Sigmoid Colon Rectum Dr Abeera Sarfraz Dr Muhammad

Sigmoid Colon & Rectum Dr Abeera Sarfraz / Dr Muhammad Zubair
")
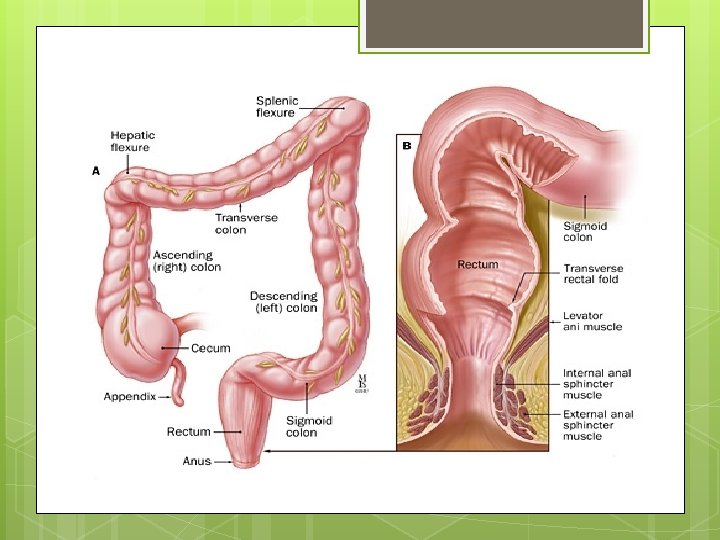
Sigmoid Colon The sigmoid colon is 10 to 15 in. (25 to 38 cm) long and begins as a continuation of the descending colon in front of the pelvic brim. It is continuous with the rectum below in front of the third sacral vertebra. The sigmoid colon is mobile and hangs down into the pelvic cavity in the form of a roughly S-shaped loop. The fan-shaped sigmoid mesocolon attaches it to the posterior pelvic wall.

Relations Anteriorly: In the male, the urinary bladder. In the female, the posterior surface of the uterus and the upper part of the vagina. Posteriorly: The rectum and the sacrum. The sigmoid colon is also related to the lower coils of the terminal part of the ileum.

Blood Supply Sigmoid branches of the inferior mesenteric artery supply the sigmoid colon. The accompanying veins drain into the inferior mesenteric vein, which joins the portal venous system. Lymph Drainage : The lymph drains into nodes along the course of the sigmoid arteries. From these nodes, the lymph travels to the inferior mesenteric nodes. Nerve Supply : The sympathetic and parasympathetic nerves from the inferior hypogastric plexuses
 long and begins in front")
RECTUM The rectum is about 5 in. (13 cm) long and begins in front of the third sacral vertebra as a continuation of the sigmoid colon. It passes downward, following the curve of the sacrum and coccyx, and ends in front of the tip of the coccyx by piercing the pelvic diaphragm and becoming continuous with the anal canal. The lower part of the rectum is dilated to form the rectal ampulla.

The rectum deviates to the left but quickly returns to the median plane. On lateral view, the rectum follows the anterior concavity of the sacrum before bending downward and backward at its junction with the anal canal. The puborectalis portion of the levator ani muscles forms a sling at the junction of the rectum with the anal canal and pulls this part of the bowel forward, producing the anorectal angle. The peritoneum covers the anterior and lateral surfaces of the first third of the rectum and only the anterior surface of the middle third, leaving the lower third devoid of peritoneum.

The muscular coat of the rectum is arranged in the usual outer longitudinal and inner circular layers of smooth muscle. However, the three teniae coli of the sigmoid colon come together so that the longitudinal fibers form a broad band on the anterior and posterior surfaces of the rectum. The mucous membrane of the rectum, together with the circular muscle layer, forms two or three semicircular permanent folds called the transverse folds of the rectum. They vary in position.

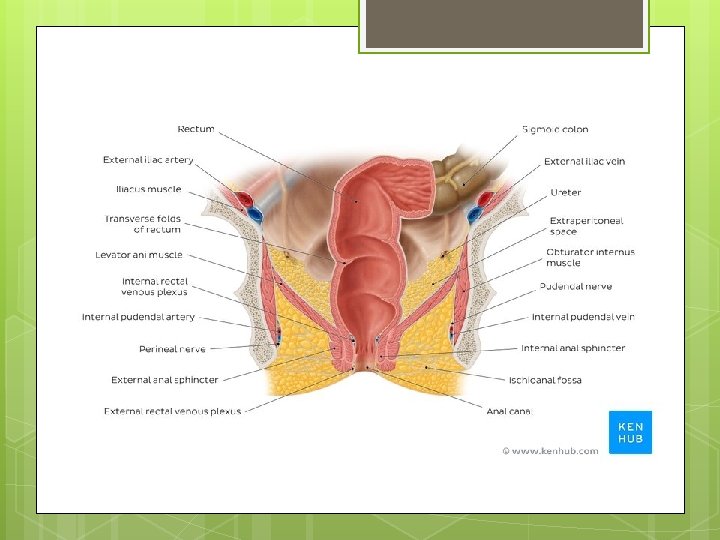
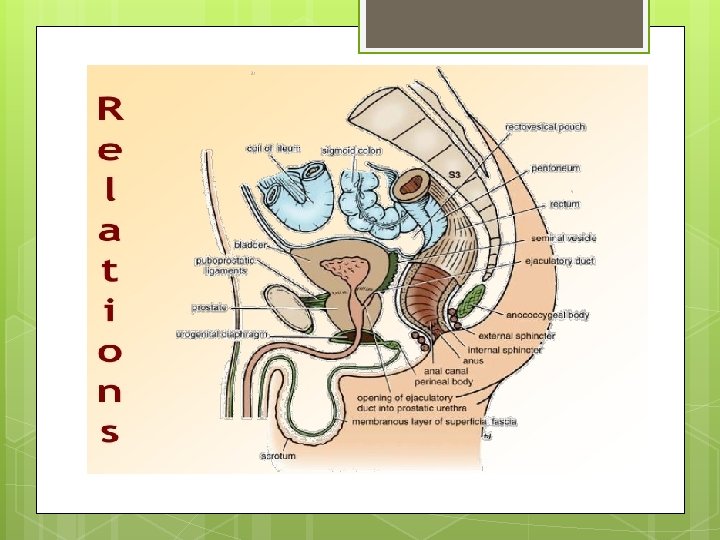
Relations Posteriorly: The rectum is in contact with the sacrum and coccyx; the piriformis, coccygeus, and levatores ani muscles; the sacral plexus; and the sympathetic trunks. Anteriorly: In the male, the upper two thirds of the rectum, which is covered by peritoneum, is related to the sigmoid colon and coils of ileum that occupy the rectovesical pouch. The lower third of the rectum, which is devoid of peritoneum, is related to the posterior surface of the bladder, to the termination of the vas deferens and the seminal vesicles on each side, and to the prostate. In the female, the upper two thirds of the rectum, which is covered by peritoneum, is related to the sigmoid colon and coils of ileum that occupy the rectouterine pouch (pouch of Douglas). The lower third of the rectum, which is devoid of peritoneum, is related to the posterior surface of the vagina

Blood Supply Multiple arteries from different sources and multiple veins with different terminations provide the rectal vasculature. Both the arteries and veins anastomose freely with their neighbors. Arteries The superior, middle, and inferior rectal arteries supply the rectum. The superior rectal artery is a direct continuation of the inferior mesenteric artery and is the chief artery supplying the mucous membrane. It enters the pelvis by descending in the root of the sigmoid mesocolon and divides into right and left branches, which pierce the muscular coat and supply the mucous membrane. They anastomose with one another and with the middle and inferior rectal arteries. The middle rectal artery is a small branch of the internal iliac artery and is distributed mainly to the muscular coat. The inferior rectal artery is a branch of the internal pudendal artery in the perineum. It anastomoses with the middle rectal artery at the anorectal junction.

Veins The veins of the rectum correspond to the arteries. The superior rectal vein is a tributary of the portal circulation and drains into the inferior mesenteric vein. The middle and inferior rectal veins drain into the internal iliac and internal pudendal veins, respectively. The union between the rectal veins forms an important anorectal portal–systemic anastomosis. Lymph Drainage The lymph vessels of the upper rectum drain first into the pararectal nodes and then into inferior mesenteric nodes. Lymph vessels from the lower part of the rectum follow the middle rectal artery to the internal iliac nodes. Nerve Supply The nerve supply is from the sympathetic and parasympathetic nerves from the inferior hypogastric plexuses. The rectum is sensitive only to stretch.

Clinical Notes Sigmoid The sigmoid colon shows great variation in length and may measure as much as 36 in. (91 cm). In the young child, because the pelvis is small, this segment of the colon may lie mainly in the abdomen. Sigmoid Colon Variation in Length and Location Colon Cancer The sigmoid colon is a common site for cancer of the large bowel. Because the lymphatic vessels of this segment of the colon drain ultimately into the inferior mesenteric nodes, an extensive resection of the gut and its associated lymphatic field is necessary to extirpate the growth and its local lymphatic metastases. The colon is removed from the left colic flexure to the distal end of the sigmoid colon, and the transverse colon is anastomosed to the rectum.

Volvulus Because of its extreme mobility, the sigmoid colon sometimes rotates around its mesentery. This may correct itself spontaneously, or, the rotation may continue until the blood supply of the gut is cut off completely. The rotation commonly occurs in a counterclockwise direction and is referred to as volvulus. Diverticula of the mucous membrane along the course of the arteries supplying the sigmoid colon are a common clinical condition. In patients with diverticulitis or ulcerative colitis, the sigmoid colon may become adherent to the bladder, rectum, ileum, or ureter and produce an internal fistula.

Sigmoidoscopy Because the sigmoid colon lies only a short distance from the anus (6. 5 in. [17 cm]), examining the mucous membrane under direct vision for pathologic conditions is possible. A flexible tube fitted with lenses and illuminated internally is introduced through the anus and carefully passed up through the anal canal, rectum, sigmoid colon, and descending colon. This examination, called sigmoidoscopy, can be carried out without an anesthetic in an outpatient clinic. Biopsy specimens of the mucous membrane can be obtained through this instrument. Relevant Anatomic Facts The patient is placed in the left lateral position with the left knee flexed and the right knee extended. Alternatively, the patient is placed kneeling in the knee–chest position. The sigmoidoscope is gently inserted into the anus and anal canal in the direction of the umbilicus to ensure that the instrument passes along the long axis of the canal. Gentle but firm pressure is applied to overcome the resistance of the anal sphincters. After a distance of about 1. 5 in. (4 cm), the instrument enters the ampulla of the rectum. At this point, the tip of the sigmoidoscope should be directed posteriorly in the midline to follow the sacral curve of the rectum. Slow advancement is made under direct vision. Some slight side-toside movement may be necessary to bypass the transverse rectal folds.
 from the anal margin, the rectosigmoid")
At ~6. 5 in. (16. 25 cm) from the anal margin, the rectosigmoid junction will be reached. The sigmoid colon here bends forward and to the left, and the lumen appears to end in a blind cul-de-sac. To negotiate this angulation, the tip of the sigmoidoscope must be directed anteriorly and to the patient’s left side. This maneuver can cause some discomfort in the anal canal from distortion of the anal sphincters by the shaft of the sigmoidoscope. Another possibility is that the point of the instrument may stretch the wall of the colon, giving rise to colicky pain in the lower abdomen. Once the instrument has entered the sigmoid colon, it should be possible to pass it smoothly along its full extent and, using the full length of the sigmoidoscope, enter the descending colon. The sigmoidoscope may now be slowly withdrawn, carefully inspecting the mucous membrane. The normal rectal and colonic mucous membrane is smooth and glistening and pale pink with an orange tinge, and blood vessels in the submucosa can be clearly seen. The mucous membrane is supple and moves easily over the end of the sigmoidoscope. Anatomy of Complications : Perforation of the bowel at the rectosigmoid junction can occur. This is almost invariably caused by the operator failing to negotiate carefully the curve between the rectum and the sigmoid colon. In some patients, the curve forms an acute angulation, which may frustrate the overzealous advancement of the sigmoidoscope. Perforation of the sigmoid colon results in the escape of colonic contents into the peritoneal cavity.

Colonoscopy Direct visual inspection of the lining of the entire colon including the cecum (colonoscopy) has become an important weapon in the early diagnosis of mucosal polyps and large bowel cancer. Not only can the colon be observed and suspicious areas photographed for future reference but also biopsy specimens can be removed for pathologic examination (see Fig. 7. 38). Following a regime in which the large bowel is thoroughly washed out, the patient is relaxed under a light anesthetic. The flexible endoscopic tube is introduced through the anus into the anal canal, rectum, and colon. Colonoscopy can also be used in the diagnosis and treatment of ulcerative colitis and Crohn’s disease. Colostomy The sigmoid colon is often selected as a site for performing a colostomy in patients with carcinoma of the rectum. Its mobility allows the surgeon to bring out a loop of colon, with its blood supply intact, through a small incision in the left iliac region of the anterior abdominal wall. Its mobility also makes it suitable for implantation of the ureters after surgical removal of the bladder.

Rectal Curves and Mucosal Folds The anteroposterior flexure of the rectum, as it follows the curvature of the sacrum and coccyx, and the lateral flexures must be remembered when one is passing a sigmoidoscope to avoid causing the patient unnecessary discomfort. The crescentic transverse mucosal folds of the rectum must also be borne in mind when passing an instrument into the rectum. These folds likely serve to support the weight of the feces and to prevent excessive distention of the rectal ampulla. Blood Supply and Internal Hemorrhoids The chief arterial supply to the rectum is from the superior rectal artery, a continuation of the inferior mesenteric artery. In front of the third sacral vertebra, the artery divides into right and left branches. Halfway down the rectum, the right branch divides into an anterior and a posterior branch. The tributaries of the superior rectal vein are arranged in a similar manner, so that it is not surprising to find that internal hemorrhoids are arranged in three groups: two on the right side of the lower rectum and anal canal and one on the left.

Partial and Complete Rectal Prolapse Partial and complete prolapses of the rectum through the anus are relatively common clinical conditions. In partial prolapse, the rectal mucous membrane and submucous coat protrude for a short distance outside the anus. In complete prolapse, the whole thickness of the rectal wall protrudes through the anus. In both conditions, many causative factors may be involved. However, damage to the levatores ani muscles as the result of childbirth and poor muscle tone in the aged are important contributing factors. A complete rectal prolapse may be regarded as a sliding hernia through the pelvic diaphragm. Rectal Cancer (carcinoma) of the rectum is a common clinical finding that remains localized to the rectal wall for a considerable time. At first, it tends to spread locally in the lymphatics around the circumference of the bowel. Later, it spreads upward and laterally along the lymph vessels, following the superior rectal and middle rectal arteries. Venous spread occurs late, and because the superior rectal vein is a tributary of the portal vein, the liver is a common site for secondary deposits.

Once the malignant tumor has extended beyond the confines of the rectal wall, knowledge of the anatomic relations of the rectum will enable a physician to assess the structures and organs likely to be involved. In both sexes, a posterior penetration involves the sacral plexus and can cause severe intractable pain down the leg in the distribution of the sciatic nerve. A lateral penetration may involve the ureter. An anterior penetration in the male may involve the prostate, seminal vesicles, or bladder; in the female, the vagina and uterus may be invaded. It is clear from the anatomic features of the rectum and its lymph drainage that a wide resection of the rectum with its lymphatic field offers the best chance of cure. When the tumor has spread to contiguous organs and is of a low grade of malignancy, some form of pelvic evisceration may be justifiable. It is most important for a medical student to remember that the interior of the lower part of the rectum can be examined by a gloved index finger introduced through the anal canal. The anal canal is about 1. 5 in. (4 cm) long so that the pulp of the index finger can easily feel the mucous membrane lining the lower end of the rectum. Most cancers of the rectum can be diagnosed by this means. This examination can be extended in both sexes by placing the other hand on the lower part of the anterior abdominal wall. With the bladder empty, the anterior rectal wall can be examined bimanually. In the female, the placing of one finger in the vagina and another in the rectum may enable the physician to make a thorough examination of the lower part of the anterior rectal wall.

Rectal Injuries The site of penetration relative to the peritoneal covering will determine the management of penetrating rectal injuries. The upper third of the rectum is covered by peritoneum on the anterior and lateral surfaces, the middle third is covered only on its anterior surface, and the lower third is devoid of a peritoneal covering. The treatment of penetration of the intraperitoneal portion of the rectum is identical to that of the colon, because the peritoneal cavity has been violated. In the case of penetration of the extraperitoneal portion, the rectum is treated by diverting the feces through a temporary abdominal colostomy, administering antibiotics, and repairing and draining the tissue in front of the sacrum. Pelvic Appendix If an inflamed appendix is hanging down into the pelvis, abdominal tenderness in the right iliac region may not be felt, but deep tenderness may be experienced above the symphysis pubis. Rectal examination (or vaginal examination in the female) may reveal tenderness of the peritoneum in the pelvis on the right side. If such an inflamed appendix perforates, a localized pelvic peritonitis may result.
- Slides: 22