SHOCK HYPOTENSION Medical Department Penang General Hospital Case














- Slides: 15
SHOCK/ HYPOTENSION Medical Department, Penang General Hospital
Case Senario 1: 68 year old lady, known case of diabetes mellitus for 15 years, hypertension, bilateral knees osteoarthritis. On regular medications from Klinik Kesihatan. 1 week history of poor appetite, lethargic, cough. Noted by family to be confused, SOB on the day of admission. BP: 90/50 mm. Hg HR : 120 bpm
What other information from the history do you need? What are the other vital signs that you want to know?
GCS: 11/15 BP: 90/50 mm. Hg PR: 120 bpm, not feeble Temperature: 38 degree celsius RR: 40 breath/ min, Sp. O 2 under room air: 93% Reflomet: 20 mmol/L Clinically pale, dehydrated. Lungs: Lt basal crepitation with occasional rhonchi. CVS: NAD CNS: moving all 4 limbs (unable to follow command) PA: mild tenderness at epigastric region, otherwise soft. BS normal.
Why is her GCS low? Why is she tachycardic but with a pulse which is not feeble? Why is she tachypnoeic? What do the lung findings suggest? Why does she have a tender epigastrium?
What is the cause of her shock? What tests can you do to help with your diagnosis?
How would you resuscitate her?
Case Senario 2 24 year old Vietnamese lady, factory worker, came to A+E with 2 days history of abdominal pain, worsening in nature. Language barrier, minimal history.
On examination: ◦ ◦ ◦ In pain, restless, obey command, moving all 4 limbs. Pale, no jaundice, dry BP: 90/60 mm. Hg PR: 123 bpm (feeble) Sp. O 2: 100% room air RR: 36 breath/min Afebrile ◦ CVS, lungs: NAD ◦ PA: guarded, tender. No hepatosplenomegaly. Bowel sounds present and normal.
What is the diagnosis? Why is her pulse feeble? Why is she dry? How would you manage her?
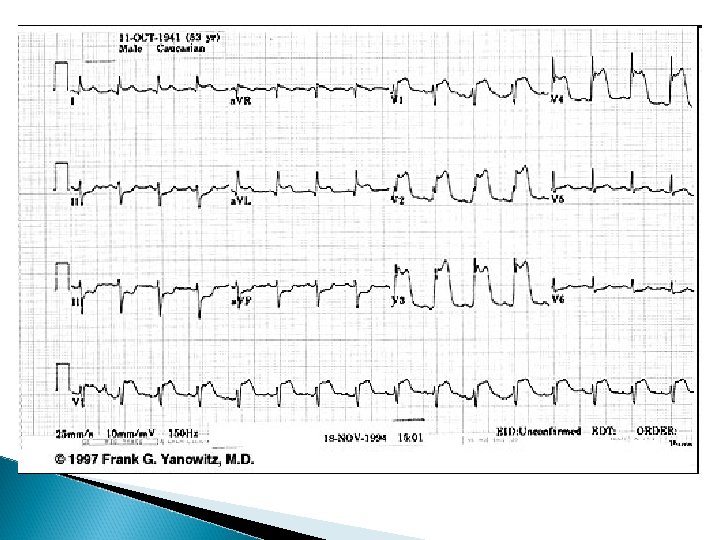
Senario 3: 55 year old gentleman, a case of diabetes mellitus, hypertension, dyslipidemia, on treatment. Under OPD follow up. C/O: ◦ Sudden left sided chest pain since morning, associated with SOB, vomiting, profuse sweating. On examination: ◦ Conscious, alert, in pain ◦ BP: 90/60 bpm, PR: 110 bpm (regular, poor volume), afebrile, Sp. O 2: 96% under room air, RR: 28 breaths/ min
Hydration: fair CVS: S 1 S 2 ESM mitral area Lungs: clear, air entry equal PA: soft, non tender, BS present Diagnosis? Explain the murmur? What is the one investigation to order immediately?
What is the diagnosis? How would you manage him?
So how do you classify shock? How do you tell them apart?