Should there be gender differences when treating raised

Should there be gender differences when treating raised blood pressure and cholesterol? Neil R Poulter International Centre for Circulatory Health NHLI, Imperial College London Hong Kong, April 2006

Risk Factors for CHD MODIFIABLE NON-MODIFIABLE High LDL cholesterol Age High blood pressure Sex Smoking Family history Low HDL cholesterol Genetic Lack of exercise Diabetes & glucose intolerance OTHER Left ventricular hypertrophy Birth weight Central obesity Homocysteine Clotting factors Oral contraceptives

Summary report Sex differences in coronary heart disease Why are women so superior? The 1995 Ancel Keys Lecture Elizabeth Barrett-Connor, MD Circulation 1997; 95 -252 -264

Summary • • • Potentially beneficial mechanisms of oestrogen can be shown (+ some harmful) Endogenous oestrogen levels do not predict CHD Lack of oestrogen (menopause) does not ↑ CHD rates Pre-menopausally exogenous oestrogen increases CVD rates Post-menopausally exogenous oestrogen provides no CVD benefit Conclusion: 1 of 8 criteria for assessing a causative link between oestrogen and CVD protection are partially satisfied (laboratory): 7 OF 8 ARE NOT!

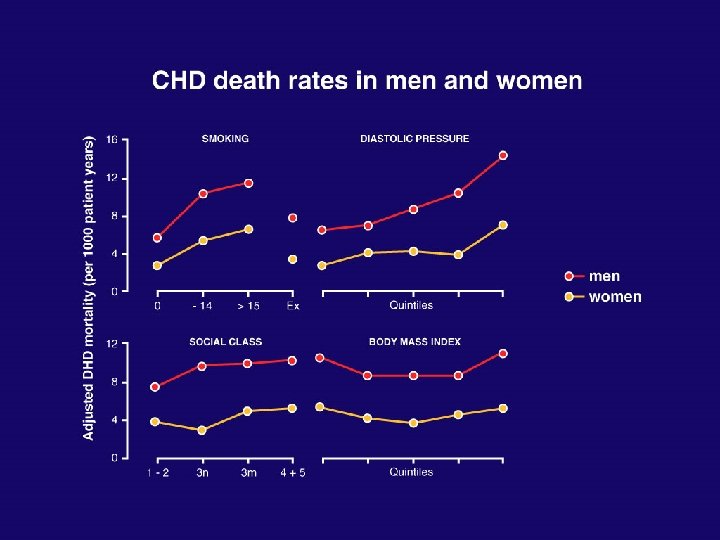
Men are bad! • • • Smoking Diet - fibre - vitamins Lipids (TC: HDL) Blood pressure Blood viscosity Uric acid BUT … - Exercise? - alcohol? - fibrinogen?

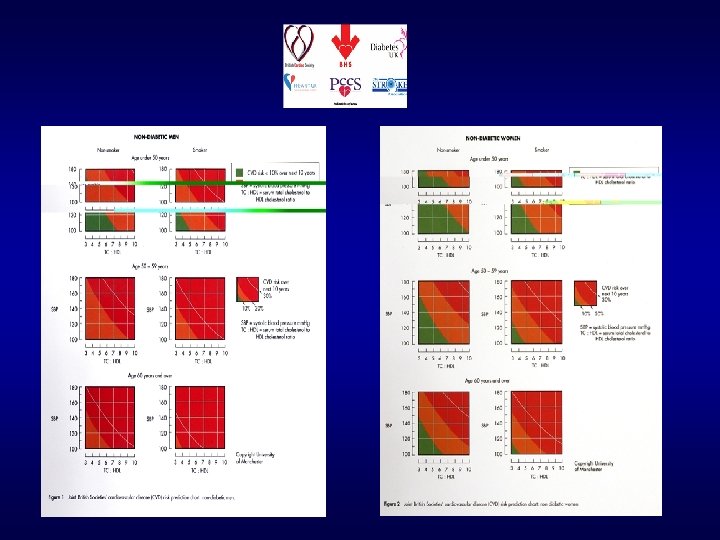
Nondiabetic women Nondiabetic men Diabetic women

Health Survey for England ‘ 98 140/90 mm. Hg 160/95 mm. Hg

Protocol for Prospective Collaborative Overviews of Major Randomised Trials of Blood pressure-lowering Treatments WHO-ISH Blood Pressure Lowering Treatment Trialists’ Collaboration Registry of >30 randomised trials of BP lowering Each trial >1, 000 patient years per limb 1 st analyses (1999) on 64, 000 patients 2 nd analyses (2003) on 195, 000 patients • 8, 000 strokes • 12, 000 CHD events J Hypertens 1998; 16: 127 -137

ACE-I and CCB’S vs DIURETIC/ -BLOCKER

MORE vs LESS BP LOWERING* * HOT: UKPDS: ABCD

“Therefore, achieved blood pressure, not choice of initial therapy, should be the overriding concern of clinicians treating hypertension” Brown, Lancet 2001

Blood Pressure Lowering Treatment Trialists’ Collaboration Second cycle of overview analyses Institute for International Health

Conclusions I · Similar net effects on total cardiovascular events of: · ACE inhibitors · Calcium antagonists · Diuretics/beta-blockers · ARBs also effective in reducing total cardiovascular events

Conclusions III · Size of blood pressure difference between randomised groups closely associated with reduction in risk (except for heart failure) · Size of blood pressure reduction appears to be a more important determinant of outcome than drug choice

Study design 19, 257 hypertensive patients atenolol ± bendroflumethiazide ASCOT-BPLA PROBE design amlodipine ± perindopril 10, 305 patients TC ≤ 6. 5 mmol/L (250 mg/d. L) atorvastatin 10 mg Double-blind ASCOT-LLA placebo Investigator-led, multinational randomised controlled trial
 + fatal CHD Unadjusted")
Summary of all end points Primary Non-fatal MI (incl silent) + fatal CHD Unadjusted Hazard ratio (95% CI) 0. 90 (0. 79 -1. 02) Secondary Non-fatal MI (exc. Silent) +fatal CHD Total coronary end point Total CV event and procedures All-cause mortality Cardiovascular mortality Fatal and non-fatal stroke Fatal and non-fatal heart failure 0. 87 (0. 76 -1. 00) 0. 87 (0. 79 -0. 96) 0. 84 (0. 78 -0. 90) 0. 89 (0. 81 -0. 99) 0. 76 (0. 65 -0. 90) 0. 77 (0. 66 -0. 89) 0. 84 (0. 66 -1. 05) Tertiary Silent MI Unstable angina Chronic stable angina Peripheral arterial disease Life-threatening arrhythmias New-onset diabetes mellitus New-onset renal impairment 1. 27 (0. 80 -2. 00) 0. 68 (0. 51 -0. 92) 0. 98 (0. 81 -1. 19) 0. 65 (0. 52 -0. 81) 1. 07 (0. 62 -1. 85) 0. 70 (0. 63 -. 078) 0. 85 (0. 75 -0. 97) Post hoc Primary end point + coronary revasc procs CV death + MI + stroke 0. 86 (0. 77 -0. 96) 0. 84 (0. 76 -0. 92) 0. 50 0. 70 1. 00 Amlodipine perindopril better 1. 45 2. 00 Atenolol thiazide better The area of the blue square is proportional to the amount of statistical information

Total CV events and procedures among subgroups p value Diabetes No diabetes Heterogeneity p 0. 0283 <0. 0001 0. 5205 0. 0001 0. 0030 0. 1138 Obese Non-obese 0. 0162 <0. 0001 0. 6753 Older (>60 years) Younger (≤ 60 years) <0. 0001 0. 0227 0. 7816 0. 0015 0. 0001 0. 2889 0. 0056 <0. 0001 0. 6364 0. 0019 0. 0001 0. 4863 <0. 0001 0. 0055 0. 7130 0. 0015 0. 0002 0. 9417 Current smoker Non-current smoker Female Male LVH according to ECG or ECHO No LVH according to ECG or ECHO Previous vascular disease No previous vascular disease Renal dysfunction No renal dysfunction With metabolic syndrome Without metabolic syndrome All patients <0. 0001 0. 60 0. 70 0. 80 0. 90 1. 00 1. 50 Amlodipine perindopril better Atenolol thiazide better The area of the blue square is proportional to the amount of statistical information

Landmark statin trials: effect of therapy on clinical events Study Primary Prevention WOSCOPS AFCAPS/Tex. CAPS Baseline LDL* Ending Years of 1° Efficacy LDL* follow-up parameter RR reduction (%) 3. 0 (115) 4. 9 5. 2 MI+CHD death+ unstable angina 31 36 3. 4 (131) 2. 3 (90) 3. 3 MI+CHD death 36 Primary/Secondary Prevention HPS 3. 4 (131) 2. 7 (104) 5. 0 MI+CHD death 24 Secondary Prevention 4 S CARE LIPID 4. 9 (188) 3. 2 (122) 3. 6 (139) 2. 5 (98) 5. 4 Total mortality 30 3. 9 (150) 2. 9 (112) 5. 0 MI+CHD death 24 ASCOT 5. 0 (192) 3. 7 (142) 3. 9 (150) 6. 1 24 *mmol/L (mg/d. L) Shepherd JM. N Engl J Med 1995; 333: 1301– 1307. Downs JR. JAMA 1998; 279: 1615– 1622. Sever. Lancet 2003; 361: 1149 – 1158. HPS Group. Lancet 2002; 360: 7– 22. 4 S Group. Lancet 1994; 344: 1383– 1389. Sacks FM. N Engl J Med 1996; 335: 1001– 1009. LIPID Group. N Engl J Med 1998; 339: 1349– 1357.

Event rates plotted against LDL cholesterol levels during statin therapy in secondary-prevention studies

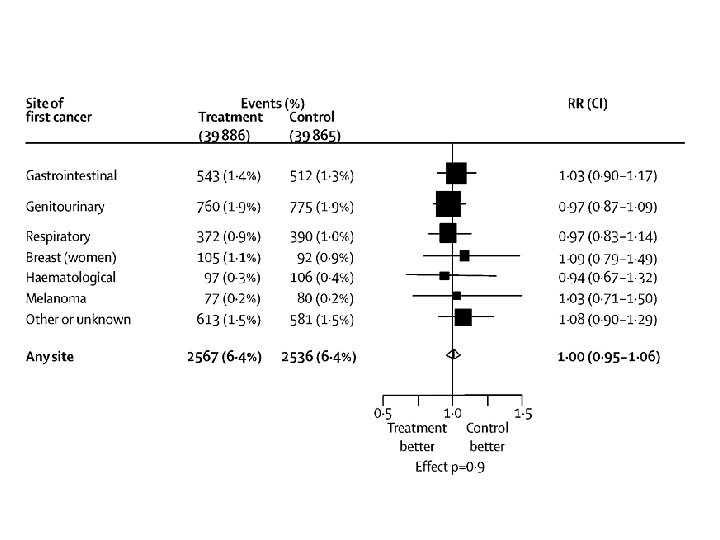
·Efficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from 90 056 participants in 14 randomised trials ·Cholesterol Treatment Trialists’ (CTT) Collaborators ·Lancet 2005; 366: 1267 -1278

Proportional effects on major CV events/ mmol/L of LDL reduction Events Men Women Rx Control HR (95% CI) 5097 1257 6504 1490 0. 78 (0. 75 -0. 81) 0. 83 (0. 76 -0. 91) CTT Collaboration, Lancet 2005

Study design 19, 257 hypertensive patients atenolol ± bendroflumethiazide ASCOT-BPLA PROBE design amlodipine ± perindopril 10, 305 patients TC ≤ 6. 5 mmol/L (250 mg/d. L) atorvastatin 10 mg Double-blind ASCOT-LLA placebo Investigator-led, multinational randomised controlled trial

Primary End Point: Nonfatal MI and Fatal CHD Atorvastatin 10 mg Number of events 100 Placebo Number of events 154 36% reduction HR = 0. 64 (0. 50 -0. 83) p=0. 0005

Prespecified Subgroups: Primary End Point Risk Ratio Diabetes Nondiabetes Current smoker Noncurrent smoker Obese Nonobese LVH No LVH Older (>60 years) Younger (≤ 60 years) Female Male Previous vascular disease No previous vascular disease Renal dysfunction No renal dysfunction With metabolic syndrome Without metabolic syndrome Hazard Ratio 0. 84 (0. 55 -1. 29) 0. 56 (0. 41 -0. 77) 0. 56 (0. 37 -0. 85) 0. 70 (0. 51 -0. 96) 0. 59 (0. 39 -0. 90) 0. 67 (0. 49 -0. 92) 0. 67 (0. 35 -1. 29) 0. 64 (0. 49 -0. 84) 0. 64 (0. 47 -0. 86) 0. 66 (0. 41 -1. 06) 1. 10 (0. 57 -2. 12) 0. 59 (0. 44 -0. 77) 0. 80 (0. 45 -1. 42) 0. 61 (0. 46 -0. 81) 0. 61 (0. 44 -0. 84) 0. 70 (0. 47 -1. 04) 0. 77 (0. 52 -1. 12) 0. 56 (0. 40 -0. 79) All patients 0. 64 (0. 50 -0. 83) Atorvastatin better Placebo better 0. 5 1. 0 1. 5 Area of squares is proportional to the amount of statistical information Sever PS, et al. Lancet. 2003; 361: 1149 -1158.

Subgroups: Total CV Events and Procedures Risk Ratio Diabetes Nondiabetes Current smoker Noncurrent smoker Obese Nonobese LVH No LVH Older (>60 years) Younger (≤ 60 years) Female Male Previous vascular disease No previous vascular disease Renal dysfunction No renal dysfunction With metabolic syndrome Without metabolic syndrome All patients Atorvastatin better Placebo better 0. 5 1. 0 Area of squares is proportional to the amount of statistical information 1. 5

HSE Lipids 2003: Treatment and control in subgroups Treatment * Subgroup Control * ≠ M F CHD or stroke: Hx 71. 1 55. 8 51. 7 28. 8 Hypertension 32. 7 22. 4 22. 9 11. 1 Diabetes 50. 9 50. 0 33. 3 31. 9 * Among those with TC >5 mmol/l or on Rx ≠ <5. 0 mmol/l
 • Current smoker (began 5 years")
Case history • 19 year old woman (JP) • Current smoker (began 5 years ago) Treatment plan (a) Based on short-term absolute risk (b) - NO ACTION (b) Based on long-term intuition - ADVISE

Summary · Clinical guidelines relating to CVD need to incorporate a broad multifactorial approach · Total (‘global’) CV risk assessment will assist decision-making, but the shortcomings of the system used should be appreciated · Intervention based on estimated total CV risk levels remains unvalidated in RCT’s · The majority of CV events can be prevented by optimal treatment of raised BP and lipid levels supported by non-drug interventions.

Should there be gender differences when treating raised blood pressure and cholesterol? 1. If treatment is based on estimated CV risk More man will be treated 2. For the same level of CV risk women benefit as much as men
- Slides: 37