Simplifying Serial Lesion Assessment Justin Davies MBBS Ph

Simplifying Serial Lesion Assessment Justin Davies, MBBS, Ph. D Interventional Cardiologist Hammersmith Hospital, Imperial College London CRT, 2017

Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner have had a financial interest/arrangement or affiliation with the organization(s) listed below. Affiliation/Financial Relationship Grant/Research Support Consulting Fees/Honoraria Royalty Income Intellectual Property Rights Company Volcano Philips

How would you treat? Patient 1 Patient 2

FFR and i. FR interpretation is easy? No GO FFR >0. 81 i. FR >0. 89 GO FFR <=0. 80 i. FR <=0. 89

How would you treat? DIFFUSE • Diffuse atheroma • Often no clear landing zone • Likely small increase in flow FOCAL • Atheroma present • Often clear landing zone • Likely large increase in flow

FFR in serial lesion assessment • Not possible to independently and reliabily interrogate tandem lesions • 3 -5 beat averaging means unable to demarcate beginning-end of stenosis • Not possible to visualize some stenoses

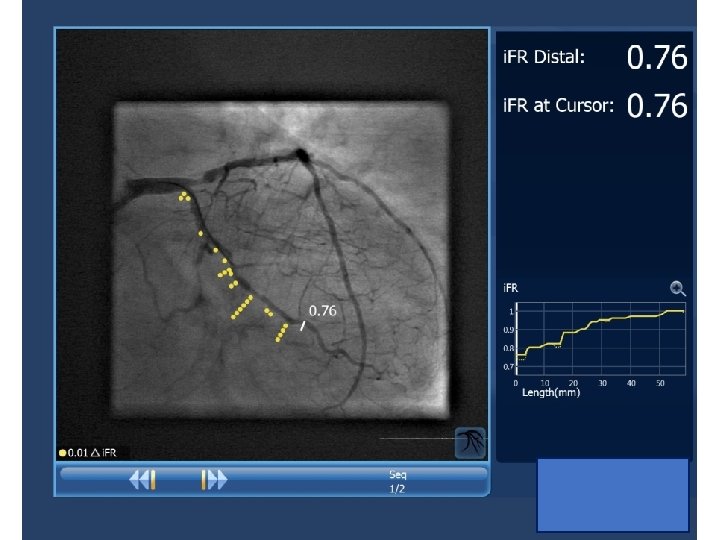
i. FR Scout used to identify the physiological most significant lesion

i. FR Scout used to identify the physiological most significant lesion FFR Pullback ( IV adenosine infusion) FFR 0, 35 i. FR Pullback (no adenosine required)

SOLUTION TO PROBLEM Complex Time Consuming Must balloon at least one stenosis Overestimate predicted pressure gradient Not work if more than 2 stenoses

Coronary Flow Hyperemic Flow x Rest Flow Increase in hyperemic flow after PCI Minimal change in rest flow after PCI Stenosis severity Pre-PCI Post-PCI Adapted from Nijjer Sukhinder

IFR PULLBACK STUDY 0. 78 ± 0. 03 Predicted i. FR: 0. 94 ± 0. 01 Observed i. FR: 0. 93 ± 0. 03 p=0. 48 Difference between virtual and measured post-PCI i. FR Pre-PCI i. FR: Nijjer SS, Davies J et al JACC: Cardiovascular Interventions. 2014; 7: 1386– 1396

PREDICTION OF IFR USING IFR-SCOUT Pre Xience Xpedition 2. 75 x 48 Xience Prime 2. 75 x 23 Post 1 st PCI Post 2 nd PCI

Future of physiological evaluation: Serial lesion assessment i. FR Co-Registration CT-FFR

CASE 1 – Hammersmith Hospital • 75 Male • 6 month history of chest pain • Presented with NSTEMI • Troponin positive • Preserved LV systolic function • Normal Labs

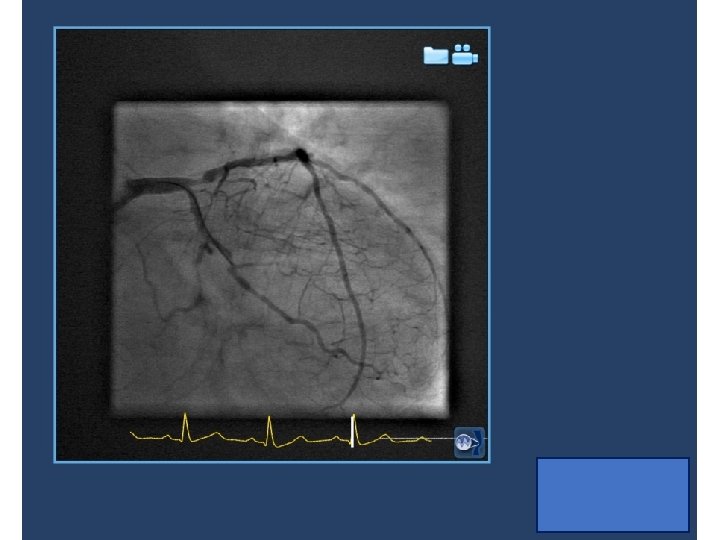
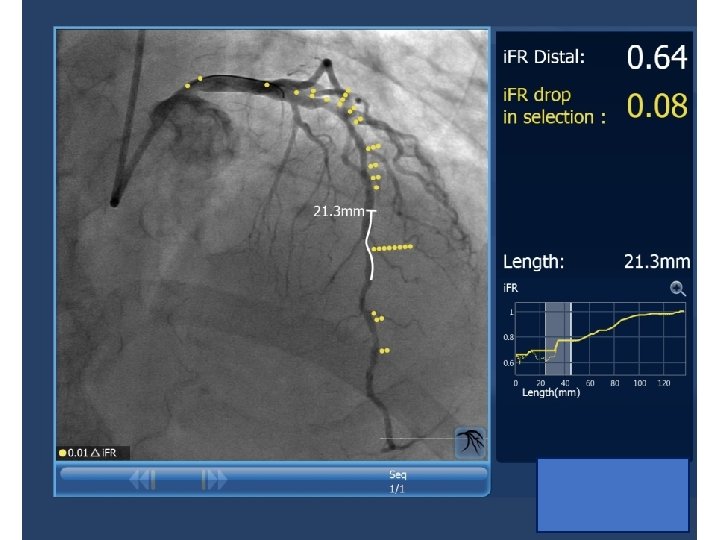
Is there a focal LAD lesion to treat?

Is there a focal LAD lesion to treat?

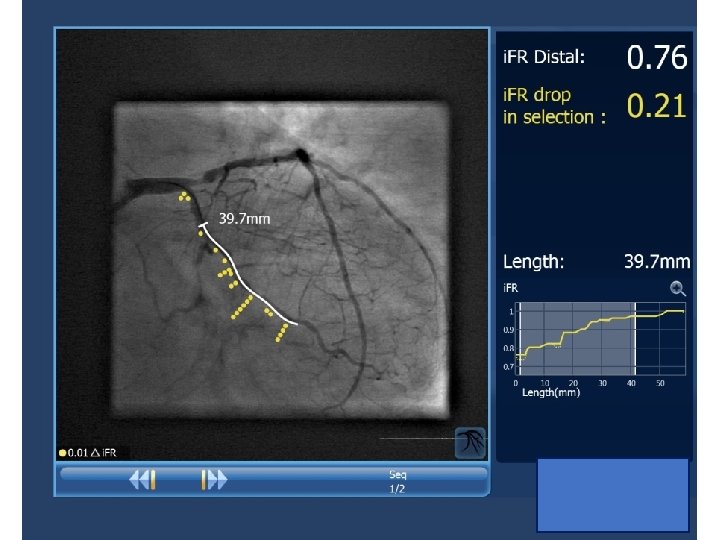
Yes- focal lesion present

Calibrated length

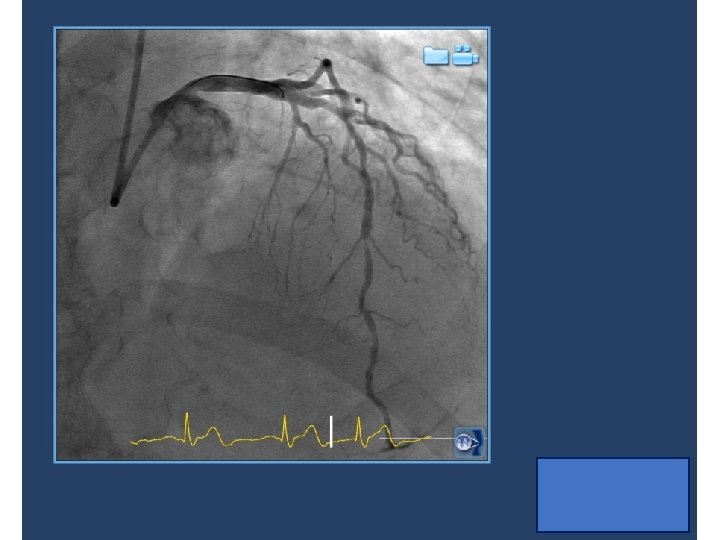
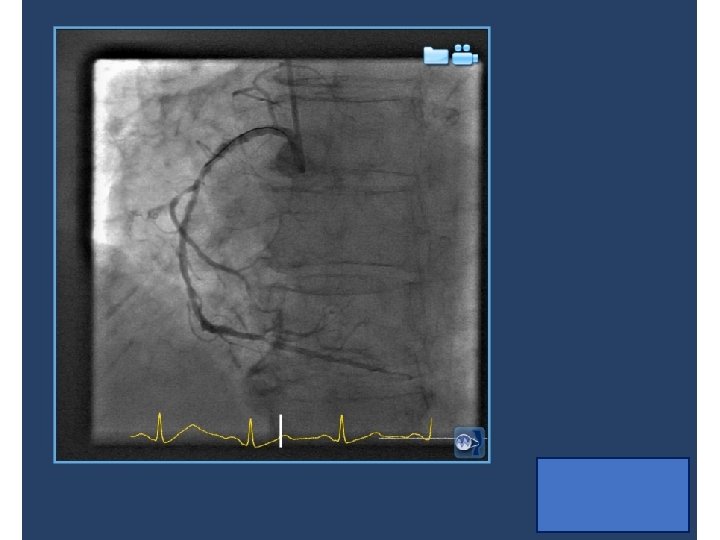
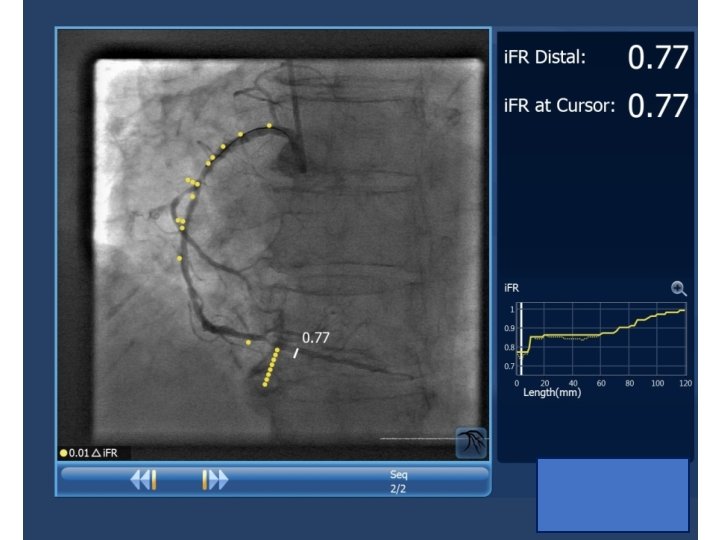
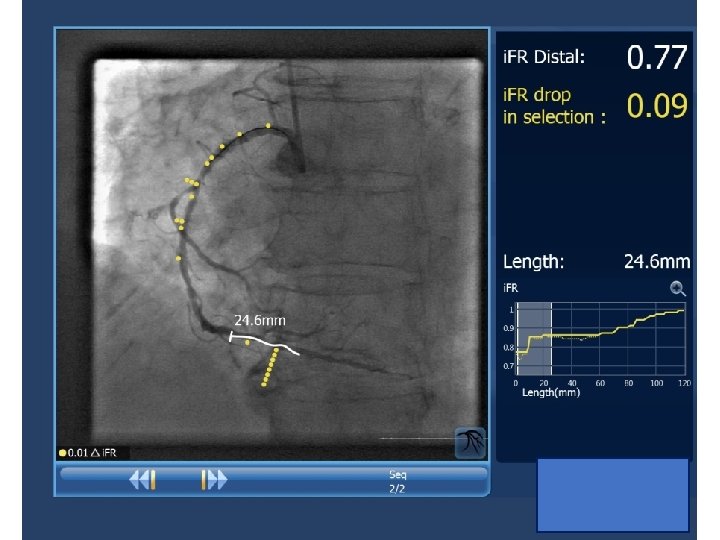
CASE 2 – Hammersmith Hospital • 65 Male • 2 month history of chest pain • Presented with Stable CAD • Troponin negative • Preserved LV systolic function • Normal Labs

Learning points 1. Complex coronary disease requires differentiation between diffuse and focal disease 2. i. FR and i. FR Co-Registration enables serial stenoses to be interrogate

Learning points 3. Predict the likely improvement in physiology prior to PCI 4. Better targeted stenting 5. Greater angina relief
- Slides: 29