Skeletal Muscle Physiology Muscular System Functions Body movement

Skeletal Muscle Physiology
 Maintenance of posture Respiration Diaphragm and intercostal contractions")
Muscular System Functions Body movement (Locomotion) Maintenance of posture Respiration Diaphragm and intercostal contractions Communication (Verbal and Facial) Constriction of organs and vessels Peristalsis of intestinal tract Vasoconstriction of b. v. and other structures (pupils) Heart beat Production of body heat (Thermogenesis)

Properties of Muscle Excitability: capacity of muscle to respond to a stimulus Contractility: ability of a muscle to shorten and generate pulling force Extensibility: muscle can be stretched back to its original length Elasticity: ability of muscle to recoil to original resting length after stretched

Types of Muscle Skeletal Attached to bones Makes up 40% of body weight Responsible for locomotion, facial expressions, posture, respiratory movements, other types of body movement Voluntary in action; controlled by somatic motor neurons Smooth In the walls of hollow organs, blood vessels, eye, glands, uterus, skin Some functions: propel urine, mix food in digestive tract, dilating/constricting pupils, regulating blood flow, In some locations, autorhythmic Controlled involuntarily by endocrine and autonomic nervous systems Cardiac Heart: major source of movement of blood Autorhythmic Controlled involuntarily by endocrine and autonomic nervous systems

Connective Tissue Sheaths Connective Tissue of a Muscle Epimysium. Dense regular c. t. surrounding entire muscle Separates muscle from surrounding tissues and organs Perimysium. Collagen and elastic fibers surrounding a group of muscle fibers called a fascicle Endomysium. Loose connective tissue that surrounds individual muscle fibers Collagen fibers of all 3 layers come together at each end of muscle to form a tendon or aponeurosis.

Nerve and Blood Vessel Supply Motor neurons stimulate muscle fibers to contract Capillary beds surround muscle fibers Muscles require large amts of energy Extensive vascular network delivers necessary oxygen and nutrients and carries away metabolic waste produced by muscle fibers

Muscle Tissue Types

Skeletal Muscle Long cylindrical cells Many nuclei per cell Striated Voluntary Rapid contractions

Basic Features of a Skeletal Muscle attachments Most skeletal muscles run from one bone to another One bone will move – other bone remains fixed Origin – less movable attachment Insertion – more movable attachment
 Muscles attach to origins and insertions")
Basic Features of a Skeletal Muscle attachments (continued) Muscles attach to origins and insertions by connective tissue Fleshy attachments – connective tissue fibers are short Indirect attachments – connective tissue forms a tendon or aponeurosis Bone markings present where tendons meet bones Tubercles, trochanters, and crests
, connective tissue, blood vessels, nerves Fibers")
Skeletal Muscle Structure Composed of muscle cells (fibers), connective tissue, blood vessels, nerves Fibers are long, cylindrical, and multinucleated Tend to be smaller diameter in small muscles and larger in large muscles. 1 mm- 4 cm in length Develop from myoblasts; numbers remain constant Striated appearance Nuclei are peripherally located

Muscle Attachments

Antagonistic Muscles

Microanatomy of Skeletal Muscle

Parts of a Muscle

Motor Unit: The Nerve-Muscle Functional Unit A motor unit is a motor neuron and all the muscle fibers it supplies The number of muscle fibers per motor unit can vary from a few (4 -6) to hundreds (1200 -1500) Muscles that control fine movements (fingers, eyes) have small motor units Large weight-bearing muscles (thighs, hips) have large motor units

Motor Unit: The Nerve-Muscle Functional Unit Muscle fibers from a motor unit are spread throughout the muscle Not confined to one fascicle (bundle of skeletal muscle fibers surrounded by perimysium) Therefore, contraction of a single motor unit causes weak contraction of the entire muscle Stronger and stronger contractions of a muscle require more and more motor units being stimulated (recruited)

Motor Unit All the muscle cells controlled by one nerve cell

Power Output: The Most Physiologically Relevant Marker of Performance Power = work / time = force x distance / time = force x velocity Peak power obtained at intermediate loads and intermediate velocities. Figure from Berne and Levy, Physiology Mosby—Year Book, Inc. , 1993.

Three Potential Actions During Muscle Contraction: • shortening Biceps muscle shortens during contraction Isometric-muscle does not change its length • isometric • lengthening Biceps muscle lengthens during contraction Most likely to cause muscle injury

Recall The Motor Unit: motor neuron and the muscle fibers it innervates Spinal cord • The smallest amount of muscle that can be activated voluntarily. • Gradation of force in skeletal muscle is coordinated largely by the nervous system. • Recruitment of motor units is the most important means of controlling muscle tension. • To increase force: 1. Recruit more M. U. s 2. Increase freq. (force –frequency) Since all fibers in the motor unit contract simultaneously, pressures for gene expression (e. g. frequency of stimulation, load) are identical in all fibers of a motor unit.

Increased use: strength training Early gains in strength appear to be predominantly due to neural factors…optimizing recruitment patterns. Long term gains almost solely the result of hypertrophy i. e. increased size.
 Performance Declines with Aging --despite maintenance of physical activity 100")
Performance (% of peak) Performance Declines with Aging --despite maintenance of physical activity 100 80 60 40 Shotput/Discus Marathon Basketball (rebounds/game) 20 0 10 20 30 40 50 60 Age (years) D. H. Moore (1975) Nature 253: 264 -265. NBA Register, 1992 -1993 Edition

Number of motor units declines during aging AGE-ASSOCIATED ATROPHY DUE TO BOTH… Individual fiber atrophy (which may be at least partially preventable and reversible through exercise). Loss of fibers (which as yet appears irreversible). Campbell et al. , (1973) J Neurol Neurosurg Psych 36: 74 -182.

Motor unit remodeling with aging Central nervous system AGING Motor neuron loss Muscle Fewer motor units • More fibers/motor unit •

Mean Motor Unit Forces: • FF motor units get smaller in old age and decrease in number • S motor units get bigger with no change in number • Decreased rate of force generation and POWER!! Maximum Isometric Force (m. N) 225 200 Adult Old 175 150 125 100 75 50 25 0 FF FI FR Motor Unit Classification S Kadhiresan et al. , (1996) J Physiol 493: 543 -552.

Muscle injury may play a role in the development of atrophy with aging. • Muscles in old animals are more susceptible to contractioninduced injury than those in young or adult animals. • Muscles in old animals show delayed and impaired recovery following contraction-induced injury. • Following severe injury, muscles in old animals display prolonged, possibly irreversible, structural and functional deficits.

Disorders of Muscle Tissue Muscle tissues experience few disorders Heart muscle is the exception Skeletal muscle – remarkably resistant to infection Smooth muscle – problems stem from external irritants

Disorders of Muscle Tissue Muscular dystrophy – a group of inherited muscle destroying disease Affected muscles enlarge with fat and connective tissue Muscles degenerate Types of muscular dystrophy Duchenne muscular dystrophy Myotonic dystrophy

Disorders of Muscle Tissue Myofascial pain syndrome – pain is caused by tightened bands of muscle fibers Fibromyalgia – a mysterious chronic-pain syndrome Affects mostly women Symptoms – fatigue, sleep abnormalities, severe musculoskeletal pain, and headache

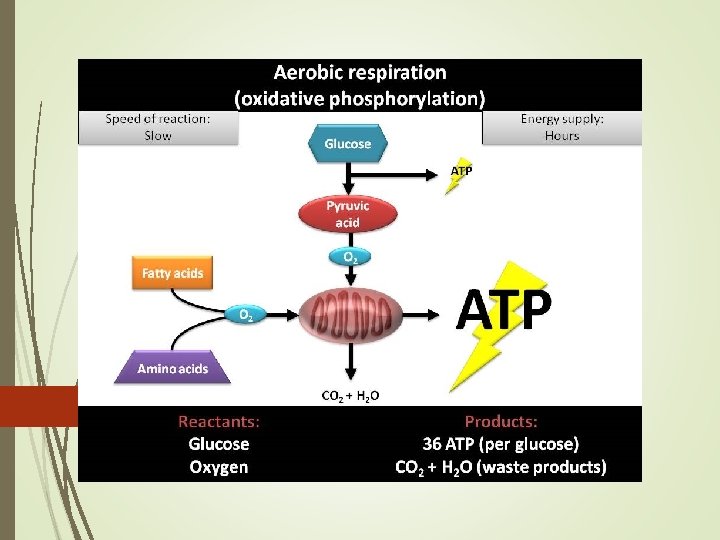
Aerobic Respiration Needs oxygen for respiration Glucose + Oxygen Carbon Dioxide + Water + Energy=ATP

ATP

Anaerobic Respiration Without oxygen for respiration Glucose Lactic Acid + Energy Incomplete breakdown of glucose 5% of energy released by aerobic respiration Lactic Acid-produces an oxygen debt because oxygen is needed to oxidize lactic acid (liver) REST
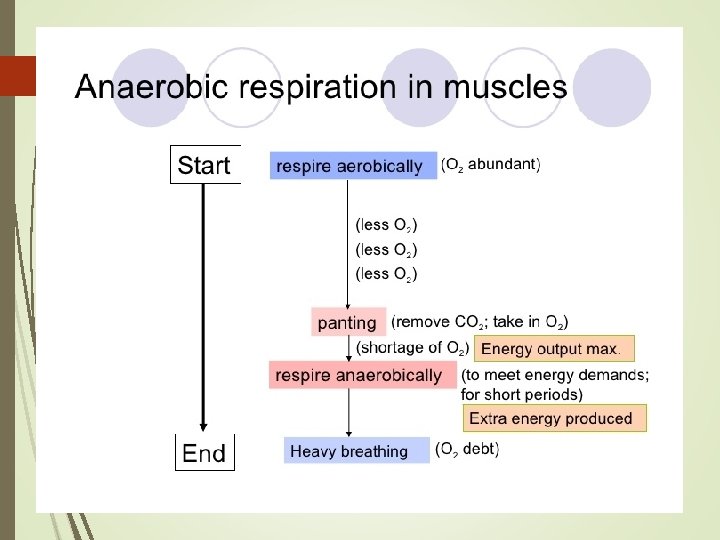

Muscle Fatigue Lack of oxygen causes ATP deficit Lactic acid builds up from anaerobic respiration

Muscle Fatigue

Muscle Atrophy Weakening and shrinking of a muscle May be caused Immobilization Loss of neural stimulation

Muscle Hypertrophy Enlargement of a muscle More capillaries More mitochondria Caused by Strenuous exercise Steroid hormones

Steroid Hormones Stimulate muscle growth and hypertrophy

Muscle Tonus Tightness of a muscle Some fibers always contracted

Tetany Sustained contraction of a muscle Result of a rapid succession of nerve impulses

Tetanus

Refractory Period Brief period of time in which muscle cells will not respond to a stimulus

Refractory

Refractory Periods Skeletal Muscle Cardiac Muscle

Isometric Contraction Produces no movement Used in Standing Sitting Posture

Isotonic Contraction Produces movement Used in Walking Moving any part of the body

Muscle Spindle

Muscle Spindle Responses

Alpha / Gamma Coactivation

Golgi Tendon Organs

Developmental Aspects: Regeneration Cardiac and skeletal muscle become amitotic, but can lengthen and thicken Myoblast-like satellite cells show very limited regenerative ability Cardiac cells lack satellite cells Smooth muscle has good regenerative ability There is a biological basis for greater strength in men than in women Women’s skeletal muscle makes up 36% of their body mass Men’s skeletal muscle makes up 42% of their body mass

Developmental Aspects: Male and Female These differences are due primarily to the male sex hormone testosterone With more muscle mass, men are generally stronger than women Body strength per unit muscle mass, however, is the same in both sexes

Developmental Aspects: Age Related With age, connective tissue increases and muscle fibers decrease Muscles become stringier and more sinewy By age 80, 50% of muscle mass is lost (sarcopenia) Decreased density of capillaries in muscle Reduced stamina Increased recovery time Regular exercise reverses sarcopenia
- Slides: 57