Sistem Syaraf dan Nyeri Apakah nyeri itu Sensori




 Afferent Neurons")









 Mendeskripsikan mekanisme faktor psikologik yang memengaruhi rasa")




















- Slides: 40
Sistem Syaraf dan Nyeri
Apakah nyeri itu? Sensori dan perasaan tidak menyenangkan dan pengalaman emosional terkait kerusakan jaringan. ◦ ◦ NOSISEPSI NYERI SUFFERING Perilaku Nyeri senantiasa bersifat subyektif Merupakan salah satu mekanisme pertahanan diri - peringatan pada otak bahwa jaringan terancam rusak Dapat tanpa picuan kerusakan fisik. Nyeri akut membuat orang mencari pengobatan dan keluhan utama menjadi titik memulai evaluasi Nyeri kronis mungkin emosional dan membuat fisik terhambat yang mendorong terjadinya bunuh diri
Sistem Syaraf dan Nyeri
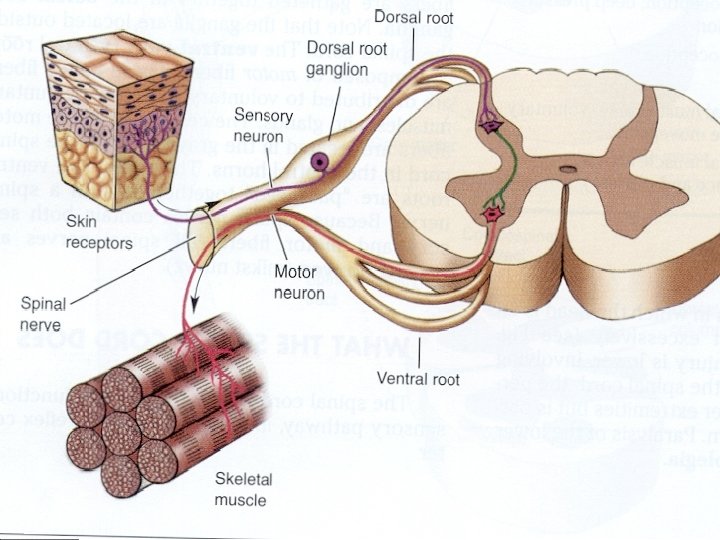
Sistem Syaraf Tepi – Tipe serabut syaraf Afferent – neuron Sensori ◦ Tiga Tipe memahami nyeri Serabut A-delta fibers – serabut syaraf kecil, bermyelin, cepat mengantar rangsang- nyeri tajam Mekanoreseptor – dipicu oleh tekanan mekanik kuat dan suhu intens Serabut C– paling kecil, tidak bermyelin, menghantar rangsang lamban, -rangsang yang diantar tumpul atau gatal. Mekanoreseptor – Mekanikal dan suhu panas Kemoreseptor – Zat kimia terlepas dari jaringan inflamasi Serabut A-beta – diameter besar, bermyelin, mengantar rangsang dengan cepat Efferent – Neuron Motor
Korda Spinal Jaras naik dan turun interneuron multiple (menghubungkan afferent & efferent) Afferent Neurons – Masuk Efferent Neurons – Keluar ke dari sisi belakang sisi ventral
Korda Spinal Lpisan Spinal s ◦ Bagian abu korda spinal dibagi atas 10 lapisan Substantia Gelatinosa ◦ Komposisinya : lapisan badan sel berjalan naik dan turun pada tanduk dorsal korda spinal ◦ Menerima asupan dari serabut A dan C -fibers ◦ Aktivitas dalam substansi abu menghambat transmisi nyeri
Otak Thalamus Kortek Somatosensori
Thalamus bagian Otak yang merupakan panel sensori switchboard Lokasinya ditengah otak
Kortek Somatosensori • Area korteks serebri di lobus parietal kanan dibelakang lobus frontal • Menerima semua informasi sentuh dan nyeri. • Organisasi somatotopik
Pain Pathways – Keatas Informasi nyeri berjalan ke korda spinal melalui traktus spinotalamikus (2 bagian) ◦ PSTT Tnda waspada segera akan adanya trauma , tempat dan intensitasnya NSTT Lambat, mengisyaratkan nyeri, bahwa sudah terjadi kerusakan jarngan
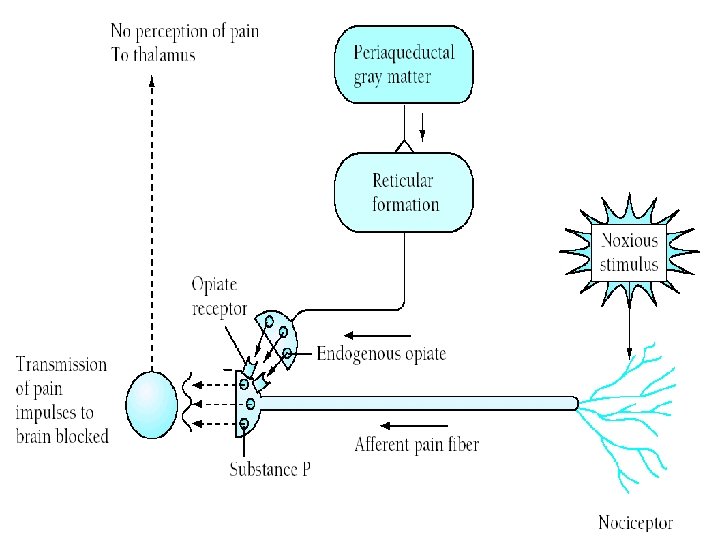
Pain Pathways – Kebawah Jaras kebawah rasa nyeri diperuntukan penghambatan nyeri
Nyeri Neurokimiawi Pain Initiators ◦ Glutamate - Central ◦ Substance P - Central ◦ Brandykinin - Peripheral ◦ Prostaglandins - Peripheral Pain Inhibitors ◦ Serotonin ◦ Endorphins ◦ Enkephalins ◦ Dynorphin
Teori Nyeri Teori Spesifitas ◦ Dimulai oleh Aristotle ◦ Nyeri itu mempunyai rangkaian Serabut 'nyeri' spesifik membawa info ke 'pusat nyeri' ◦ Ditolak pada 1965 Gate Control Theory
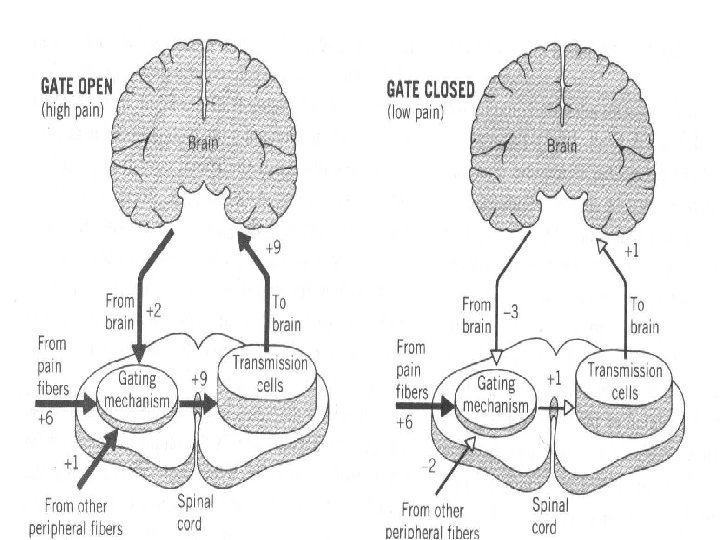
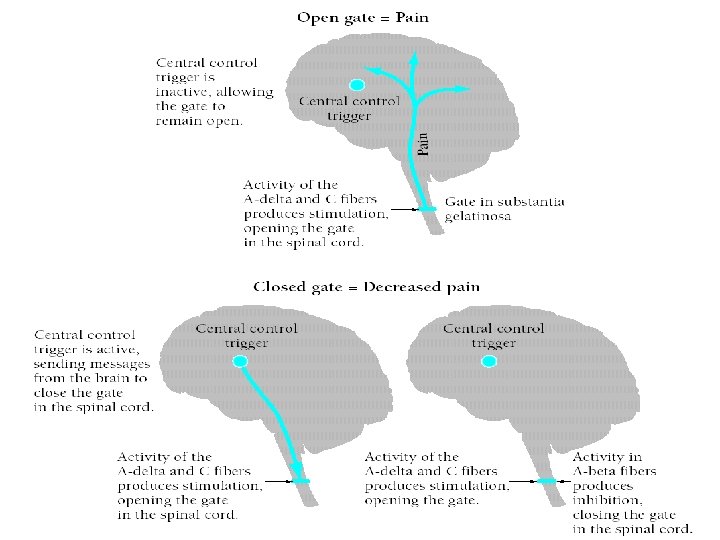
Opening and Closing the Gate When the gate is closed signals from small diameter pain fibres do not excite the dorsal horn transmission neurons. When the gate is open pain signals excite dorsal horn transmission cells
Gate-Control Theory – Ronald Melzack (1960 s) Mendeskripsikan mekanisme faktor psikologik yang memengaruhi rasa nyeri. Neural gate dapat dibuka dan ditutup dengan memodulasi nyeri. Gerbang berlokasi di korda spinal. ◦ pada substansi abu-abu
Tiga Faktor Membuka dan Menutupnya Gerbang Nyeri Jumlah serabut nyeri yang beraktivitas Jumlah serabut tepi yang beraktivitas Pesan yang diturunkan dari Otak . . .
Kondisi yang Membuka Pintu Kondisi Fisik ◦ Cedera yang meluas ◦ Level aktivitas tidak tepat Emosi dan kondisi ◦ Anxietas atau khawatir ◦ Tegang ◦ Depresi Kondisi Mental ◦ Fokus pada sakitnya ◦ Bosan
Kondisi yang Menutup Gerbang Physical conditions ◦ Medications ◦ Counter stimulation (e. g. , heat, massage) Emotional conditions ◦ Positive emotions ◦ Relaxation, Rest Mental conditions ◦ Intense concentration or distraction ◦ Involvement and interest in life activities
Categories of Pain can be categorized according to its origin: ◦ ◦ Cutaneous – Skin, tendons, ligaments Deep somatic - Bone, muscle connective tissue Visceral – Organs, cavity linings Neuropathic – Nerve pain By certain qualities ◦ Radiating ◦ Referred ◦ Intractable
Phantom Limb Pain in a absent body part Very common in amputees Ranges from tingling top sensation to pain
Acute Pain ACUTE – Pain lasting for less than 6 months ◦ Highly correlated to damage ◦ Anxiety abates w/treatment ◦ De-activation often helpful
Chronic Pain lasting > 6 months ◦ Not correlated to tissue damage ◦ Learned/Reinforced ◦ Often associated w/psychopathology or coping problems ◦ More likely to abuse alcohol and drugs ◦ Leads to shutting down ◦ Typically does not respond to drugs very well ◦ Activity is the best medicine
Measuring Pain Physiological ◦ Unreliable Self-report ◦ Behavioral observations ◦ Rankings ◦ Pain questionnaires ◦ Psych tests
Headaches Tension - Muscular ◦ Daily hassles and perfectionism predict frequency and duration of headaches (Hons & Dewey, 2004) Migraine – Muscular and vascular ◦ Neuroticism scores predict migraines for females, but not males. ◦ Abbate-Daga et. Al, (2007) 105 Migrane w/out aura vs. 79 health controls Migraine group greater than controls on Depression Anger management Overcontrol Harm-avoidance, persistence and lower in self-directedness
Back Pain 80% of US residents experience LBP Many causes, but only 20% have definite identification Burns (2006) ◦ Chronic LBP ◦ Induced anger and sadness Anger tightened LB muscles in CLBP not C Sadness did not have and effect No effect found in other muscles
MANAGING PAIN Medical and Psychosocial Approaches
Multiple Sites of Control
Medical Treatments for Pain Non-opiate Analgesics Act peripherally NSAIDS COX inhibitors Advil, Vioxx, Aleve Steroidal Drugs Suppress immune system Cortisone, Prednisone
Medical Treatments for Pain Opiate Analgesics Act centrally via endogenous opiate system ◦ Short-acting ◦ Long-acting Problems ◦ Tolerance ◦ Dependence
Medical Treatments for Pain Skin Stimulation Massage ◦ Great as an adjunct TENS ◦ Mixed results Acupuncture ◦ Effective for a number of types of pain ◦ Reduces the need for meds
Medical Treatments for Pain Surgery to reduce pain ◦ Brain surgery – ablate thalamus ◦ For intractable pain (cancer) Surgery to restore function ◦ Surgery for merely pain relief should be avoided Back Carpal Tunnel
Psychosocial Interventions to Improve Coping w/Pain Hypnosis Biofeedback Relaxation Training Behavior Modification Cognitive Therapy/CBT Multimodal Approaches
Relaxation Training Variety of techniques utilizing relaxation, distraction and re-focusing Generally Effective and Cheap ◦ Progressive Muscle Relaxation ◦ Meditative Relaxation ◦ Mindfulness Meditation ◦ Guided Imagery
Behavior Modification Programs Selectively reinforce new and more adaptive coping behaviors ◦ Exercise ◦ Activities ◦ Communication In regards to pain - extinguish pain behavior
Cognitive Therapy/CBT CT = Reappraisal + Coping Skills and Emotional Expression … CBT = CT + Behavior Mod ◦ Inoculation Training (CBT) Conceptualization Skill acquisition and rehearsal Application and follow-through Overall CT & CBT Effective for many conditions ◦ Table in your book LBP Recurrent Abdominal Pain Rheumatoid Arthritis Many more