Sialadenitis Dr Ahmed Negm ass professor of general





 Ø Site: wedged between sternomastoid muscle &")
 �emerges from the anterior border �passes forward over")


 q • • • emerges from the")


 Acute bacterial (suppurative) sialadenitis 2) Mumps")
 ACUTE SUPPURATIVE SIALOADENITIS q Etiology: * Predisposing Factors: 1. Poor oral hygiene. 2.")


. II. Local→ 1.")


 Conservative: * General: rest - antibiotic - analgesics & tonics. *")

 Surgical treatment: ** Indications: - Failure of conservative treatment. - If there is")

 CHRONIC SIALO-ADENITIS ♣♣ Etiology: I. Chronic calcular sialadenitis 1. Infection: is a good")




 Plain X-Ray: most of the stones are radio opaque (may be")



 Submandibular gland (A) Stone in the Duct: a. Peeping stone from orifice")
 �usually")





- Slides: 43
Sialadenitis Dr. Ahmed Negm ass. professor of general Surgery Faculty of medicine– Mansoura University
Objectives Ø salivary glands: anatomy & physiology ØFunction of saliva. ØCauses of salivary gland enlargement (neoplastic & non-neoplastic) ØSialadenitis ØDifferential diagnosis
Introduction q. Salivary glands are exocrine glands. q. Major SG are paired structures and include the parotid, submandibular and sublingual q. Secret saliva in the mouth Ø Parotid: serous ØSubmandibular: mucous & serous Ø Sublingual: mucous
Types of salivary glands q. The Major Salivary Glands � Parotid glands. � Submandibular glands. � Sublingual glands. q. The Minor Salivary Glands � Labial & buccal glands. � Glossopalatine glands. � Palatine glands. � Lingual glands
Anatomy of major salivary glands
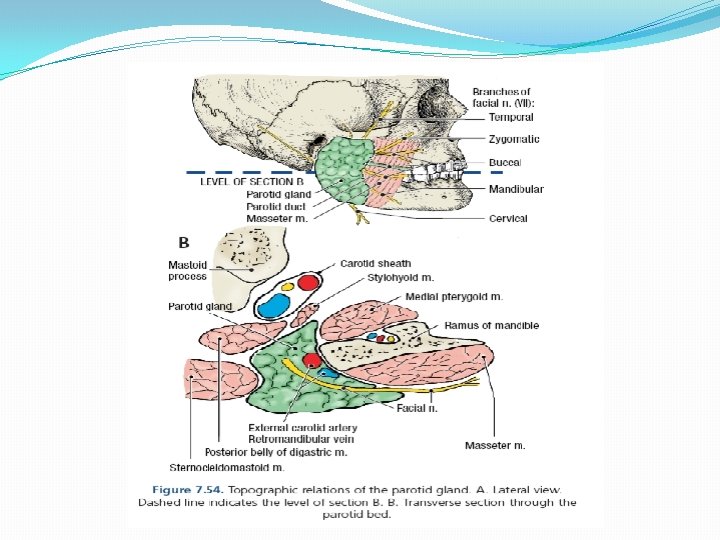
Parotid gland Ø Size: The largest(hen egg) Ø Site: wedged between sternomastoid muscle & ramus of the mandible Ø Capsule: tight fascial capsule
The parotid duct (stanson’s duct ) �emerges from the anterior border �passes forward over the masseter, �enters the vestibule of the mouth opposite the upper second molar tooth.
Structures passing through parotid gland: 1. 2. 3. Facial nerve. Retromandibular vein. External carotid artery. �It’s a pure serous gland, composed mostly of serous acini.
Submandibular gland Ø Found in the floor of the mouth; it is medial and partly inferior to the body of the mandible. Ø It is divided into superficial and deep parts by the mylohyhoid muscle.
The submandibular duct ( Wharton's duct ) q • • • emerges from the anterior end of the deep part of the gland runs forward beneath the mucous membrane of the mouth, It opens at the lingual frenulum on the floor of the mouth. Has triple relation with the lingual nerve
Sublingual gland Ø Located beneath the tongue and superior to the submandibular gland. Ø It’s ducts open into the floor of the mouth in the oral cavity. Ø It’s a mixed gland, it has both serous and mucous acini,
Function of saliva Ø Digestion : Moistens dry foods to aid swallowing. Ø Disinfectants : Salivary lysozyme, Ig. A and other antibacterial substances protect against caries and oral cavity infections. Ø Hormonal : Saliva secretes Gustin hormone which is thought to play a role in the development of taste buds.
Sialadenitis FInflammatory diseases of the salivary glands: 1) Acute bacterial (suppurative) sialadenitis 2) Mumps 3) Chronic sialadenitis 4) Post operative usually parotid 5) Autoimmune diseases
1) ACUTE SUPPURATIVE SIALOADENITIS q Etiology: * Predisposing Factors: 1. Poor oral hygiene. 2. Obstruction of salivary duct by food particles, or stone. 3. Dehydration (postoperatively). 4. Debility. * Organisms: Staph. aureus (commonest), streptococci and pneumococci * Route of Entry: 1 - Direct: either along duct from mouth (commonest). 2 - Blood borne
q. Pathology: - Site: The parotid is the commonest gland involved. - The gland duct are congested edematous and may suppurate. q Complications: 1. Abscess if it ruptures it may lead to a fistula. 2. Chronicity and stone formation. 3. Spread: a. Local to surrounding: submandibular when involved→ Ludwig’s angina. b. General: toxaemia, septicemia and pyaemia.
q Clinical Picture: I. General→ toxemic symptoms (Fever, headache etc. ). II. Local→ 1. Pain: early, dull aching, later it is severe throbbing. 2. Swelling: elevating the lobule of the ear- red- warm- edema- tender- fluctuate (late due to thicker parotid fascia) 3. Opening of the duct: red, raised, and edematous, with possible discharge. 4. restricted movement of tempro-mandibular joint
On examination: The parotid gland is tender and diffusely enlarged and purulent discharge can be seen oozing (or can be milked) from the parotid duct orifice.
q Investigations: 1. Leucocytosis 2. X-ray film may show calcifications or stones 3. U. S.
q Treatment: (1) Conservative: * General: rest - antibiotic - analgesics & tonics. * Local: hot fomentation, H 202 mouth wash, KI as sialogogue. * Observation: a. General: pulse, temperature. b. Local: swelling.
After 3 days of conservative treatment, patient either: a. Improve: continue conservative treatment till complete cure. b. Worsens: signs of suppuration (throbbing pain, hectic fever, pitting edema) → incision and drainage (Do not wait for fluctuation)
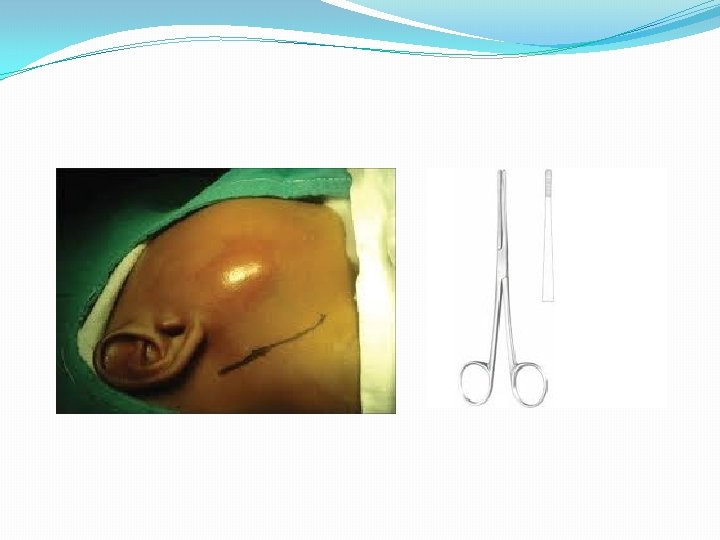
(2) Surgical treatment: ** Indications: - Failure of conservative treatment. - If there is signs of suppuration (abscess formation). ** Procedure: a. Parotid abscess: - A vertical skin incision in front of ear. - The deep fascia is incised transversely to avoid injury of the branches of facial nerve. - A sinus forceps is then introduced closed and then opened to drain the pus (Hilton’s method).
b. Submandibular abscess: - Skin incision parallel to lower border of the mandible 1. 5 inch below and in front of the angle of mandible to avoid injury of mandibular branch of facial nerve. - Incise deep fascia - A sinus forceps is then introduced closed and then opened to drain the pus (Hilton’s method).
2) CHRONIC SIALO-ADENITIS ♣♣ Etiology: I. Chronic calcular sialadenitis 1. Infection: is a good former for stones as it provides: Nucleus: through the tissue debris & bacterial colonies. Soil: ulceration of epithelium. Climate: change p. H of saliva. Manure: the exudate is sticky gluing the constituents together. Time: it causes stasis that gives time for stone formation. 2. Stasis: by sepsis, stricture. II. Chronic non calcular sialadenitis 1. Oral hygiene is poor. 2. Obstruction of salivary duct by food particles, F. B. 3. Imperfect drainage of acute sialoadenitis
♣♣ Pathology: Chronic calcular sialadenitis * Site: - Stones lie in the gland or in the duct. - Submandibular glands to parotid ratio is 50: 1. WHY? A. Secretions of submandibular are more viscid. B. Its duct opens in floor of mouth → obstruction by food particles. C. Drainage of submandibular gland is independed. * * Composition: composed of Calcium, Mg phosphate & carbonate.
q Complications: Chronic calcular sialoadenitis a. Obstruction and infection may lead to abscess & fistula formation. b. Migration: If small stone. c. Malignancy.
♣♣ Clinical Picture: ** Type of patient: male > female, occurs in middle and old age. q ** Symptoms: Pain: - Dull aching pain if the stone is in the gland or colicky pain if it is in duct - May refer to tip of the tongue or teeth due to irritation of lingual nerve as it hooks around submandibular duct - Increases with meal & mastication. Swelling: - its size is increased after meal. - Stone in submandibular duct may be felt through floor of mouth. Discharge: Bloody or even purulent discharge may be seen coming from duct.
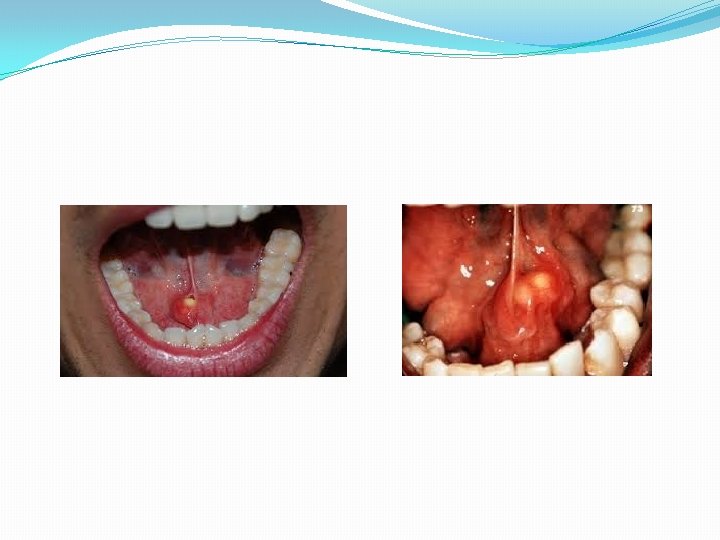
q ** Signs: Gland is enlarged, tender, • cannot be rolled over lower border of mandible (due to capsule of the gland which fix it to the mandible) • with preservation of the sulcus ( ) the gland & body of the mandible Bidigital palpation: • the gland better felt from inside the mouth Opening of duct • is seen red, raised, discharging blood or pus. • A stone may be seen peeping from the duct opening Lemon test: Pain and gland increase in size when the patient is given a lemon to suck.
♣♣ Investigations: (1) Plain X-Ray: most of the stones are radio opaque (may be hidden by mandible) (2) Sialography: A radio-opaque material as lipidol or hypaque (Na diatrizoate) 0. 5 -2 ml is injected in the canulated duct to delineate it and shows sialactasis behind stone. (3) Neck ultra-sound
x. Rays
SIALOGRAM
Differential diagnosis: Enlarged submandibular salivary gland Enlarged Subamndibular lymph node Single swelling Usually multiple Can not be rolled around mandible Can be rolled around mandible Best palpated from inside It is best palpated from outside. Duct: discharge, stone Duct: NAD +ve lemon test -ve lemon test NO 1 ry focus There is usually 1 ry focus
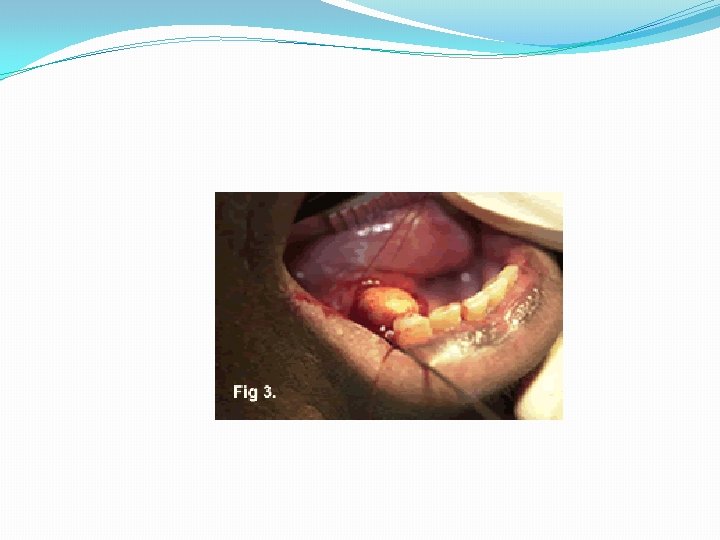
Treatment: (I) Submandibular gland (A) Stone in the Duct: a. Peeping stone from orifice → meatotomy b. Stone in the duct: - Under local anesthesia, the duct is underrun by an anchoring stitch (to avoid slippage of stone to the gland) - Slit duct open from orifice to stone. - Remove stone, and leave duct opened after removal of anchoring stitch to allow a better drainage. c. Recurrent ductal stones or associated with gland stones: Submandibular sialadenectomy (B) Stone in the gland: Submandibular sialadenectomy.
MUMPS �Viral infectious disease attack the parotid gland �incubation period (17 -21 days) �usually bilateral � occur in children.
q. Symptoms: • • • Asymptomatic Swollen, painful salivary glands on one or both sides. Pain with chewing or swallowing Fever Weakness and fatigue q: Complications of mumps are potentially serious, but rare. These include: 1. 2. 3. Orchitis Pancreatitis Meningitis
q. Treatment: • Mumps is a self-limited disease. • Treated with bed rest. • Use analgesics to relieve pain and reduce fever such as: • Acetaminophen. • Nonsteroidal anti-inflammatory drugs. • Complications may require treatment in the hospital. q. Prevention: � The most common preventative measure against mumps is immunization with a mumps vaccine.
Von Mickulicz Disease - It is autoimmune disease → enlargement of Both parotid – both submandibular- both lacrimal glands - It is precursor of lymphoma of salivary gland - The salivary glands are the seat of heavy lymphocytic infiltration - The disease responds to prednisolone - The syndrome includes also: - Narrowing of the palpebral fissure due to enlargement of lacrimal gland - Dry mouth ** Sjogren syndrome → dry mouth, dry eyes, generalized arthritis ** Sicca syndrome → dry mouth, dry eyes
Immunologic Disease Sjögren’s Syndrome 7 �Most common immunologic disorder associated with salivary gland disease. �Characterized by a lymphocyte-mediated destruction of the exocrine glands leading to xerostomia and keratoconjunctivitis sicca � 90% cases occur in women �Average of onset is 50 y �Classic monograph on the diease published in 1933 by Sjögren, a Swedish ophthalmologist
Sjögren’s Syndrome Two forms: �Primary: involves the exocrine glands only �Secondary: associated with a definable autoimmune disease, usually rheumatoid arthritis. � 80% of primary and 30 -40% of secondary involves unilateral or bilateral salivary glands swelling