Skin and Soft Tissue Tumors Dr Jamaleldin Hassainan







 o Present at birth or appears 2 -3 weeks after")







 o Most common malignant carcinoma o Predisposing factors :")






 o Growth is slow , steady & insidious. Several years")












 o Other causative agents are chronic contact with tars hydrocarbons")

 o Grows initially starts as a erythomatous plaque or nodule with")








 o Pink base with indistinctive irregular edges o Family")

 o Etiology - Ultra violet increase risk -Familial Hx has been")







 o TREATMENT SMALL METASTISIS BCG NOT SUITABLE FOR")
- Slides: 62
Skin and Soft Tissue Tumors Dr. Jamaleldin Hassainan
Arise from any histological structures that make up skin o Epidermis o Connective tissue o Glands o Muscle o Nerves
CLASSIFICATION o Benign o Premalignant o Malignant
Common Benign Tumors o. Heamangiomas : o. Involuting o. Non- involuting
Involuting Heamangiomas of childhood o 95% of all heamangiomas o Not a true neoplasm o Neoplasm of endothelial cells o Undergo complete spontaneous involution
Involuting Heamangiomas (cont. ) o Present at birth or appears 2 -3 weeks after birth o Grows rapidly 4 -6 months o Spontaneous involution complete 5 -7 yrs
Classification Involuting o. Superficial o. Combined o. Deep
Superficial Involuting o Strawberry nevus o Nevus vasculosa o Capillary heamangioma Appearance : o Sharp demarcated red o Slightly raised lesion & irregular surface
COMBINED o Strawberry o Capillary & Cavernous Appearance : A firm bluish tumor , may extend deeply into sub cutaneous surface
Deep Involuting o Cavernous o Appearance : Blue tumor covered by normal skin o Treatment : Requires no treatment involving vital organ eg. lid
Non Involuting Heamangiomas o Usually present at birth o No rapid growth o Growth is proportion to growth of child o Persists into adulthood o Causes severe aesthetic problems o May cause arterio venous fistula , eventually lead to cardiac failure. o Treatment : Not satisfactory
Port Wine Stain o May involve any portion of the body o When present in face as a flat patch correlating to sensory branch of 5 th nerve o Microscopic appearance : o Thin walled capillaries distributed throughout the dermis lined by thin mature endothelial cells o Treatment : Unsatisfactory - Tattooing - Laser -Radiotherapy
Malignant Tumors o. Basal cell carcinoma o. Squamous cell carcinoma o. Malignant Melanoma
Basal Cell Carcinoma (Rodent ulcer) o Most common malignant carcinoma o Predisposing factors : o Age >40 yrs o Ultraviolet light exposure o Fair skin , blond hair & blue eyes living in tropical climate i. e. westerners living in Saudi Arabia.
Predisposing Factors (cont. ) o Growth is slow , steady & insidious. Several years may pass before patient becomes concerned. o Invade adjacent tissue , massive ulcerations. o Rarely metastases & death may occur by invading deeper extension into intracranial or major blood vessels.
APPEARANCE o Small , translucent skin elevated nodule o Rolled pearly edges o Telangiactic vessels occur commonly on surface
Sclerosing Morphia o Less common o Elongated strands of basal that infiltrate the dermis. o Flat & whitish or waxy appearance and firm palpation
Erythromateous Basal Cell Carcinoma o Body basal occurs most frequently on the trunks. o Appears reddish plaques with atrophic center o Smooth slightly raised borders.
Pigment Basal o. Sometimes mistaken for melanoma
Treatment o Radio therapy : Good in treatment of structures that are difficult to reconstruct. Should not be used in pt. under 40 y , or in pt. who failed to respond to radiation therapy Treatment : 4 -6 weeks
Treatment o Curettage & Electro desiccation : Excise 2 -3 mm margin o Surgical excision : small moderate size lesion down to subcutaneous tissue
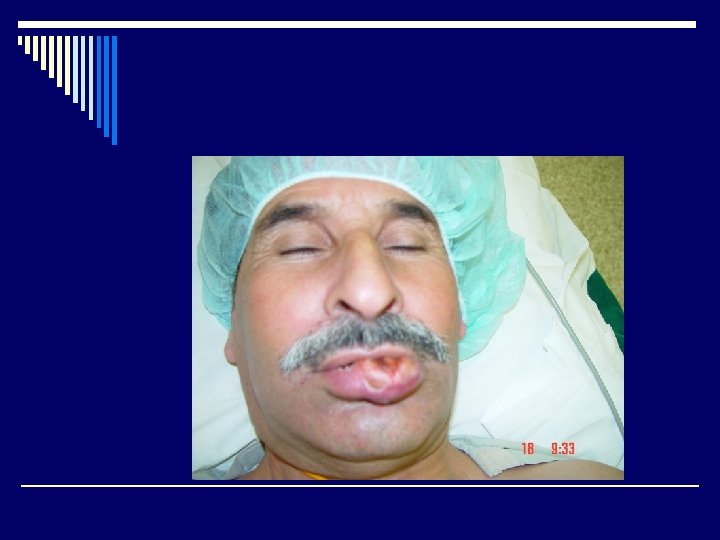
Squamous Cell Carcinoma o 1 st most cancer in dark skinned people o 2 nd most cancer in light skinned group o Causative agents same as basal cell carcinoma. o Most common sites are the ears , cheeks , lower lip & back of the hands.
Squamous cell (cont. ) o Other causative agents are chronic contact with tars hydrocarbons & exposure to ionizing radiation. o Also chronic ulcers , thermal burns healed with fibrosis ( Marjolins ulcer ) o These are aggressive tumors , does not usually metastasize , as fibrosis & initial burns has already destroyed lymphatic
Presentation o Locally invasive without metastasizing from premalignant tumors eg. Bowens disease , chronic radiation dermatitis. o Rapidly growing widely invasive with metastasizes especially squamous cell tumors arising from normal skin.
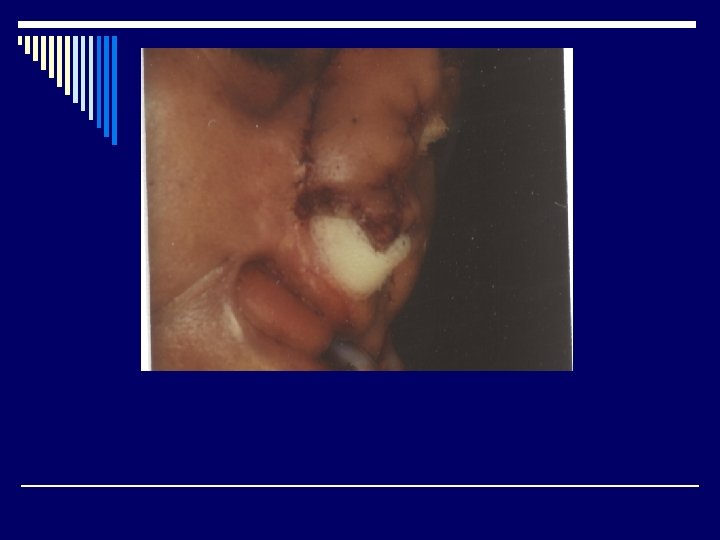
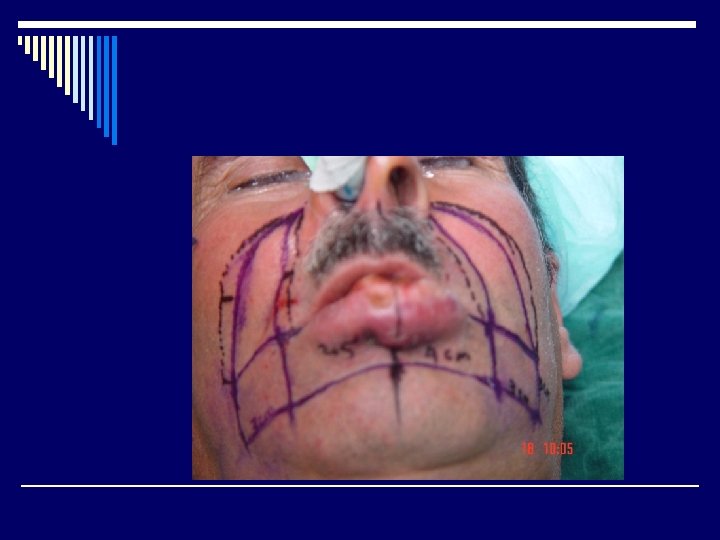
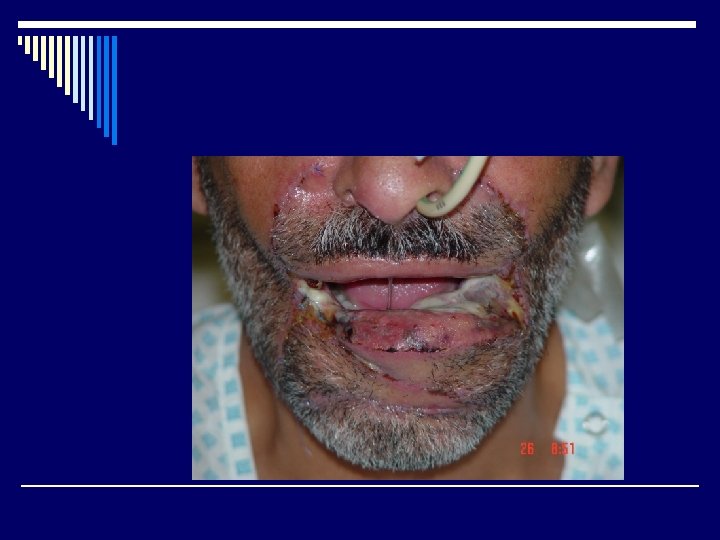
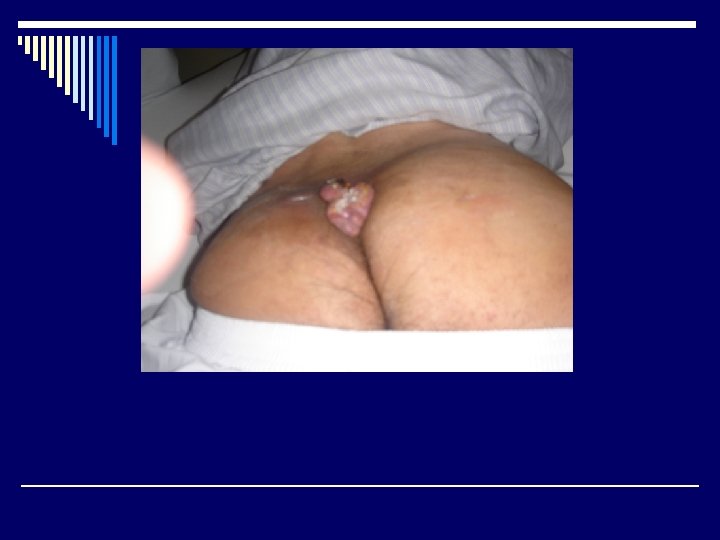
Presentation (cont. ) o Grows initially starts as a erythomatous plaque or nodule with indistinct margins. o Surface may be : - Flat - Verocous - Ulcerative o Histopathology : Malignant epithelium cell are seen extending down into the dermis like horn pearls. o Treatment : - Surgery -Radiation
Types of Nevi o Junctional Nevi: o Are small , circumscribed , light brown or black , flat – slightly raised & rarely contained hair o Mainly lies between dermis & epidermis these may be found in mucous membrane , genitalia , soles & palms
Intradermal Nevi o Small spots , color range from blue to bluish black o Flat & dome shaped o Compound found in both dermis and epidermis
Dysplastic Nevi (5 -12 mm) o Pink base with indistinctive irregular edges o Family Hx important , suspicious lesions must be excised. o Congenital : Excess in 1% of newborn , most lesions are small o Considered to be pre cancerous
Malignant Melanoma o Incidence over 300, 000 new cases skin tumors every year in USA. 9000 are melanomas, that is 4. 6 % o 2/3 of all deaths of skin tumors are from melanomas. o Incidence of melanomas is increasing & 5 year survival also inc. from 41% - 67% o Men= Women o White > Black
MELANOMA (cont. ) o Etiology - Ultra violet increase risk -Familial Hx has been recognized o Average person has 15 -20 nevi o 1/3 of all melanomas arise from pigment nevi.
Factors which suggest melanoma from mole o Color : focal shades with red blue or white. A o o o darkening in colours Size : recent rapid enlargement in dia. > 10 mm Shape: irregular margins , notchening and indentations Surface: ulceration s bleeding or crusting irregular elevation Symptoms: pruritis , inflamation and pain Location : back lower extamities neck (BANS)
Classification of Melanoma based on Histology o Superficial spreading : most common type especialy from pre-existing mole Common in back & both sexes o Nodular melanoma becomes large and ulcerated before noticed o Cartigo melanoma : most common occur in old age
CLARKS CLASSIFICATION LEVEL %OF RM 1 INSITU ABOVE 0 BASMENTMEMBRANE 2 INVASION OF PAPILLERY DERMIS 4% 3 FILLING PAPILLARY AREA AND EXTENDING TO THE JUNCTION OF 33 4 PAPILLARY AND RETICULAR AREA INTO RETICULAR LEYER OFDERMIS 61 5 SUBCUTANIOUS TISSUE 78
HIGH RISK AREAS AND POOR SYRVIVAL RATE o. B : o A: o. N o. S BACK POS. LAT OF ARM POS LAT NECK SCALP
PROPHYLACTIC NODE DISSECTION o LEVEL 1 AND 2 NO NODE DISSECTION o LEVEL 3 ? ? ? o LEVEL 4 AND 5 PROPHYLACTIC NODE DISSECTION
NODE DISSECTION NOT ADVISED IN LYPHATIC DRAINAGE MORE THAN ONE AREA PATIENT AGE > 70 YEARS SERIOUS CONCURRENT DISEASE UNRESECTABLE DISTANT METASTISIS
PROGNOSIS MOST IMPORTANT SIZE OF TUMOUR AND DEPTH OF INVASION o LESS THAN 2 CM DIAMETER ANDLESS THAN 0. 7 MM DEPTH. o CURABLE BY WIDE LOCAL EXCISION. o NODULAR MELENOMAS WITH UNCERATION POOR PROGNOSIS, LESSION IN EXTRAMITIES BETTER , PROGNOSIS THAN TRUNK o WOMEN BETTER 5 YRS SURVIVAL THAN MEN
• NON SURGICAL TREATMENT (IMMUNOTHERAPY) o TREATMENT SMALL METASTISIS BCG NOT SUITABLE FOR LARGE LESSIONS o MELANOMA RADIO RESISTANT RARELY USED FOR DEFINITE TRAETMENT MAYBE USED FOR PALIATION o CHEMOTHARAPY WITH PHENYLIN & ALAMINE MUSTURED AND OTHER DRUGS FOR SURVIVAL AND LIMB PRESERVATIONS LONG TERM PALIATION TT LARE LEGION SURGERY , RADIO THERAPY AND CHEMOTHERAPY