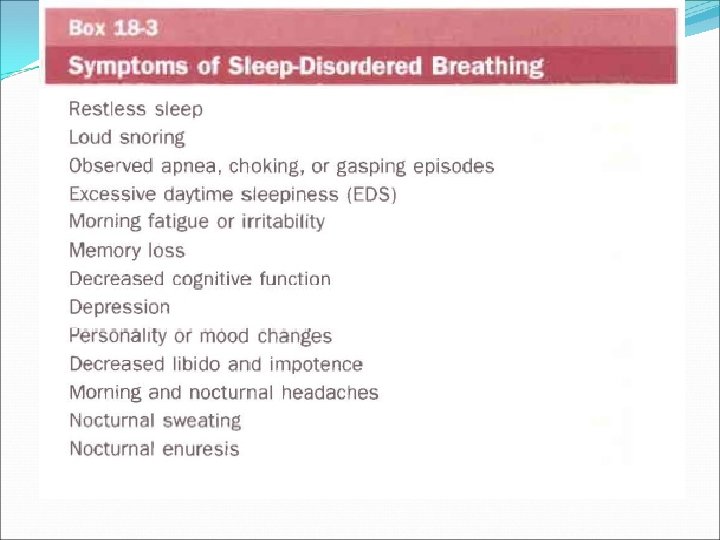
Complication of Untreated Obstructive Sleep Apnea 1. Unrefreshing sleep & excessive daytime somnolence is a common presenting complaint. 2. Automobile accidents 3. increased cardiovascular morbidity hypertension, coronary heart disease, congestive heart failure, arrhythmias, sudden death, pulmonary hypertension 4. Morning headache 5. Sore throat 6. Fatigue 7. problems with attention, working memory, , and stroke 8. GERD
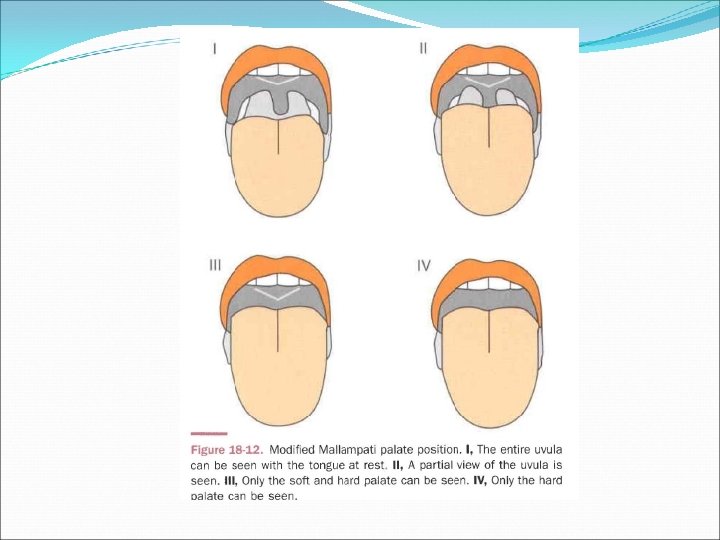
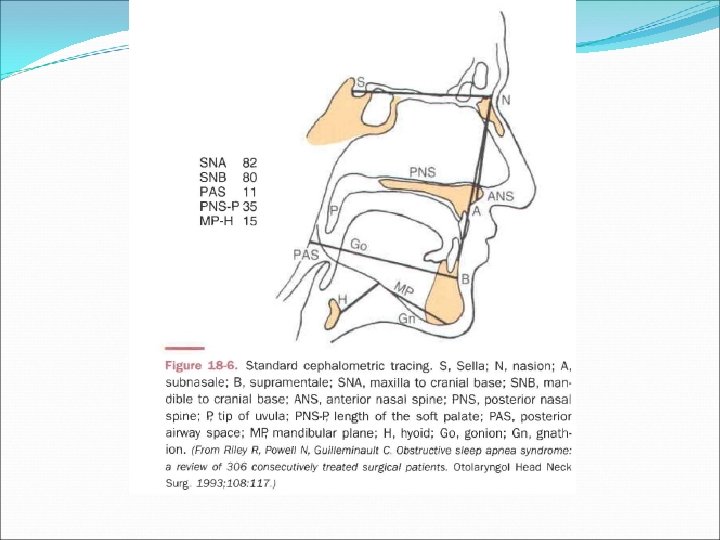
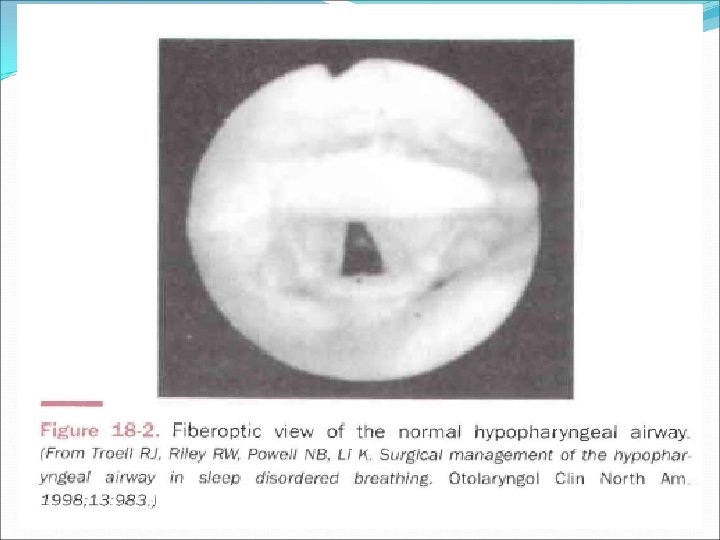
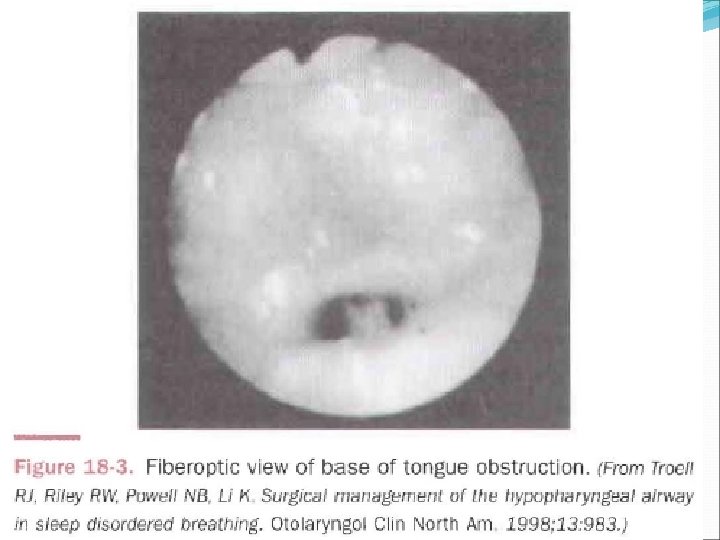
Diagnosis �Screening sleep Hx and PH/EX �Fiberoptic nasopharyngoscopy �cephalometric radiography �Awake computed tomography (CT) �Nocturnal PSG
Treatment �Medical Treatment �Weight loss �Continuous positive airway pressure (CPAP) gold standard treatment for moderate to severe OSA Reduce AHI Prevent upper airway collapse Improvement of quality of life Reduce cardiovascular events Decreased inflammation as measured by a decrease in the inflammatory markers C-reactive protein and interleukin-6, improved endothelial function, and reduced sympathetic activity
Pharmacologic therapy �Fluticasone �Leucotriene Receptor antagonist (montelukast) �Reducing the adenoid size and respiratory-related sleep disturbances in children with mild OSA �Modafinil �central stimulant of postsynaptic alpha adrenergic receptors �nasal dilator strips and topical decongestants �Reduce snoring, mouth breathing, sleepiness
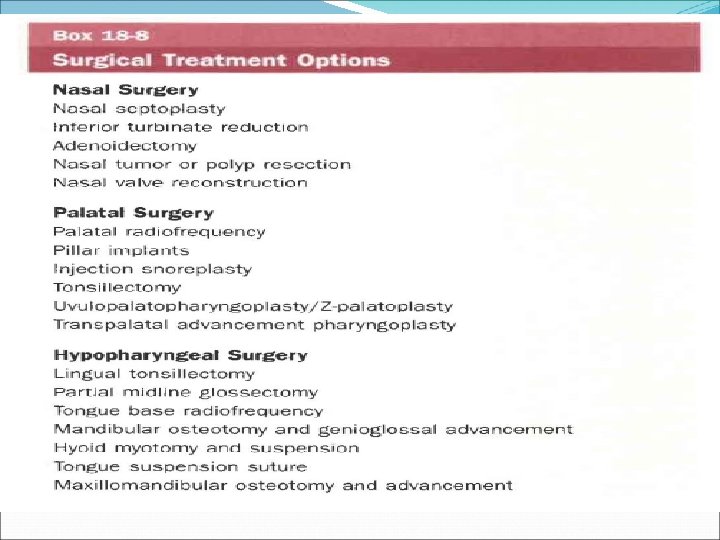
Surgical treatment � 5<AHI<14 with daytime sleepness � AHI>15 � SIO 2< 90% �Significant cardiac arrhythmias with obstruction �Unsuccessfull or refused medical treathment �Medically stabe enough to undergo procesure