Skin problems n n n n Dermatitis Bacterial

Skin problems n n n n Dermatitis Bacterial Viral Fungal Infestations Age specific Burns General principles Pages 753 -763 1

Learning Objectives n Identify Signs /Symptoms/Treatment for: n n n n Contact Dermatitis Atopic dermatitis Impetigo Cellulitis Herpes Simplex Varicella Zoster Tinea capitis Ringworm Scabies Head lice Acne Steven-Johnson Syndrome Pediatric burns 2

Contact dermatitis n n Localized irritation caused by direct, external contact with a foreign substance 2 types n n Irritant Allergic Hockenberry p 777 3

Contact dermatitis n Causes n Plants n Nickel/other metals n Topical medications n Rubber n Cosmetics n Fabrics n Detergents n Solvents n Fragrances n Sun n On & on 4

Contact dermatitis n Symptoms n n n Pruritis Redness/inflammation Skin tenderness Local swelling Local warmth to exposed area Rash/lesion 5

Contact dermatitis n Treatment n Wash affected area-lots of water n n n Soap may irritate the skin even more, don’t use it Avoid scratching Keep fingernails trimmed Medications n Topical n Corticosteroids n Lotions n Oral n Antihistamines n Steroids Skin patch testing Make sure to avoid that thing that gave you the contact dermatitis in the first place 6

Contact Dermatitis n Prevention n n Avoid offending agent Protective clothing Sunscreen Expectations n Usually resolves in 2 -3 weeks 7
 n n n Affects 3 -5% of children before the age")
Atopic dermatitis (eczema) n n n Affects 3 -5% of children before the age of 5 Genetic component- 70% have 1 st degree relative with some form of AD 50 -80% will develop allergic rhinitis or asthma 8

Atopic dermatitis n Symptoms n n n Dry, scaly, pruritic lesions Weeping, oozing, crusting lesions Often erythematous Chronic relapse/remission pattern Tend to be more susceptible to viral skin infections http: //www. riskindoc. com/dermatitis_eczema. html 9

Atopic dermatitis n Symptoms n n Typically seen on the face, inside the elbows, and behind the knees Appearance of rash will depend on the amount of scratching Worse in fall/winter Secondary infection 10

Atopic dermatitis n n n Treatment Topical medications Systemic medications Other topicals Other treatments n n Avoid triggers n n Sometimes use phototherapy (about 12 y/o and older) Tepid water for bathing Increase humidity in winter months 11

Impetigo n n Common, contagious, superficial, bacterial infection Group A β- hemolytic streptococcus n n Staphylococcus aureus n http: //www. cgh. com. sg/caring/issue 82/Pg_6_7_8. asp Brown crusty blisters Clear then cloudy blisters Hockenberry p 767 12

Impetigo n n Preschoolers/ school age Those In Close Physical Contact n Day care Warm, Moist Climate Poor Hygiene https: //mayoclinic. com/health/medical/IM 00401 13

Impetigo n n n Spread by direct contact Can be itchy Can occur on any part of the body n Usually hands, forearms, nose, & mouth Copyright Mosby 2002 14

Impetigo n Treatment n Antibiotics n n Gentle cleansing of crusted areas n n Topical, sometimes use systemic if it’s a huge area that is affected With warm soapy water, but don’t want to break the blisters. It doesn’t speed up healing and opens up the way for infection Cover infected areas Don’t rupture the blisters Prevention n Good hygiene n n n Regular hand washing Separate towels/linens Keep fingernails cut short 15

Cellulitis n n n Inflammation of the skin and subcutaneous tissues Associated with pain, swelling, intense redness Opportunistic n n n Any area of broken skin Immunocompromised/diabetics NOT contagious page 767 16

Cellulitis n Bacterial infection n Staph n Strep n Pasteurella multocida n n Animal bites Pseudomonas n Puncture of foot through sneakers 17

Cellulitis n Symptoms n n n n Inflammation with redness Pain Swelling Warm to touch Lymphangitis- streaking Fever, malaise Swollen regional lymph nodes 18
 n Antibiotics n n n Oral Elevation, immobilization")
Cellulitis n Treatment (mild/treated at home) n Antibiotics n n n Oral Elevation, immobilization Warm, moist compresses Pain relievers Close monitoring n Hospitalization, if necessary 19

Herpes Simplex n n n n Type I n Usual exposure- preschool years n Typically found above the waist, but can be anywhere Type II n Sexually transmitted n Typically found below the waist, but can be anywhere Once exposed always present Outbreaks Very contagious Spread by direct contact No cure 20

Herpes Simplex n Triggers n n Stress Increased exposure to sun Viral infections Food high in arginine http: //www. minarsdermatology. com/medical/coldsores. asp 21

Herpes Simplex n Symptoms n n n Tingling, numbness, burning, itching Small erythematous, tender area clusters of blisters Blisters begin to dry yellow crusting Possible regional lymphadenopathy Usual coarse 7 -10 days 22
 n n If it")
Herpes Simplex n Complications n n Possible scarring Blindness (ocular) n n If it gets into the eye Depression (type 2 HSV) 23

Herpes Simplex Treatment n Goal - control outbreaks n Medication n n Pain relievers Compresses Other Antivirals need to be given in the first 24 hours after the first lesion 24

Varicella zoster n Shingles n n n Same virus that causes chicken pox Anyone who has had chicken pox or the vaccine can have varicella zoster Chickenpox may follow exposure to shingle 25

Varicella zoster n Causes n n n Stress Fatigue Weak immune system Cancer Radiation 26

Varicella zoster n Symptoms n Pre-eruption n n Intense, localized pain along a dermatome Fever/malaise Lesions occur 1 -7 days Progress thru rupture, crusting, and healing over 2 -3 weeks 27

Varicella zoster n n Is unilateral Follows dermatomes 28
 Postherpetic neuralgia")
Varicella zoster n Complications n n Scarring Secondary infection Hearingvision loss (facial) Postherpetic neuralgia (PHN) n Pain persists after the rash has completely healed, can last a long time (months or years). Rare in children, but it can happen 29

Varicella zoster n Treatment n n n Avoid scratching Keep fingernails trimmed Medication n Antivirals n n In first 24 hours! Can slow down the shingles or prevent them from popping up in the first place Pain Cool compresses/ baths Good hygiene 30
 n Fungal Infection That Lives On, Not In, The")
Dermatophytoses- Tinea (aka. - Ringworm) n Fungal Infection That Lives On, Not In, The Skin, Or Nails Spread by: n n n Direct contact Indirect contact Contact with soil n rare www. emedicinehealth. com/slideshow_ringworm_pictures/article_em. htm 31
 n Symptoms n n Begins as small lesion Enlarges, leaving scaly")
Tinea capitis (head) n Symptoms n n Begins as small lesion Enlarges, leaving scaly patch Alopecia Worst case, develops into kerion n n Like a boggy gross thing, immune response to the ringworm Hair usually grows back kerion 32
")
Tinea capitis n Treatment n n Griseofulvin Topical antifungal Selenium sulfide shampoo Corticosteroids (kerion) 33
 n Symptoms n n n Begins as small lesion Enlarges, leaving")
Tinea corporis (body) n Symptoms n n n Begins as small lesion Enlarges, leaving scaly patch Center usually clears leaving the “ring” appearance Copyright Mosby 2004 34
 n Treatment n n Griseofulvin Topical antifungal 35")
Tinea corporis (body) n Treatment n n Griseofulvin Topical antifungal 35
 n Symptoms n n Pruritic Medial proximal aspect of thigh/")
Tinea cruris (‘jock itch’) n Symptoms n n Pruritic Medial proximal aspect of thigh/ crural fold (may involve scrotum in males) 36
 37")
Tinea cruris n Treatment n n Topical antifungal Compresses/ sitz baths (comfort) 37
 n Symptoms n n Pruritis Lesions to plantar surface of")
Tinea pedis (athlete’s foot) n Symptoms n n Pruritis Lesions to plantar surface of foot, between toes 38

Tinea pedis n Treatment n n Griseofulvin Topical antifungal Severe cases- topical glucocortical cream Eliminate causes 39

http: //www. emedicinehealth. com/slideshow_ringworm_pictures/article_em. htm
 n n Skin infestation with microscopic mite Spread skin to skin")
Sarcoptes scabei (Scabies) n n Skin infestation with microscopic mite Spread skin to skin Crowded conditions If you got one today it would take a couple of months before you began to feel the effects http: //www. dermisil. com/products/what/scabies. asp 41
 n n n Female burrows under the skin Lays 2 -3")
Sarcoptes scabei (Scabies) n n n Female burrows under the skin Lays 2 -3 eggs/day Eggs hatch and in 10 days—adult mites! http: //www. dermnetnz. org/common/image. php? path=/arthropods/img/s/scabies 3. jpg 42
 n Symptoms n n n Severe pruritis Small, tiny lesions develop")
Sarcoptes scabei (Scabies) n Symptoms n n n Severe pruritis Small, tiny lesions develop into blisters Usually on hands or feet http: //www. dermnetnz. org/common/image. php? path=/arthropods/img/s/scabies 2. jpg 43
 n Treatment n ? Whole family? n n n Scabicide -")
Sarcoptes scabei (Scabies) n Treatment n ? Whole family? n n n Scabicide - Permethrin (Elimite) Treat personal items n n Yes!! Spread by close, prolonged contact. The mite takes about 45 mins to burrow under your skin Clothes, bedding, towels, wash in hot water Lotions Topical steroid for itch Antibiotics- secondary infections 44
 n n n Very common, parasitic infestation Typically affects ages")
Pediculosis capitus (head lice) n n n Very common, parasitic infestation Typically affects ages 3 -12 Very contagious, very annoying http: //www. haircareguide. com/lice. htm 45

Pediculosis capitus n n n Person to person contact Object to person contact Not carried by animals 46

Pediculosis capitus n Adult Louse n Small, grayish-tan, wingless insect n Visible n Can live up to 3 days away from a human host n Life span of female is 1 month n n http: //www. msmosquito. com/headli ce. html In this time can lay 100 -200 eggs… eww Use claws to hold to hair shaft http: //bioweb. uwlax. edu/bio 203/s 2008/koc h%5 Fsama/Nutrition. htm 47

Pediculosis capitus n n Feed on small amounts of blood from the scalp every 4 -6 hours Eggs will hatch 1 -2 weeks after being laid 48 http: //www. msmosquito. com/headlice. html

Pediculosis capitus n Symptoms n n n May note small, red lesions Persistent pruritis Nits on hair shafts Visible adult lice Regional lymphadenopathy Secondary infection 49

Pediculosis capitus n Treatment n n n Medicated shampoos Mechanical removal of nits Wash all linens Vacuum/ dry clean nonlaundry items Repeat treatment in 7 -10 days Treat secondary infection as needed 50
 n n n Hockenberry p 849 -852 n Most common skin")
Acne vulgaris (acne) n n n Hockenberry p 849 -852 n Most common skin problem of adolescence 50% of adolescent population will experience acne Not caused/worsened by foods Has a hereditary factor 51
 n Causes n Hormones n n n Increased sebum (oil) gland")
Acne vulgaris (acne) n Causes n Hormones n n n Increased sebum (oil) gland activity Comedone formation Overgrowth of Propionibacterium acnes 52
 n Treatment n n n Wash-don’t scrub Oil-free make-up Keep your")
Acne vulgaris (acne) n Treatment n n n Wash-don’t scrub Oil-free make-up Keep your hands off!! Lotions/creams Medications n n n Retinoids Topical Antibacterial Agent Systemic Antibiotics Oral Contraceptives If using topicals, AVOID SUN, or AT LEAST USE SUN SCREEN 53
/ Toxic Epidermal Necrosis (TEN) n n Severe manifestation of erythema multiforme")
Stevens-Johnson Syndrome (SJS)/ Toxic Epidermal Necrosis (TEN) n n Severe manifestation of erythema multiforme Mortality can be as high as 25%-35% (TEN) emedicine. medscape. com/article/756523 -media 54
/ Toxic Epidermal Necrosis (TEN) n Causes n Infections n n 50%")
Stevens-Johnson Syndrome (SJS)/ Toxic Epidermal Necrosis (TEN) n Causes n Infections n n 50% of patients report recent URI Drug induced n Sulfa, Penicillin, cocaine Malignancy (adults) n Idiopathic n 55
/ Toxic Epidermal Necrosis (TEN) n Signs/symptoms n n n Cough Headache")
Stevens-Johnson Syndrome (SJS)/ Toxic Epidermal Necrosis (TEN) n Signs/symptoms n n n Cough Headache Malaise Arthralgia Mucocutaneous lesions 56

/ Toxic Epidermal Necrosis (TEN) n Treatment n Support symptoms n n")
Stevens-Johnson Syndrome (SJS)/ Toxic Epidermal Necrosis (TEN) n Treatment n Support symptoms n n n Remove offending agent Treat lesions as burns n n May get care from burn units in the hospital Cover denuded skin n n Many times we don’t know what’s caused it Cover with gauze wet with solution Prevent secondary infection 58

Pediatric Burns - Causes n n n n Extreme heat sources Cold Chemicals Electricity Radiation Accidental – inadequate supervision, curiosity, inability to escape burning agent Intentional (Child Abuse) 59

Guides to Treatment n n n Extent Depth Severity n n Percentage of total body surface area (TBSA) burned Location Child’s age General health 60
 n Rule of Nines n Lund Browder")
Extent - Total Burn Surface Area (TBSA) n Rule of Nines n Lund Browder 61

Rule of Nines http: //emedicine. medscape. com/article/769193 -print http: //www. medtrng. net/efmb/tasks/081 -833 -0070. htm
 n Only epidermis,")
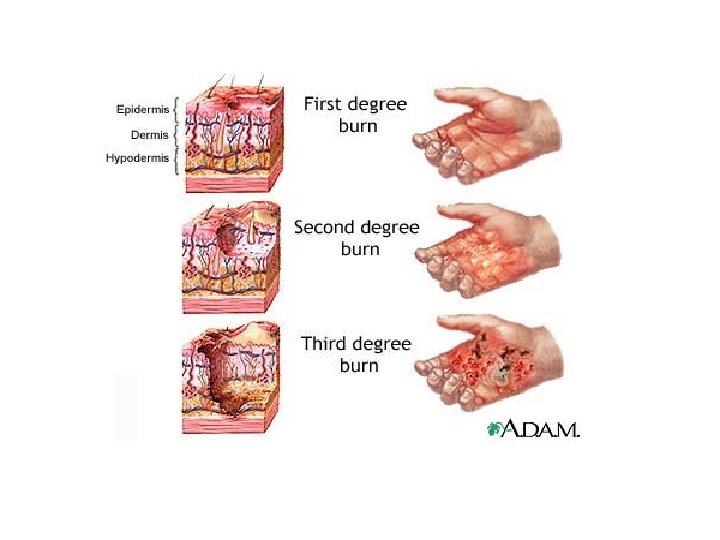
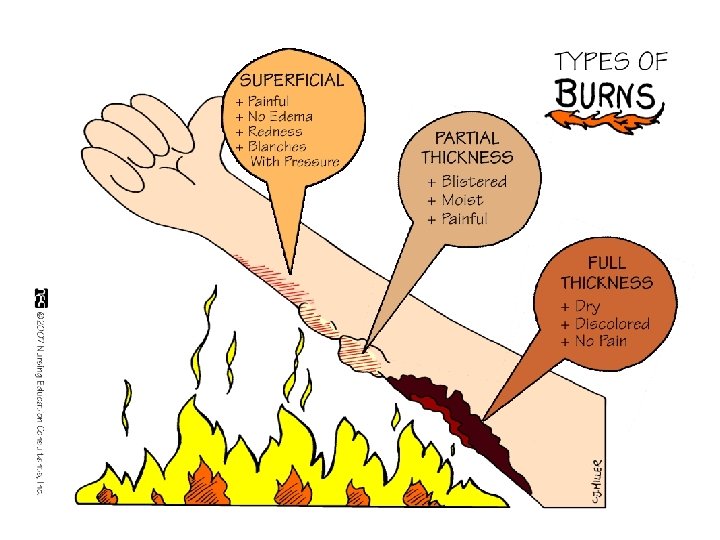
Depth and Severity n Depth n Superficial (1 st degree ) n Only epidermis, blisters, gone in days, not scarring Partial thickness (2 nd degree ) n n sensory is intact, moist skin, scarring is low, but takes longer to heal n Full thickness (3 rd and 4 th degree) n Dermis, epidermis, and subq tissue, if you burn thru this then it’s not painful because you’ve killed all the nerve cells. Don’t usually heal, may need skin grafts and what not 63

Second degree burn http: //emedicine. medscape. com/article/769193 -media 66

3 rd degree burns http: //emedicine. medscape. com/article/769193 -media 67

Burn Unit Referral Criteria 1. Partial-thickness burns > 10% TBSA 2. 3. 4. 5. 6. Burns involving face, hands, feet, genitalia, perineum, or major joints 3 rd degree burns Electrical burns, including lightning injury Chemical burns Inhalation injury 7. Preexisting medical disorders that could complicate management, prolong recovery, or affect mortality 8. Concomitant trauma (such as fractures) in which the burn injury poses the greatest risk of morbidity or mortality. 9. Burned children in hospitals without qualified personnel or equipment for the care of children 10. Special social, emotional, or rehabilitative intervention requirements She won’t test us on this but it’s just good to know or whatever…
 n n Avoid sun, wear protective clothing, sunscreen")
Burn Care n Superficial burns (sunburn) n n Avoid sun, wear protective clothing, sunscreen Minor burns n n n Apply cold compress Analgesia Cleanse with soap /water – avoid friction Tetanus Antimicrobial ointment Loose clothing 69

Care of Moderate and Severe Burns n n n n Maintain airway, Oxygen IV access/ fluids Observe closely for s/s shock Pain management Wound care Nutritional support Skin and musculoskeletal care Emotional/psychosocial support 70
 [2")
Parkland Formula Fluids for 24 hours = (4 х kg х % burn) [2 nd & 3 rd degree burns added together] 1 st 50% given over 8 hours Followed by 2 nd 50% given over 16 hours n n Example 4 X 20 kg X 35% = 2800 Give 1400 in 8 hours = 175 ml/hr Remaining 1400 over next 16 hours at 88 ml/hr 71

Systemic Responses/Complications n Cardiovascular system n Burn shock n n n Hemoconcentration/hyperviscosity Treatment - Fluid resuscitation n n From loosing fluids Watching urine output is key, you know they’re hydrated if their I&O is even Commonly use Parkland formula Maintain urine output 1 -2 ml/kg Renal System n n Immature infant renal system Fluid loss reduces renal blood flow 72

Responses/Complications n n Metabolism n Hypermetabolism Pulmonary ndary to smoke/carbon dioxide, heat n Injury 2 n Pulmonary edema Wound Sepsis GI System n Stress ulcer 73

Burn Wound Management n n n n Excision/Debridement Topical antimicrobial agents Temporary skin substitute Synthetic Skin coverings Artificial skin Permanent skin coverings Cultured epithelium 74

Complications n Long term n n Contracture deformities Body image 75

Prevention/Parent Education n n Never leave child alone Install smoke alarms – check monthly Lower hot water setting to <120 degrees Keep matches, gasoline, candles away from children Use stove back burners and turn pot handles 76

Prevention/Education n n Keep hot foods/liquids away from table edge Keep electrical cords out of reach Practice fire escape Teach - Stop, drop, and roll Place microwave at safe height (higher than children’s faces but low enough to reach easily) 77
- Slides: 77