Shoulder instability Alirezaafiat ir Special test Jerrek test

Shoulder instability ﻓیﺰیﻮﺗﺮﺍپیﺴﺖ ﻋﻠیﺮﺿﺎ ﻋﺎﻓیﺖ Alirezaafiat. ir

Special test: Jerrek test anterior-posterior drawer test Fulcrum test

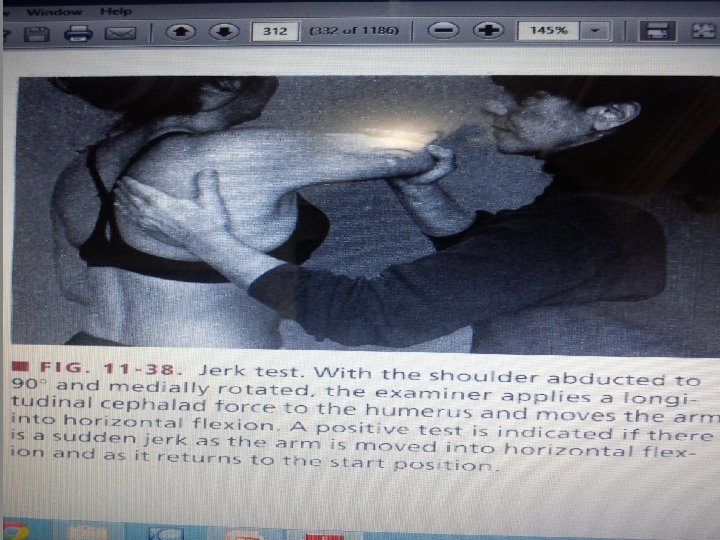
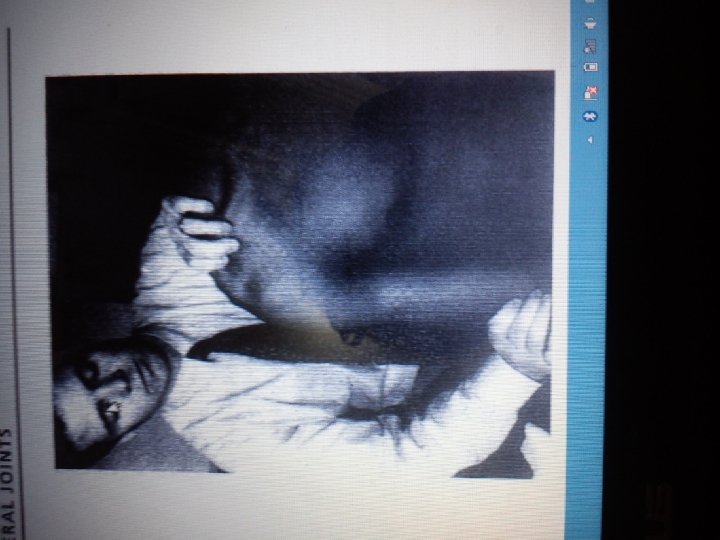
� FIG. 11 -38. Jerk test. With the shoulder abducted to 90° and medially rotated, the examiner applies a longi - tudinal cephalad force to the humerus and moves the arm into horizontal flexion. A positive test is indicated if there is a sudden jerk as the arm is moved into horizontal flex- ion and as it returns to the start position.

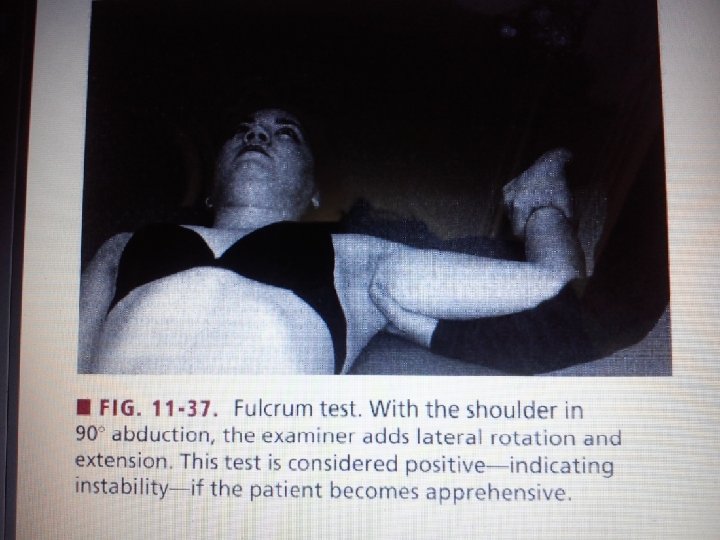
� • FIG. 11 -37. Fulcrum test. With the shoulder in 90° abduction, the examiner adds lateral rotation and extension. This test is considered positive-indicating instability-if the patient becomes apprehensive.

� FIG. 11 -39. Sulcus test. The examiner applies a longitudinal caudad force to the humerus. A positive test is indicated if the patient's pain is reproduced or a sulcus appears distal to the acromion, suggesting inferior insta- bility of the shoulder.

Common Functional Limitations/Disabilities � � � � � With rotator cuff rupture, inability to reach or lift objects to the level of horizontal, thus interfering with all activities using humeral elevation Possibility of recurrence when replicating the dislocating action With anterior dislocation, restricted ability in sports activities, such as pitching, swimming, serving (tennis, volleyball), spiking (volleyball) Restricted ability, particularly when overhead or horizontal abduction movements are required while dressing, such as putting on a shirt or jacket, and with self-grooming, such as combing the back of the hair Discomfort or pain when sleeping on the involved side in some cases With posterior dislocation, restricted ability in sports activities, such as follow-through in pitching and golf; restricted ability in pushing activities, such as pushing open a heavy door or pushing one’s self up out of a chair or out of a swimming pool

Management: Protection Phase �Activity restriction is recommended for 6 to 8 weeks �in a young patient. If a sling is used, the arm is removed �from the sling only for controlled exercise. During �the first week, the patient’s arm may be continuously �immobilized because of pain and muscle guarding.

Promote Tissue Health � Protected ROM, intermittent muscle setting of the rotator � cuff, deltoid, and biceps brachii muscles, and grade II � joint techniques (with the humerus at the side or in the � resting position) are initiated as soon as the patient tolerates � them. � P R E C A U T I O N S : In order not to disrupt healing of the � capsule and other damaged tissues after anterior dislocation, � ROM into external rotation is performed with the � elbow at the patient’s side, with the shoulder flexed in the � sagittal plane, and with the shoulder in the resting position � (in the plane of the scapula, abducted 55 and 30 to 45 � anterior to the frontal plane) but not in the 90 abducted � position. The forearm is moved from in front of the trunk � (maximal internal rotation) to 0 or possibly 10 to 15 � external rotation.

Management: Controlled Motion Phase �Provide Protection �The patient continues to protect the joint and avoid full �return to unrestricted activity. If a sling is being used, the �patient increases the time the sling is off. The sling is used �when the shoulder is tired or if protection is needed. �Increase Shoulder Mobility �Mobilization techniques are initiated using all appropriate �glides except the anterior glide.

�is contraindicated even though external rotation is necessary �for functional elevation of the humerus. For a �safe stretch to increase external rotation, the shoulder is �placed in the resting position (abducted 55 and horizontally �adducted 30); it is then externally rotated to the �limit of its range, after which a grade III distraction force �is applied perpendicular to the treatment plane in the glenoid �fossa (Fig. 17. 20). �The posterior joint structures are passively stretched with �horizontal adduction self-stretching techniques.

� � � � � � Increase Stability and Strength of Rotator Cuff and Scapular Muscles Both the internal and external rotators need to be strengthened as healing occurs. 25 The internal rotators and adductors must be strong to support the anterior capsule. The external rotators must be strong to stabilize the humeral head against anterior translating forces and to participate in the deltoid-rotator cuff force couple when abducting and laterally rotating the humerus. Scapular stability is important for normal shoulder function and to maintain the scapula in normal alignment. The following exercises are initiated. Isometric resistance exercises with the joint positioned at the side and progressed to various pain-free positions within the available ranges. Partial weight-bearing and stabilization exercises. Dynamic resistance, limiting external rotation to 50 and avoiding the position of dislocation. At 3 weeks, supervised isokinetic resistance for internal rotation and adduction at speeds of 180 per second or higher. 7 • Patient position and procedure: Standing with the arm at the side or in slight flexion and elbow flexed 90.

�The patient performs internal rotation beginning at the �zero position with the hand pointing anteriorly and �moving across the front of the body. Progress to positioning �the shoulder at 90 flexion; then perform the �exercise from zero to full internal rotation. Do not �position in 90 abduction. �By 5 weeks, all shoulder motions are incorporated into �exercises on isokinetic or other mechanical equipment �except in the position of 90 abduction with external �rotation.

Shoulder instability ﻓیﺰیﻮﺗﺮﺍپیﺴﺖ ﻋﻠیﺮﺿﺎ ﻋﺎﻓیﺖ Alirezaafiat. ir
- Slides: 29