SHOULDER DISLOCATION Prepared by Dr Shane Barclay OBJECTIVES

SHOULDER DISLOCATION Prepared by Dr. Shane Barclay

OBJECTIVES - Review the anatomy of the shoulder. - Review the types of shoulder dislocations. - Review the radiographic appearances of shoulder dislocations. - Be aware of complications of shoulder dislocation and from reduction. - Outline an algorithm for reductions. - Review the types of reduction procedures.

ANATOMY OF THE SHOULDER - Most mobile joint, at the expense of being most unstable. - Only 25% of humeral head is in contact with glenoid. - The glenohumeral joint is surrounded by ligaments that are overlaid by muscles/tendons (rotator cuff) - Glenohumeral ligament is primary ligament. - Rotator cuff is made up of 4 muscles: - Supraspinatus - Subscapularis - Teres minor - Infraspinatus
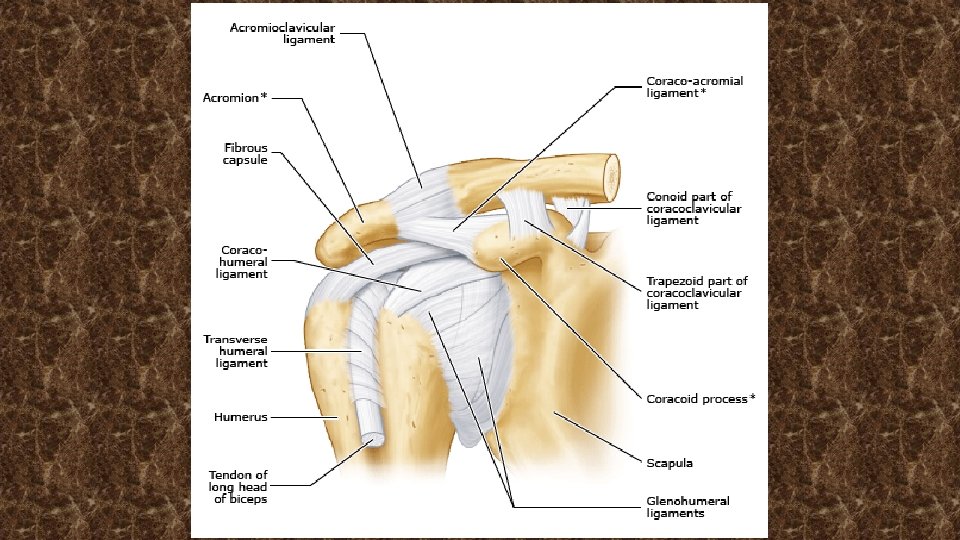
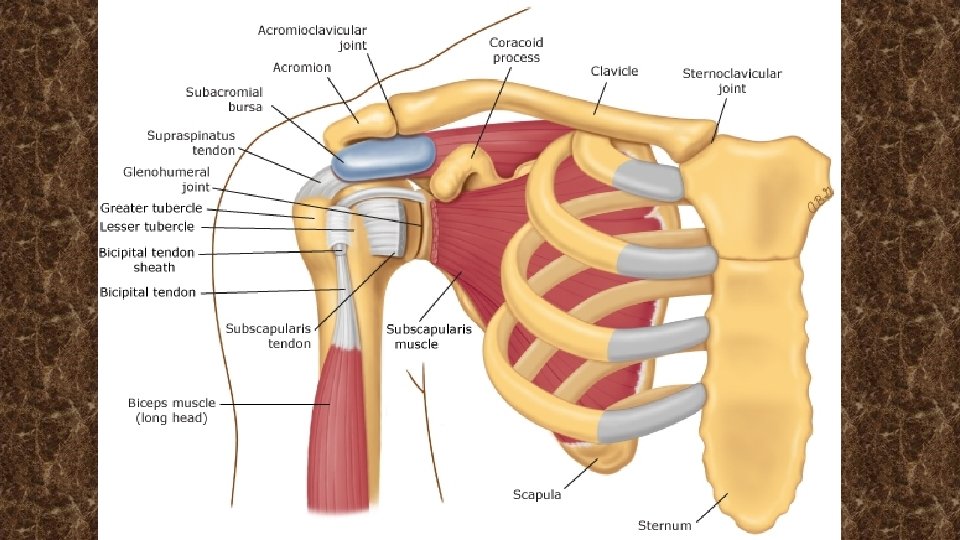

ANATOMY OF THE SHOULDER Rotator Cuff and Muscle Function: Internally Rotate – Subscapularis Externally Rotate – Infraspinatus and Teres Minor Abduction – Supraspinatus and Deltoid The Rotator cuff helps compress the humoral head and stabilize the joint along with the glenohumeral ligament.

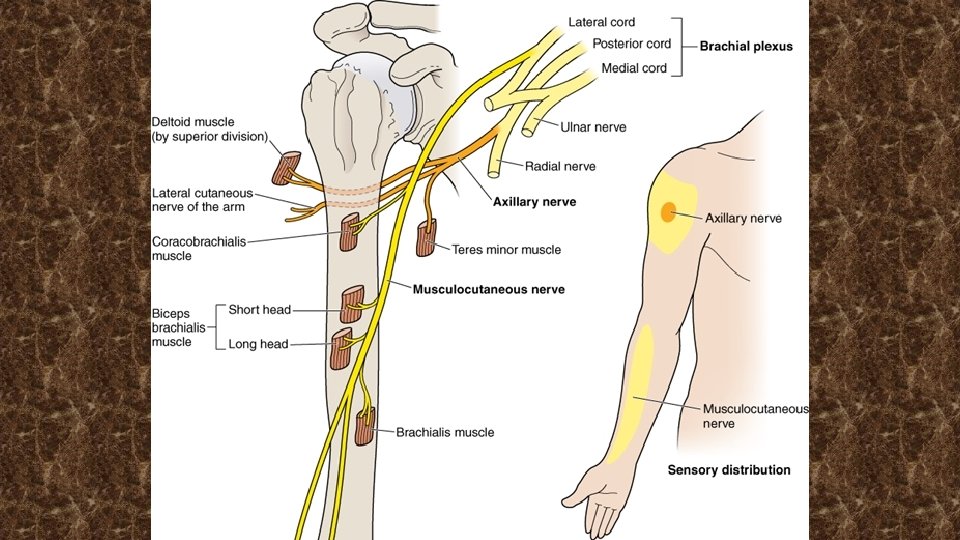
ANATOMY OF THE SHOULDER Axillary Artery and Nerve: - The other structure to be aware of is the axillary artery and the nerve with its branch, the lateral cutaneous nerve of the arm. - Laceration of the artery with reduction of a fracture humerus can be devastating. - The nerve can be injured from humeral head fractures, inferior shoulder dislocations or incorrect use of crutches. - Result is numbness over the upper lateral aspect of the arm.

TYPES OF SHOULDER DISLOCATIONS There are various types of injuries to the shoulder. This presentation will only address dislocations. However a common error is diagnosing an A-C separation as a dislocation.

TYPES OF SHOULDER DISLOCATIONS There are 3 types of dislocation. 1. Anterior 95 - 97% of dislocations 2. Posterior 2 -4% 3. Inferior < 1%

Anterior Dislocation: Arm is abducted and externally rotated. Inferior Dislocation: Arm is above head and unable to adduct. Posterior Dislocation: Arm is adducted and internally rotated. Unable to externally rotate

TYPES OF SHOULDER DISLOCATIONS There are 3 types of dislocation. 1. Anterior 2. Posterior 3. Inferior

IMAGING OF SHOULDER DISLOCATIONS Subsequent slides in this presentation will cover the specific radiological signs of shoulder dislocations. However if you have an ultrasound in your ER department, a quicker and perhaps easier way to distinguish anterior versus posterior dislocation is via ultrasound.

ULTRASOUND FOR SHOULDER DISLOCATIONS - Remember, ultrasound is more sensitive to determining a posterior dislocation than x-ray. - 100% sensitivity, 100% specificity and 98% positive predictive value. - West J Emerg Med. 2017 Aug; 18(5): 937– 942 - Plus is faster, cheaper and no radiation exposure.

ULTRASOUND FOR SHOULDER DISLOCATIONS You can first scan the humeral head (down the anterior aspect of the humerus) looking for a fracture before you even attempt a reduction. Then go to the back and scan under the scapular spine to look at the glenohumeral joint. With anterior dislocations, the humeral head will be distal to the glenoid on the U/S monitor (away from your probe) With posterior dislocations, the humeral head will be proximal to the glenoid.

ULTRASOUND FOR SHOULDER DISLOCATIONS U/S probe

ULTRASOUND FOR SHOULDER DISLOCATIONS

ULTRASOUND FOR SHOULDER DISLOCATIONS

ANTERIOR SHOULDER DISLOCATION

ULTRASOUND OF POSTERIOR DISLOCATION

ANTERIOR SHOULDER DISLOCATION - Usually due to forces to the abducted, externally rotated and extended arm. - May also be caused from a fall on outstretched arm.

ANTERIOR SHOULDER DISLOCATION Clinically: - Clinically arm will be slightly externally rotated and abducted. - The acromion will appear prominent with ‘depression’ over the normal rounded shoulder. - Up to 40% have axillary nerve damage, but most recover.


ANTERIOR SHOULDER DISLOCATION Complications: 1. Fractured humeral head: - occur in ~ 25% of dislocations. - more frequent in age > 40, first time dislocations and traumatic mechanism. - if none of these factors, x-rays may not be indicated. - humeral head fracture is a contraindication for reduction as it can result in avascular necrosis.
")
ANTERIOR SHOULDER DISLOCATION Complications: 2. Axillary Nerve injury. (occur in up to 40% cases) - assess for numbness over upper lateral arm. - usually resolve spontaneously. 3. Brachial plexus, radial nerve damage. - weakness of hand, arm and shoulder. 4. Axillary artery damage. - check for axillary hematoma, reduced radial pulse and/or cool extremity.

ANTERIOR SHOULDER DISLOCATION Imaging: - Depending on location, imaging may or may not be available. - If unavailable, decisions to reduce are based on time line, clinical status and confidence of diagnosis.

ANTERIOR SHOULDER DISLOCATION Imaging: 3 Views: - Anteroposterior - Scapular Y - Axillary

NORMAL SHOULDER X-RAY AP View Scapular Y View Axillary View

ANTERIOR SHOULDER DISLOCATION AP View Scapular Y View Axillary View
 Injuries 1. Hill-Sacks Deformity 2. Bankart Lesion")
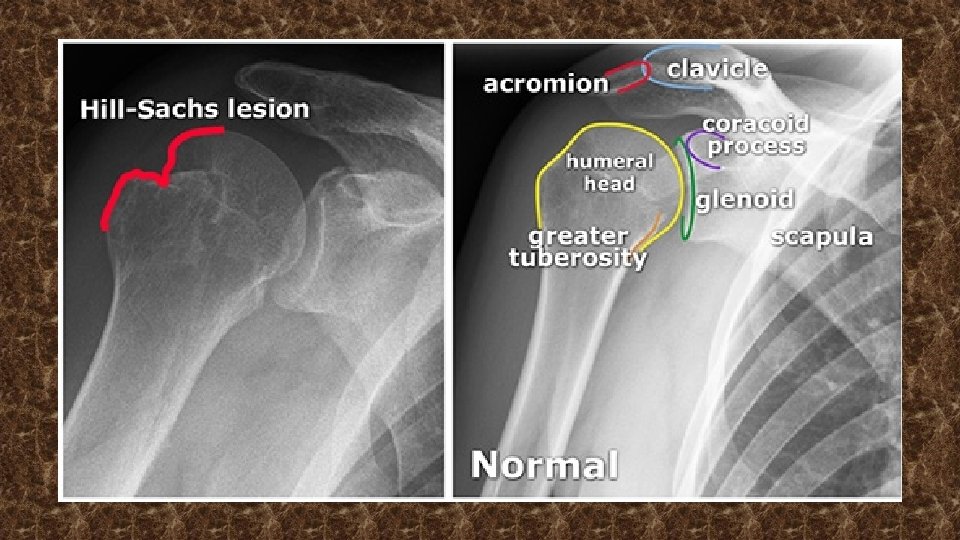
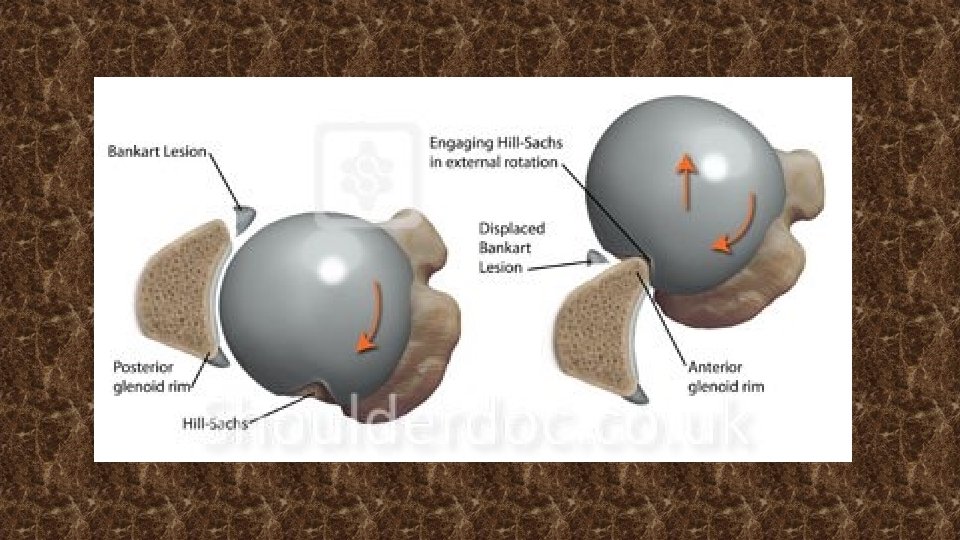
ANTERIOR SHOULDER DISLOCATION Associated (Radiologic) Injuries 1. Hill-Sacks Deformity 2. Bankart Lesion

ANTERIOR SHOULDER DISLOCATION Hill Sacks Deformity - Cortical depression in the humeral head. - Occur in ~ 50% of first time anterior dislocations. - Incidence and size of lesions increases with dislocations. - Treatment can usually be physiotherapy unless recurrent dislocations (ie > 5), then surgical assessment is indicated.

ANTERIOR SHOULDER DISLOCATION Bankart Lesion - Damage to the anterior part of the glenohumeral labrum from repeated anterior shoulder subluxations and/or dislocations. - Clinically characterized by non specific shoulder pain that is worse when the arm is held behind the back. - Can have a sense of weakness and instability. - Diagnosed with MRI. - Treatment is physiotherapy or operative.

REDUCTION ANTERIOR SHOULDER There have been numerous techniques described. They all work, as reduction of this joint is usually not that difficult. The technique should: - Have a high rate of success. - Ideally not require procedural sedation. - Be the most comfortable for the patient. - Be easy to learn and remember. - Low incidence of complications.

REDUCTION ANTERIOR SHOULDER There is not one technique that is particularly preferable over the others, but clinicians should be familiar with a few in case one doesn’t work. The following slide lists some of these, but in no particular order of preference.

REDUCTION ANTERIOR SHOULDER 1. Scapular Manipulation 2. Cunningham Technique 3. External Rotation 4. Prone Technique 5. Fares Technique 6. Modified Milch Technique 7. Kocher 8. Many others: Hippocratic, Eskimo, Chair, Davos. . .

REDUCTION ANTERIOR SHOULDER Up to 90% of anterior reductions do NOT require IV sedation. Some clinicians use intra-articular xylocaine, but even this is often not required.
 Check Axillary Nerve and Radial Pulse Can adduct")
ALGORITHM Anterior Shoulder Dislocation (x-ray confirmed) Check Axillary Nerve and Radial Pulse Can adduct arm? Yes SMT Cunningham Modified Milch No Ext. Rotation Fares SMT Kocher Successful – x-ray confirm, sling Modified Milch Kocher
 - One of the easiest and least traumatic techniques. -")
SCAPULAR MANIPULATION TECHNIQUE (SMT) - One of the easiest and least traumatic techniques. - The patient sits upright and leans the unaffected shoulder against the stretcher. - The physician stands behind the patient and palpates the tip of the scapula with his thumbs and directs a force medially. - The assistant stands in front of the patient and provides gentle downward traction on the humerus. - If only one operator, have patient lie prone on stretcher with arm hanging down, often with 10 lb. weight attached.
")
SCAPULAR MANIPULATION TECHNIQUE (SMT)

CUNNINGHAM TECHNIQUE - Tends to be most successful if patient is able to adduct the arm against the chest. - Try to get the patient to relax as much as possible. - Instruct the patient to pull their shoulder blades together and straighten their back. This maneuver moves the scapula medially and removes the major obstacle preventing reduction of the humeral head

CUNNINGHAM TECHNIQUE - Clinician sits in front of the patient, who assumes a comfortable sitting position. - The patient places the hand on the affected side atop the clinician’s shoulder. The clinician rests one arm gently in the patient’s elbow crease while the other hand gently massages the patient’s biceps, deltoid, and trapezius.

VIDEO ON CUNNINGHAM TECHNIQUE

EXTERNAL ROTATION TECHNIQUE - Requires only one operator and rarely entails procedural sedation. - Patient lies supine with elbow flexed at 90 degrees. - Hold the elbow to ensure adduction. - With the other hand, grasp the patient’s wrist and slowly externally rotate. - Stop and wait if any pain, spasm or resistance is met. - Reduction can be subtle, with no ‘clunk’.

EXTERNAL ROTATION TECHNIQUE

EXTERNAL ROTATION TECHNIQUE

FARES TECHNIQUE - Also known as the ‘Hand Shake’ technique. - Patient lies supine on a stretcher with the affected upper extremity at their side. - The clinician grasps the patient’s wrist, extends the arm straight and gently pulls the arm to provide traction. No counter-traction is used.

FARES TECHNIQUE - The arm is gradually abducted while the clinician continuously moves the arm up and down in an arc of approximately 10 cm. (the ‘hand shake’). - The up and down motion helps relax the shoulder musculature. If the shoulder has not reduced by 90 degrees of abduction, external rotation is added.

MODIFIED MILCH TECHNIQUE - The patient may be supine or prone, with the shoulder close to the edge of the stretcher. - The affected arm is placed in full abduction overhead, or the patient is instructed to raise the arm laterally and behind the head. - The operator may assist abduction gently.

MODIFIED MILCH TECHNIQUE - With the patient’s arm in full abduction, the physician gently applies longitudinal traction and external rotation with one arm (see the video below). - If reduction is not completed, the physician uses the thumb or fingers to push the humeral head up into the glenoid fossa, with gradual adduction of the extended arm still held in traction.

MODIFIED MILCH TECHNIQUE

KOCHER TECHNIQUE - This technique has become less favored over other less potentially painful and safer methods (nerve damage and humeral fractures) - Flex the elbow to a right angle. - Traction in the line of the humerus. - External rotation of the arm: this brings the head of the humerus to face forwards. - The elbow is pulled across the body: this adducts the humerus and disengages the humeral head. - Internal rotation of the arm: this lets the humeral head fall back into the glenoid.

POST REDUCTION TREATMENT - Shoulder should be immobilized in adduction and internal rotation in a sling or collar and cuff. - Referral for orthopedic consultation within a week. - Most common complication is repeat dislocation. - In patients under 30, immobilization is recommended for 3 weeks. - In patients over 30, mobilization can be after one week.

SUMMARY ANTERIOR DISLOCATIONS - Account for 97% +/- shoulder dislocations. - Check for axillary nerve integrity and radial pulse. - 90% of reductions can be without IV analgesia. - Best if you can obtain pre and post reduction x-rays. - There is no one ‘best’ technique. - Be comfortable with a few – SMT, Cunningham, Fares etc.

SUMMARY ANTERIOR DISLOCATIONS

TYPES OF SHOULDER DISLOCATIONS There are 3 types of dislocation. 1. Anterior 2. Posterior 3. Inferior

POSTERIOR DISLOCATIONS - Can occur from a blow to the anterior portion of the shoulder, axial loading of an adducted and internally rotated arm, or violent muscle contractions following a seizure or electrocution. - The posterior shoulder will be prominent with flattening of the anterior shoulder. - The patient will hold the arm in adduction and internal rotation.

POSTERIOR DISLOCATIONS

POSTERIOR DISLOCATIONS - Radiographs can miss up to 50% of posterior dislocations. - The light bulb sign on x-ray is when the humeral head is internally rotated and the tuberosities no longer project laterally. - The result is a circular (‘light bulb’) appearance of the humeral head.

POSTERIOR DISLOCATIONS

POSTERIOR DISLOCATIONS Remember ultrasound for dislocations:

POSTERIOR DISLOCATIONS - Posterior dislocations have higher incidence of surgical neck fractures, reverse Hill-Sachs lesion and damage to the labrum and rotator cuff.

POSTERIOR DISLOCATION REDUCTION - Usually requires procedural sedation. - Use axial traction on the adducted arm, with elbow flexed. - With traction, the arm is internally rotated and adducted. - Pressure on the posterior humeral head may help.

POSTERIOR DISLOCATION REDUCTION

TYPES OF SHOULDER DISLOCATIONS There are 3 types of dislocation. 1. Anterior 2. Posterior 3. Inferior

INFERIOR DISLOCATIONS - Usually occur with the arm fully abducted and axial loading or via forceful hyperabduction of the arm. - Patients will hold the arm above the head and are unable to adduct the arm.

INFERIOR DISLOCATION REDUCTION - Apply traction-countertraction in line with the abducted humerus. - Gentle, gradual adduction of the arm reduces the dislocation. - Closed reduction is successful in most cases, unless a "buttonhole" deformity (humeral head is trapped in a tear of the inferior capsule) exists, in which case open surgical reduction is required.

INFERIOR DISLOCATION REDUCTION

INFERIOR DISLOCATION REDUCTION

THE END
- Slides: 73