Skin Cancer Carlos Garcia MD Dermatology at OUHSC






")






 n Basal skin cancers cell carcinoma n Squamous cell carcinoma n")
")






 n n BCC is 4")
 n Surgical excision n Traditional n Mohs")












")







- Slides: 44
Skin Cancer Carlos Garcia MD Dermatology at OUHSC No conflicts of interest to disclose
Objectives n Identify clinical characteristics of n Precancerous lesions n Common skin cancers n Define risk factors for development of skin cancer n Choose appropriate methods for diagnosis and treatment
Precancerous skin lesions n. Actinic n. Dysplastic keratoses melanocytic nevi
Actinic keratoses 10% risk of malignant transformation
Hypertrophic AK’s
Actinic cheilitis
Treatment of AK’s n Liquid nitrogen cryotherapy n Topical therapies n 5 -FU (Efudex) n Imiquimod n (Aldara) Curettage for hypertrophic lesions
Liquid nitrogen Cryotherapy Residual hypopigmentation Blister formation
Topical therapies Efudex or Aldara * 3 -5 times per week * 6 -8 weeks
Dysplastic nevi • Precursors for melanoma • Markers for melanoma
Treatment of dysplastic nevi
n Non-melanoma (NMSC) n Basal skin cancers cell carcinoma n Squamous cell carcinoma n Keratoacanthoma
Risk factors for development of BCC and SCC n Fair skin (Fitzpatrick’s types I-III) n Blue eyes n Red hair n Family history n Genetic syndromes n Chronic sun exposure n Old age n Arsenic, tar
Basal cell carcinoma
BCC- clinical types n Nodular n Pigmented n Infiltrative n Superficial n Morpheaform
Nodular BCC n Chronic lesion n Easy bleeding n Pearly border n Surface telangiectasias n Head and neck, trunk, and extremities
Pigmented BCC n Similar to nodular but with black discoloration n Melanin deposits n Pigmented races n Face, trunk, and scalp
Superficial BCC n Erythematous scaly plaque n Slow growth n Asymptomatic n Trunk, extremities, face
Morpheaform BCC n Resembles scar n Asymptomatic and slow growing n Ill-defined margins n Marked subclinical extension
n BCC is the most frequent skin cancer (80%) n n BCC is 4 x more frequent than SCC Metastases are rare (<1% of cases) n Local destruction of tissue
Treatment of BCC n Curettage electrodessication (ED/C) n Surgical excision n Traditional n Mohs surgery n Radiation therapy n Topical therapy n imiquimod 95% Cure Rate 50 -75% Cure Rate
Squamous cell carcinoma
SCC types n n n In-situ n Bowen’s disease n Erythroplasia of Queyrat Invasive SCC Keratoacanthoma
Bowen’s disease n In-situ SCC n Arsenic, HPV 16, radiation
Erythroplasia of Queyrat n In-situ SCC n Uncircumcised men n May progress to invasive SCC
Invasive SCC n Erythematous nodule n Indurated lesion n Sun-exposed skin n Men > women n Slow growth
Invasive SCC
Keratoacanthoma n Low grade SCC n Rapid growth over weeks n Trauma, sun exposure, HPV 11 and 16 n May progress to invasive SCC
n SCC is locally invasive and destructive n Metastases in 1 -3% of cases n To lymph nodes n 50 -73% survival n Distant sites (lungs) n Incurable
Treatment of SCC n Bowen’s disease n Erythroplasia of Queyrat n Efudex or aldara n Liquid nitrogen cryotherapy n Radiation therapy n Curettage electrodessication (ED/C) n Surgical excision
n Invasive squamous cell carcinoma n Surgical excision n Traditional n Mohs surgery n Radiation therapy
Malignant Melanoma (MM)
Risk factors- MM n Fair skin, red hair, and blue eyes n Intermittent sun exposure n Sunburns n Tanning beds n Freckles and melanocytic nevi n Family history of melanoma
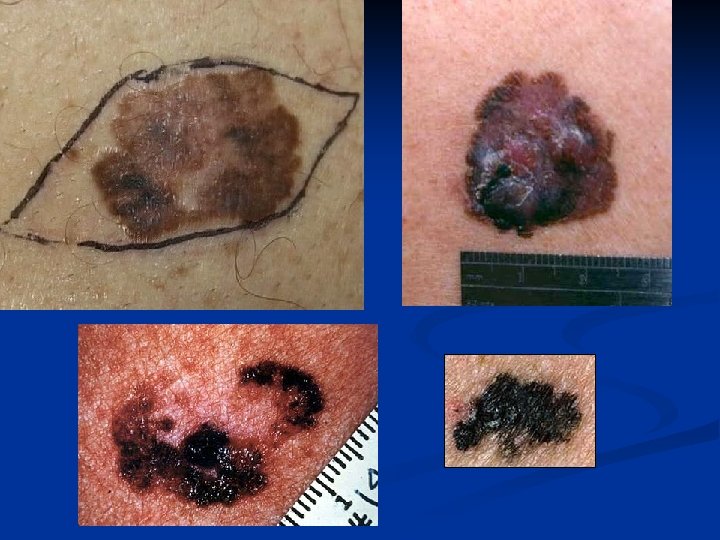
Clinical types- MM Superficial spreading melanoma Lentigo maligna melanoma Acral lentiginous melanoma Nodular melanoma
ABCD of Melanoma n Asymmetry n Border irregularity n Color variegation n Diameter >6 mm
Prognostic features- MM n Good prognosis n Breslow < 1 mm n Intermediate prognosis n Breslow 1 -4 mm n Bad prognosis n Breslow >4 mm
Treatment of MM n Surgical excision n In situ = 5 mm margin n Invasive= 1 -3 cm depending on Breslow’s depth
Sentinel lymph node biopsy- MM n Recommended for MM with Breslow 1 -4 mm n Lymphadenectomy for positive nodes n Powerful prognostic feature for disseminated disease n It does not affect survival of patients
Thank you