Skin Rash and Visual Loss Looking for Love


















: 433 -41")













- Slides: 34
Skin Rash and Visual Loss: “Looking for Love in All the Wrong Places” Clinical Conference July 28, 2004 Edward L. Goodman, MD
Case 1 History • 57 year old divorced man referred to evaluate optic neuritis and skin rash. • He became ill three weeks earlier with febrile illness, myalgias and skin rash. His internist evaluated him and obtained normal CBC, CMP. • Shortly after, he had visual symptoms and saw an opthalmologist who diagnosed unilateral optic neuritis with visual field loss • Fever resolved but rash, fatigue, myalgias and visual loss persisted.
Exam • VS were normal. • Skin had generalized reticular rash not involving palms or soles • Bilateral shoddy axillary nodes • Normal heart, lungs, abdomen, neurologic
Lab • Normal CBC, CMP, CRP • Negative Toxo, HCV, HBV, CMV, HIV serologies • Negative blood culture • RPR 1: 128 • CSF: 48 WBC (80% LM), protein 96, VDRL negative
Course • Hospitalized overnight to obtain CSF and start intravenous penicillin • Completed 14 days IV penicillin as outpatient - 3 mu IV Q 4 H followed by one dose of Bicillin 2. 4 mu • Complete resolution of rash and visual sx • Asymptomatic permanent isolated field loss • Refused follow-up LP
Sequential Serology’s Date Serum RPR 10/1/03 1: 128 1/27/04 1: 4 5/05/04 1: 1
Case 2 History • 33 year old man referred 2/18/04 for rash and visual loss • 10/03 diagnosed as uveitis; + RPR and referred to Ft Worth ID physician; never went (couldn’t afford) • Fever, skin rash, progressive visual loss • Seen in office and admitted
Exam • • Temp 100. 2, HR 104 Cloudy vitreous, white patches in pharynx Skin rash all over including palms and soles Penile ulcer
Lab • Normal CBC, low albumin • RPR 1: 128; HIV and Western Blot + • CSF: 178 WBC (98% mononuclear), protein 79, glucose 33, VDRL 1: 16 • Penile lesion: grew HSV • CD 4 259, HIV viral load 190, 000
Course • Admit to hospital for CSF and penicillin • 14 days of IV penicillin in hospital (self pay) – Herxheimer reaction first night • Rash transiently worsened • Fever transiently higher – Bicillin at end of 14 days • Valtrex for HSV: resolved • Defer HAART for fear of IRIS • LOST TO FOLLOW UP!
Clinical Stages and Presentation of Syphilis
Typical Rash of Secondary Syphilis
Plantar Syphilid in Secondary Syphilis
Mucous Patch
CSF in Syphilis Kinghorn in Cohen and Powderly 2004
CSF in Posterior Segment Ocular Syphilis Browning. Opthalmology Nov 2000. • 14 patients with posterior segment ocular syphilis • 12/14 positive RPR (14/14 + FTA-ABS) • CSF examined in 10 – VDRL: + 3/9 – Pleocytosis: 4/9 – Protein elevated: 4/9
Ocular Syphilis • Can involve all areas of the eye – Conjunctiva – Iritis/iridocyclitis – Chorioretinitis – Posterior uveitis – Neuroretinitis • Evolving syndromes associated with HIV
Ocular Syphilis Aldave AJ et al. Curr Opin Opthalmol 2001 Dec; 12(6): 433 -41 Secondary Tertiary Conjunctiva Papillary Granulomatous Sclera Episcleritis Scleritis Cornea Marginal infiltrates, precipitates Cataracts Stromal keratitis, precipitates Cataracts Lens
Ocular Syphilis Aldave et al Secondary Uveal tract Tertiary Iridocyclitis, Chorioretinitis, vascularized iris gummas nodules, isolated vitritis, chroioretinitis
Ocular Syphilis Retina Optic Nerve Secondary Tertiary Necrotizing neuroretinitis, retinochoroid, vasculitis, serous retinal detachment Disc edema, Papilledema same Same plus atrophy, gumma
Ocular Syphilis IOP Secondary Tertiary Glaucoma glaucoma Pupils EOM Argyl Robertson Various palsies
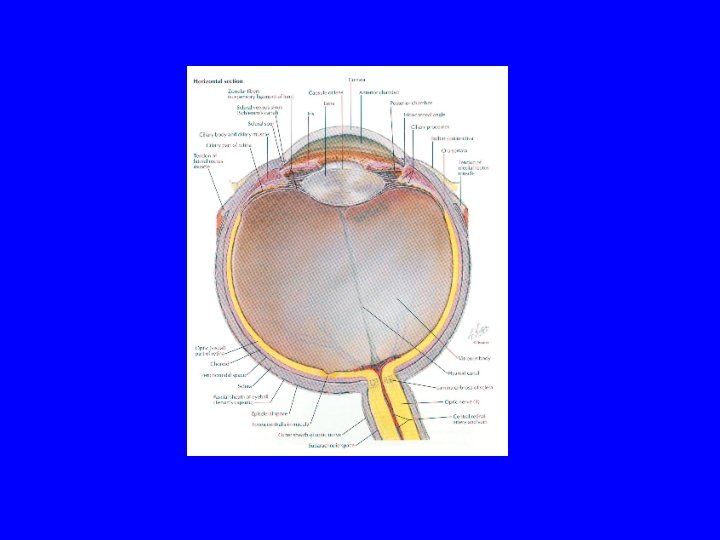
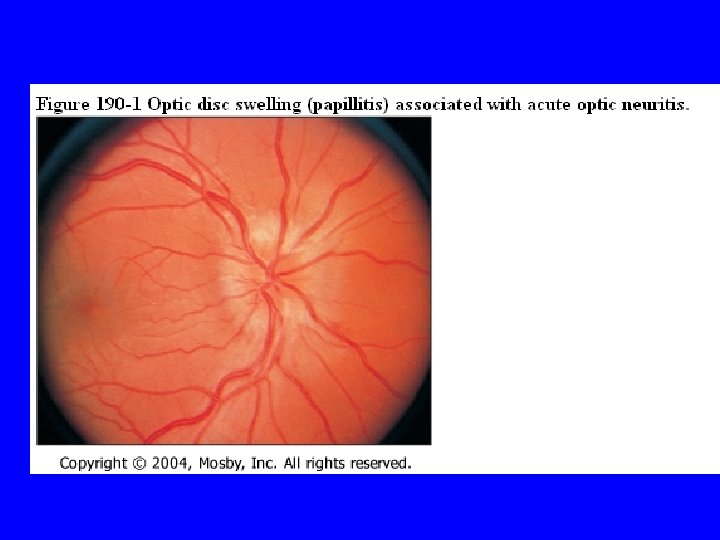
Optic Neuritis
Differential Dx of Acute Unilateral Optic Neuropathy
Specific Causes of Neuroretinitis • • • Viral and post viral Sarcoidosis Systemic Lupus and other vasculitides Syphilis Lyme Disease OI’s complicating HIV/AIDS
Optic Disc Edema and Macular Star in 13 yo girl with Bartonella Neuroretinitis
Interaction between Syphilis and HIV Cohen and Powderly 2004
Syphilis in MSM San Francisco
Syphilis in MSM Los Angeles
CDC 2002 STD Guidelines
Bibliography • Aldave A, King J, Cunningham E. Ocular Syphilis. Curr Opin Opthalmol. 2001 Dec; 12(6): 433 -41. • Balcer L, Beck R. Inflammatory Optic Neuropathies and Neuroretinitis. Yanoff Opthalmology, 2 nd ed. 2004; pp. 1263 -74. • Browning DJ. Posterior Segment Manifestations of Active Ocular Syphilis, Their Response to a Neurosyphilis Rgimen of Penicillin Therapy, and the Influence of HIV Status on Response. Ophthalmology 2000; 107: 2015 -2023. • CDC. STD Treatment Guidelines 2002. MMWR 2002; 51 (No RR-6): 18 -29.
Bibliography • CDC. Trends in Primary and Secondary Syphilis and HIV Infection in MSM – San Francisco and Los Angeles, California. MMWR 2004; 53: 575578 • Dugel P, Thach A. Syphilitic Uveitis. Yanoff: pp. 1135 -44. • Kinghorn GR. Syphilis in Cohen and Powderley. Infectious Diseases 2004: Elsevier, pp. 807 -816