Shoulder Dystocia District 1 ACOG Medical Student Education



 § DM/GDM (increases overall risk by")







: No fundal pressure; combination of Mc. Roberts")


 Tell the patient not to push § The training and experience")
- Slides: 17
Shoulder Dystocia District 1 ACOG Medical Student Education Module 2011
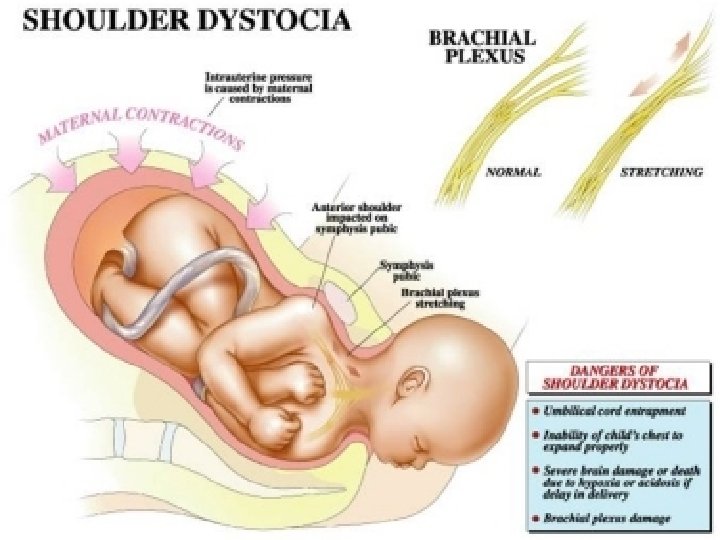
Definition § Difficulty in delivery of fetal shoulders § Failure to deliver fetal shoulder without utilizing facilitating maneuvers § Prolonged head-to-body delivery time § >60 seconds § Incidence: 0. 2 -3% of all live births; represents an obstetric emergency
Pathophysiology § Size discrepancy between fetal shoulders and maternal pelvic inlet § Macrosomia § Large chest: BPD § Absence of truncal rotation § Fetal shoulders remain A-P or descent simultaneously
Risk Factors § Antepartum § Macrosomia (>4500 g) § DM/GDM (increases overall risk by 70%) § Multiparity § Intrapartum § Prolonged deceleration phase of labor § Prolonged 2 nd stage § Protracted descent § Operative delivery (vacuum>forceps)
Risk factors cont… § No evidence based data: § Male § AMA § Short maternal stature § Abnormal pelvic shape/size
Unpredictable § 25 -50% have no defined risk factor! § 50% of cases occur in infants whose birth weight is <4000 g § 84% of patients did not have prenatal dx. of macrosomia by US § 82%of infants with brachial plexus palsy did not have macrosomia
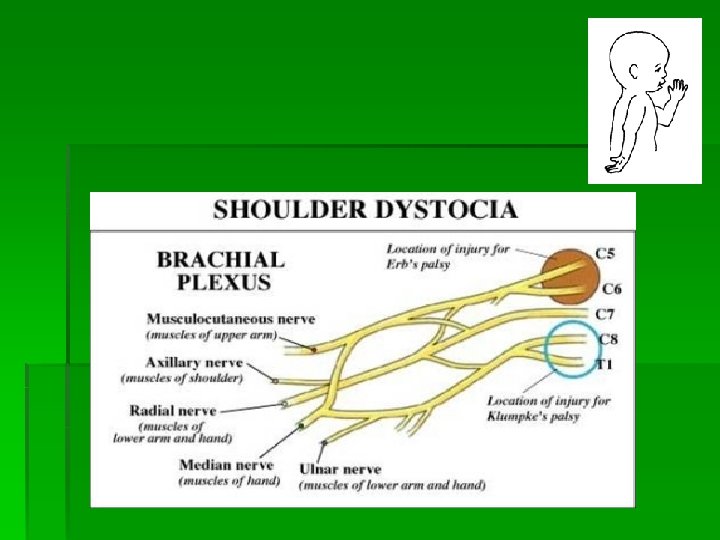
Complications § Maternal § Hemorrhage § 4 th degree laceration § Fetal § Fx of humerus or clavicle § Brachial plexus injury (Erb’s/Klumpke’s palsy) § Asphyxia/cord compression § Physician § Litigation: 11% of all obstetrical suits
Management § Goal: Safe delivery before neontal asphyxia and/or cortical injury § 7 minutes!!! § Episiotomy § Suprapubic Pressure § Mc. Roberts Maneuver § Woods or Rubin Maneuvers § Zavenelli § Push back the delivered fetal head into birth canal and perform an emergent c/s
Mc. Roberts Maneuver § 42% success rate § + Suprapubic pressure = 54 -58% § Brings pelvic inlet and outlet into more vertical alignment § Flattens sacrum § Cephalad rotation of pubic symphysis § Elevates anterior shoulder and flexes fetal spine § Increases IUP by 97% § Increases amplitude of contractions § +31 N of pushing force
Summary § Cannot accurately predict § BE PREPARED! § Consider risk factors § Be prepared to perform various maneuvers § Diagnose and treat quickly § Obtain assistance from nursing staff and NICU
HELPER Algorithm § H: Call for Help; Shoulder dystocia is called if shoulders cannot be delivered with gentle traction § E: Evaluate for Episiotomy: Not routinely indicated; maybe needed when attempting intra-vaginal maneuver § L: Legs (Mc. Roberts): Hyperflexion and abduction of hips—initial maneuver
HELPER Algorithm cont. § P (Suprapubic Pressure): No fundal pressure; combination of Mc. Roberts and suprapubic pressure resolves most shoulder dystocias § Enter (Internal Maneuvers): § Woods: Insert hand into posterior vagina and rotate posterior shoulder clockwise or counterclockwise § Rubin: Push posterior or anterior shoulder toward fetal chest to adduct shoulders § Remove: Delivery posterior arm
Prophylactic Cesarean? § Not recommended by ACOG § Exceptions: § Consider if… § >5000 g in mother without DM § >4500 g in mother with DM
Prolog Question #1 § A 25 year-old healthy woman has a normal labor and a spontaneous delivery of the fetal head. On expulsion of the head, a shoulder dystocia is recognized. Before instituting maneuvers the next step is to: § § A) Tell the patient not to push B) Apply fundal pressure C) Increase or initiate Oxytocin administration D) Cut a large episiotomy
Answer § A) Tell the patient not to push § The training and experience of clinician should dictate sequence of maneuvers that will be used; however, initially it is best to do nothing that will further impact the anterior shoulder above the pubic symphysis. The simplest way to avoid further impaction is to ask the patient to stop pushing.