Signs of Inadequate Breathing Slower than 12 breathsmin

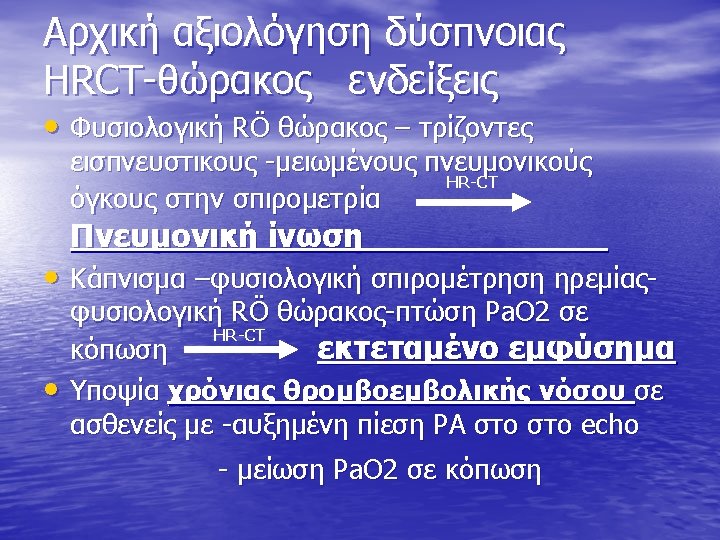
Signs of Inadequate Breathing • Slower than 12 breaths/min or faster than 20 breaths/min • Unequal chest expansion • Decreased breath sounds • Muscle retractions • Pale or cyanotic skin • Cool, damp (clammy) skin • Shallow or irregular respirations • Pursed lips • Nasal flaring

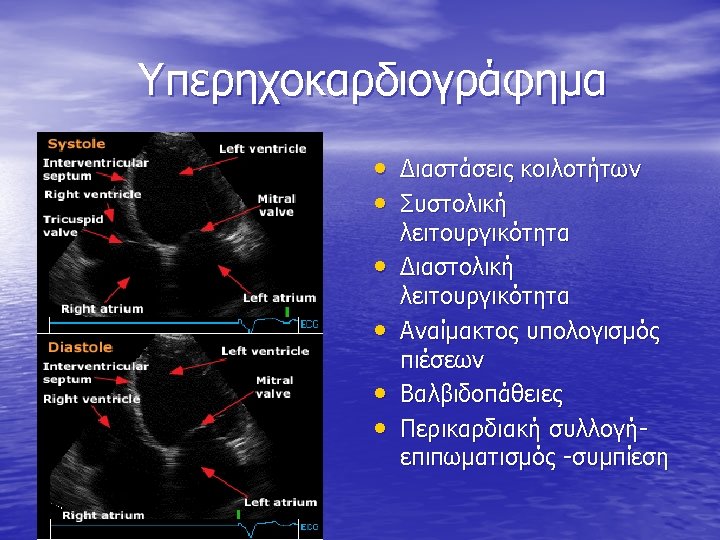
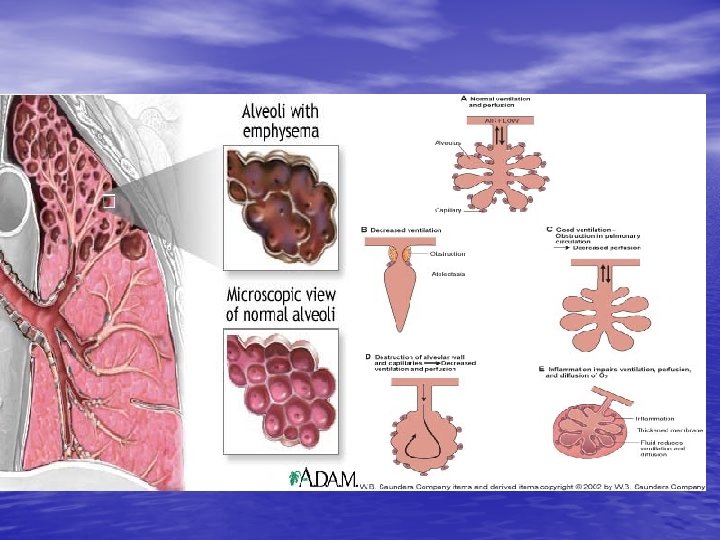
Anatomy and Function of the Lung • Pulmonary vessels • • become obstructed. Alveoli are damaged. Air passages are obstructed. Blood flow to the lungs is obstructed. Pleural space is filled


Οξεια δύσπνοια Απόφραξη αεροφόρων οδών • Be prepared to treat quickly. • Obstruction may result from the position of head, the tongue, aspiration of vomitus, or a foreign body. • Opening the airway with the head tilt-chin lift maneuver may solve the problem.

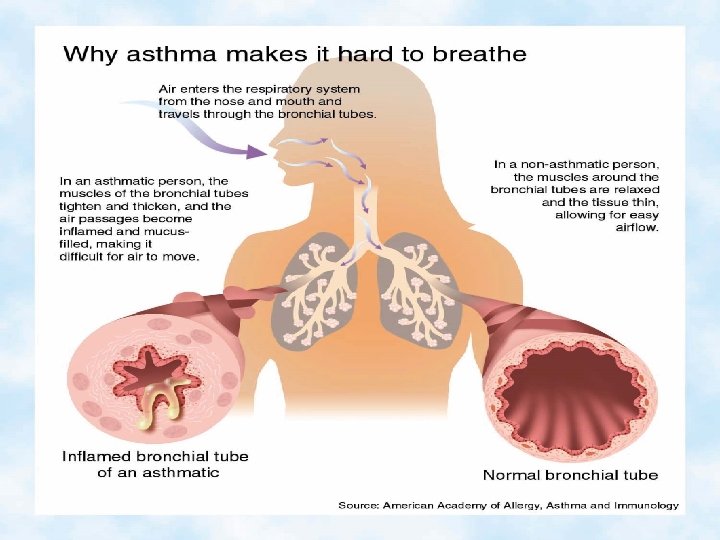
Anaphylactic Reactions • An allergen can trigger an asthma attack. • Asthma and anaphylactic (allergic) reactions can be similar. • Hay fever is a seasonal response to allergens.

Asthma • Common but serious disease • Asthma is an acute spasm of the bronchioles. • Wheezing may be audible without a stethoscope.
 • • pulmonary edema An acute inflammatory lung injury")
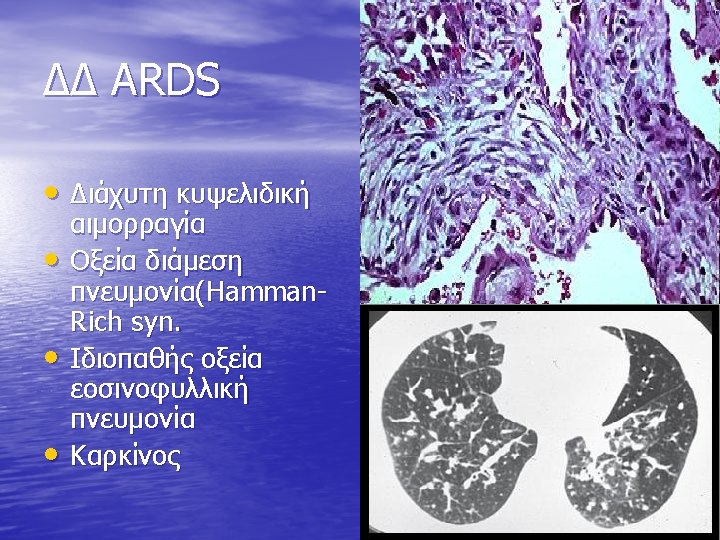
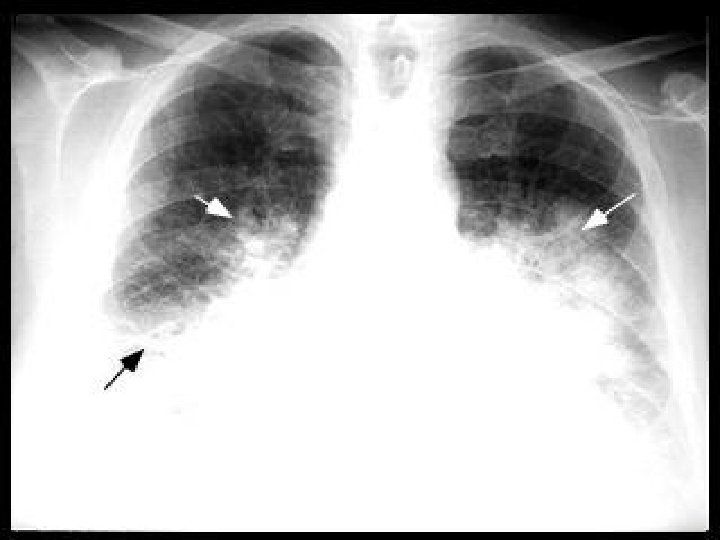
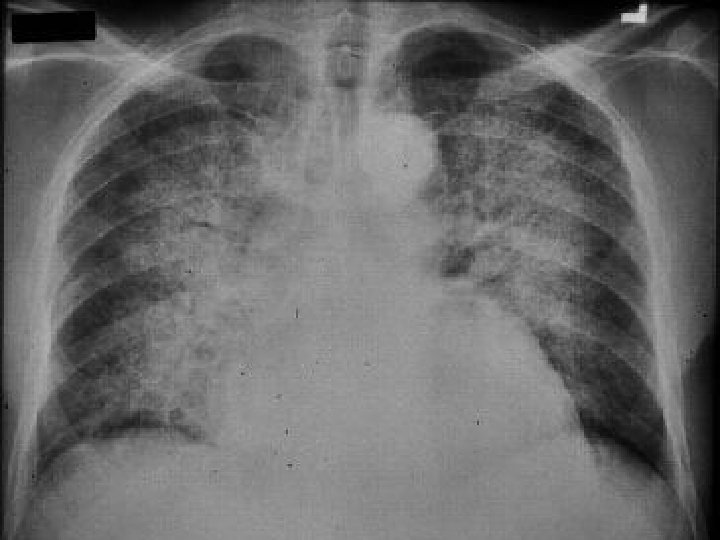
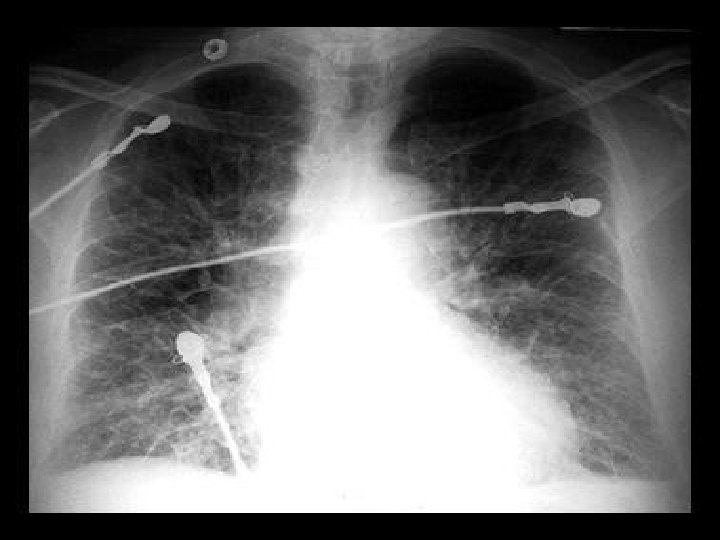
ARDS • Non-cardiogenic (low pressure) • • pulmonary edema An acute inflammatory lung injury in response to a variety of insults Acute inflammatory phase – Cytokine activated neutrophils and monocyes adhere to alveolar epithelium releasing inflammatory mediators and proteolytic enzymes – This damages the alveolar capillary membrane, increasing the permeability and causing alveolar edema – Alveolar collapse occurs from reduced surfactant – Hypoxemia/respiratory failure occur from loss of functioning alveoli and V/Q mismatch • Fibroproliferative phase – Progressive pulmonary fibrosis – Pulmonary hypertension

ARDS -Αίτια • Direct pulmonary causes – – – Infection Pulmonary trauma Near drowning Toxic gas inhalation Oxygen toxicity Gastric aspiration • Indirect causes – – – Sepsis Non-thoracic trauma Burns Hemorrhage Multiple transfusions Post arrest Bowel infarction Anaphylaxis Pancreatitis Uremia, toxins, eclampsia Drugs

BNP- Brain Natriuretic Peptide • BNP is a peptide found in blood derived from cardiac • pro-BNP Belongs to a family of hormones called the NATRIURETIC PEPTIDES – released by the ventricles of the heart in defence against the increase in blood pressure and blood volume overload seen in Heart Failure (HF) – increases sodium excretion (natriuresis) and fluid excretion (diuresis) – reduces concentration of hormones that cause blood vessel constriction (example: angiotensin, endothelin ) – Protect against collagen acumulation and pathologic remodeling 36

• Box Plots Showing Median Levels of B-Type Natriuretic Peptide among • Patients in Each of the Four New York Heart Association Classifications. Boxes show interquartile ranges, and I bars represent highest and lowest values. 37

BNP levels correlate with Left Ventricular Ejection Fraction Patients with LVEF greater than 55%had lower BNP levels than those with LVEF less than 40% Valli et al. Clin Chim Acta 2001; 306: 19 -26 38

Limitations of use of BNP 1. Only 30% of patients with BNP above 95 centile of normals have LV systolic dysfunction. Bayer have data on normals which form basis of reference group data – A RAISED BNP DOES NOT EQUAL HEART FAILURE & THE BNP CAN BE NORMAL IN RX HF 2. patients often present with concomitant disorders, such as pneumonia and decompensated heart failure. Thus, a very high concentration of BNP, although specific for decompensated heart failure, does not exclude presence of other important diseases –CLINICAL ACUMEN 3. patients with chronic HF might have persistently high BNPs despite adequate treatment, accurate diagnosis might require comparison with the patient's baseline BNP concentration, rather than use of a predetermined diagnostic threshold -SERIAL MEASUREMENTS 4. BNP levels reduce when treated aggressively so existing patient (e. g. primary care) on ACE etc may have relatively normal BNPs but still have abnormal echo – CHASE BNP DOWN 5. BNP levels vary from day to day in stable HF by up to 20% so a change from 400 to 500 would not be significant but 200 to 700 would 6. Levels of BNP were similar in patients with sepsis and th; ose with decompensated HF 7. Finally, when considering use of BNP to screen patients who are asymptomatic, doctors should recognise that the normal range of BNP is specific to age, sex, renal function and assay – BEWARE NORMAL RANGE 40
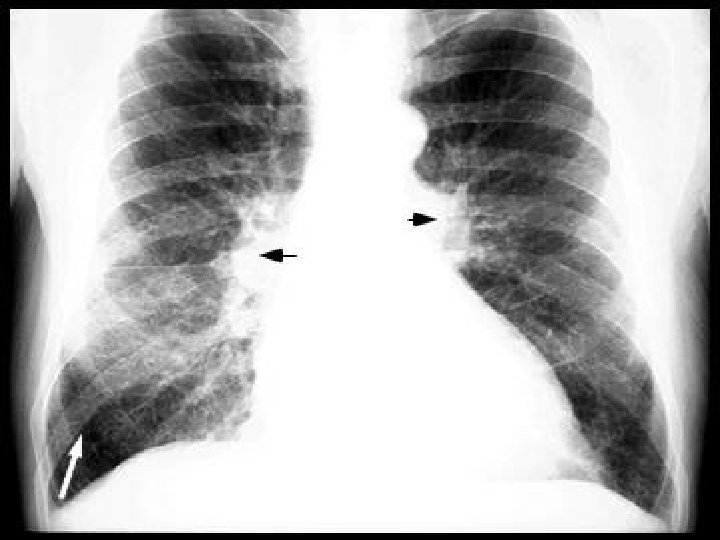
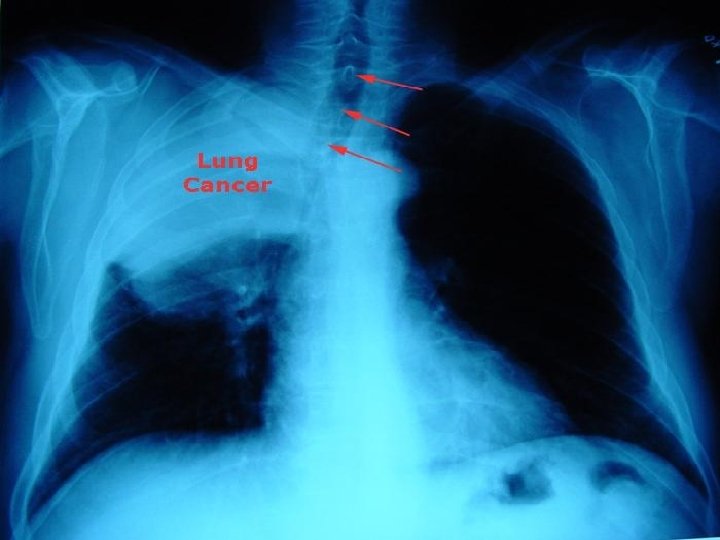

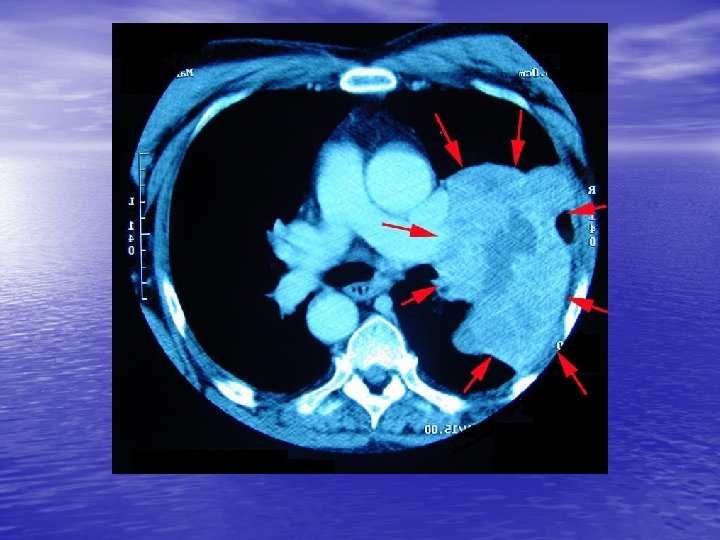
Pleural Effusion • Collection of fluid outside lung • Causes dyspnea • Caused by irritation, infection, or cancer • Decreased breath sounds over region of the chest where fluid has moved the lung away from the chest wall • Eased if patient is sitting up

Hyperventilation • Overbreathing resulting in a decrease in the level of carbon dioxide • Signs and symptoms – Anxiety – Numbness – A sense of dyspnea despite rapid breathing – Dizziness – Tingling in hands and feet
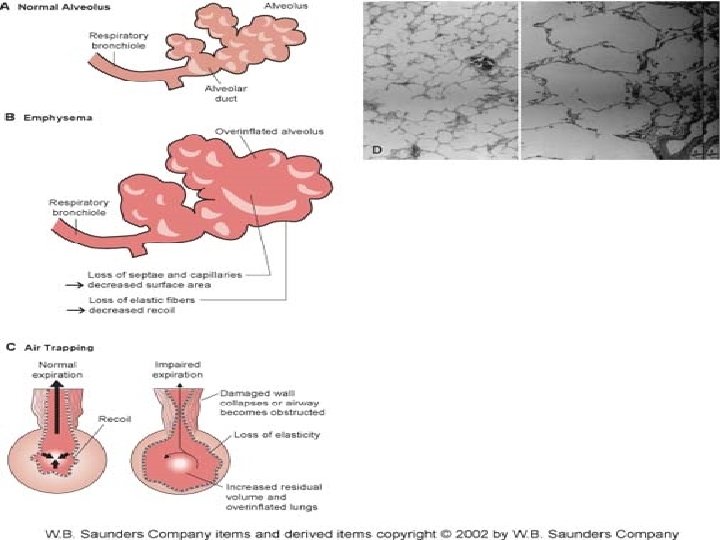
 • COPD is the result of direct lung and")
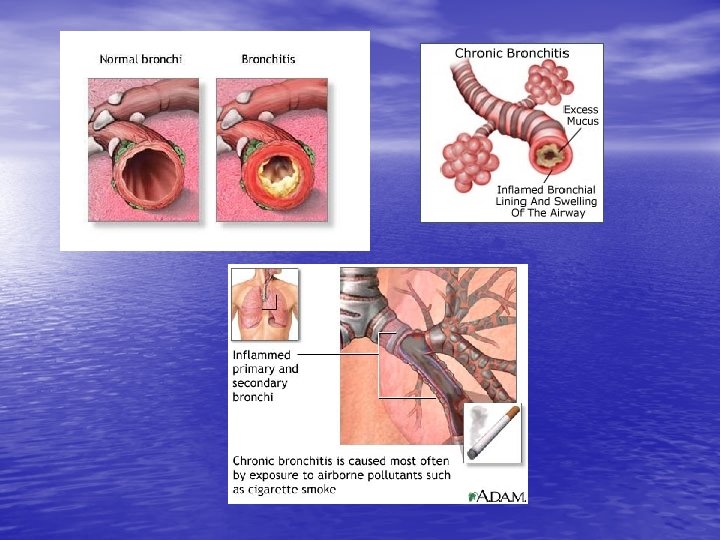
Chronic Obstructive Pulmonary Disease (COPD) • COPD is the result of direct lung and airway damage from repeated infections or inhalation of toxic agents. • Bronchitis and emphysema are two common types of COPD. • Abnormal breath sounds may be present. – Rhonchi and wheezes

From NICE HF guideline 2003 64

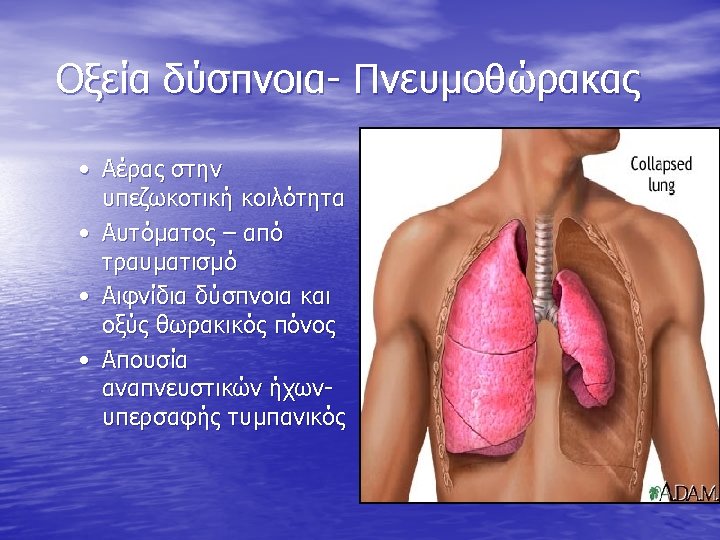
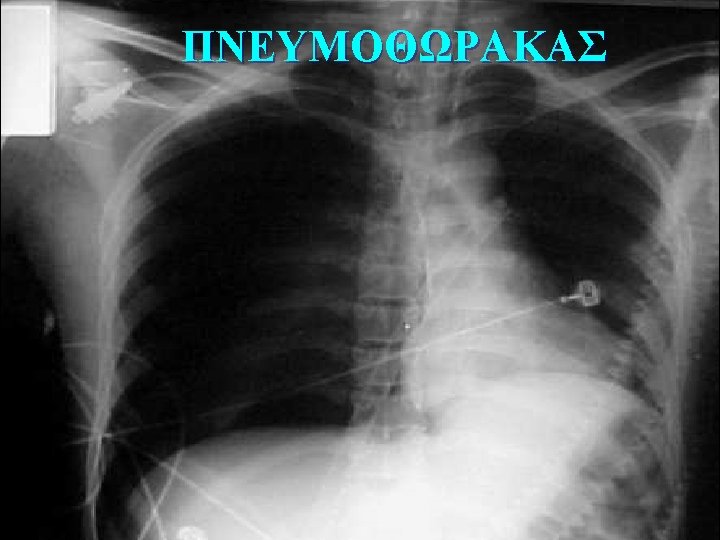
ΠΝΕΥΜΟΘΩΡΑΚΑΣ healthlibrary. epnet. com

Respiratory System

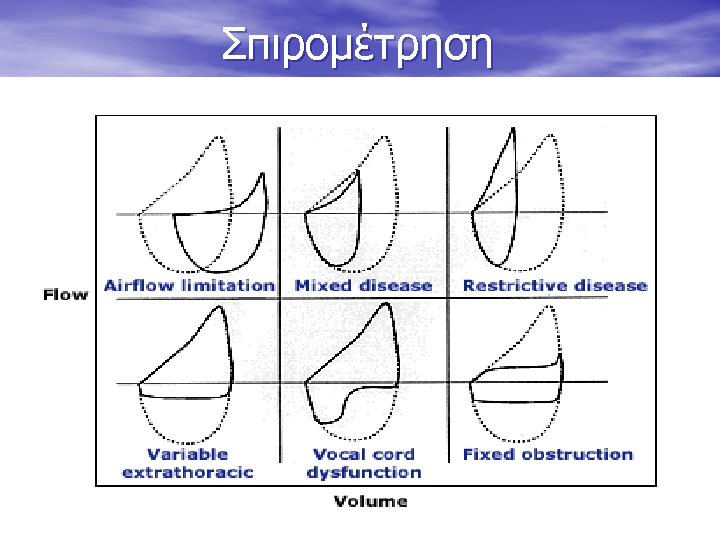
Pathophysiology of Breathing Scano and Ambrosino Lung 2002


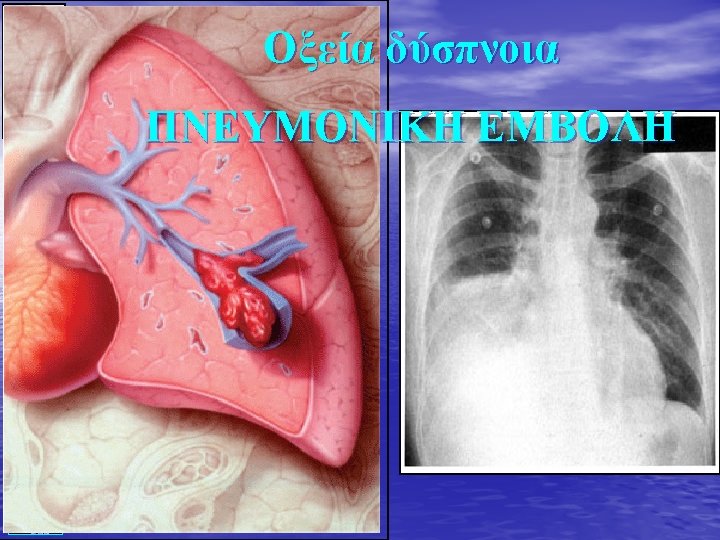
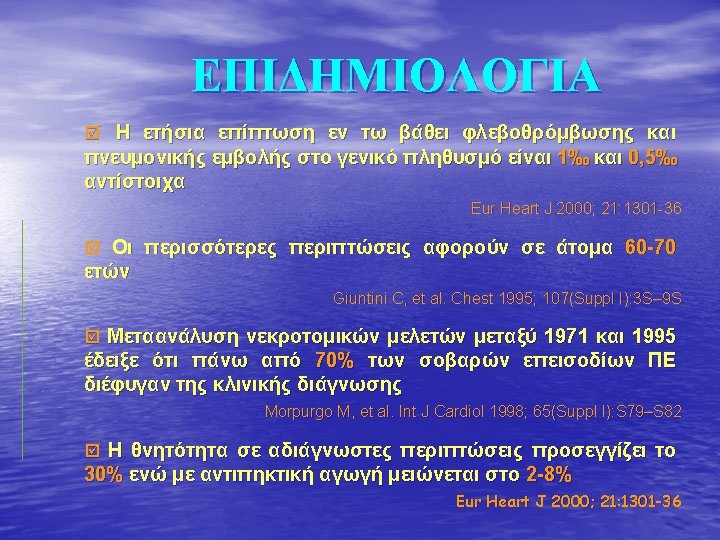
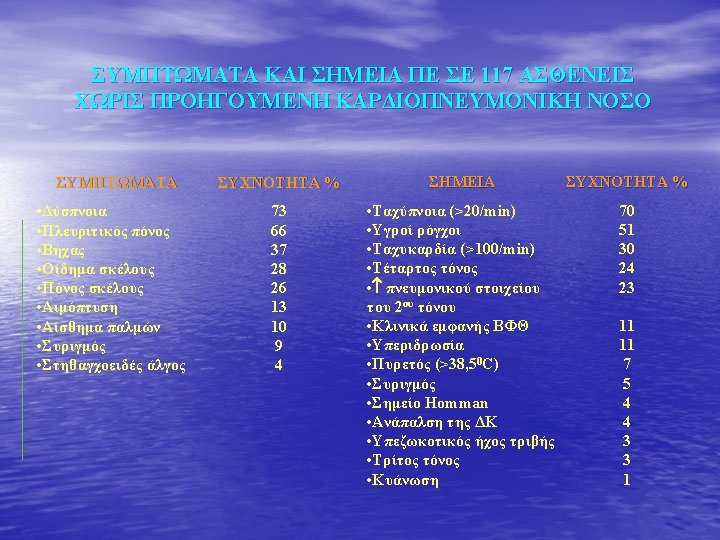
Pulmonary Embolism • A blood clot that breaks off and circulates through the venous system • Signs and symptoms – Dyspnea – Acute pleuritic pain – Hemoptysis – Cyanosis – Tachypnea – Varying degrees of hypoxia

- Slides: 77