SHINING A LIGHT ON BLACKOUTS A COLLABORATIVE APPROACH

SHINING A LIGHT ON BLACKOUTS – A COLLABORATIVE APPROACH South Tees Blackout Team

James Cook University Hospital South Tees NHS Foundation Trust
/Blackout Team • • 5 Consultant Cardiologists 1 Consultant Neurophysiologist 6")
Cardiac Rhythm Management (CRM)/Blackout Team • • 5 Consultant Cardiologists 1 Consultant Neurophysiologist 6 CRM Specialist nurses 1 Epilepsy Nurse Consultant 1 CRM Nurse Consultant 8 Cardiac Physiologists (7 wte) 2 Health Care Assistants 3 Administrative Assistants Specialist nurses – At least masters level/non medical prescribers, clinical skills, arrhythmia/syncope module, competency based in house training

Falls Drop attacks Epilepsy Catoplexy Cardiac Syncope Epilepsy Psychogenic Syncope Reflex Syncope Metabolic disorders Intoxication

Key Drivers • NICE TLOC Guidelines • European Society of Cardiology Guidelines for the Management of Syncope • NSF Chapter 8 Arrhythmias and Sudden Cardiac Death • No dedicated pathway for patients experiencing blackout • Local audit showed delayed patient pathway and over use of diagnostic testing

The Beginning………. . • Identify a coordinator • Audit to examine existing pathways/process map • Look at other established services • Develop business case • Liaise with key stakeholders/steering group

South Tees Blackout Team Consultant Cardiologist CRM Specialist Nurses/Nurse Consultant Cardiac Physiologists Epilepsy Specialist Nurse Consultant Neurophysiologist Health Care Assistants Secretaries

South Tees Blackout Service • Commenced in December 2010 • 1 year pilot funded by Middlesbrough, Redcar & Cleveland primary care trust • Evaluation concluded that the model was efficient and cost effective • Tariff agreed

Initial Results • Comparison of admission rates for patients presenting with non complicated syncope May 2010 – November 2011 and December 2010 – June 2011 - Average reduction of 19. 5 admissions per month - Approximate saving of £ 140, 000 per annum - Reduction of 409 bed days over 31 week period - Approximate saving of £ 74, 000 per annum • Reduced waiting times - Cardiology 8. 3 weeks to 5. 9 weeks - Epilepsy 5 weeks to 4 weeks - First fit 4 weeks to 2. 8 weeks

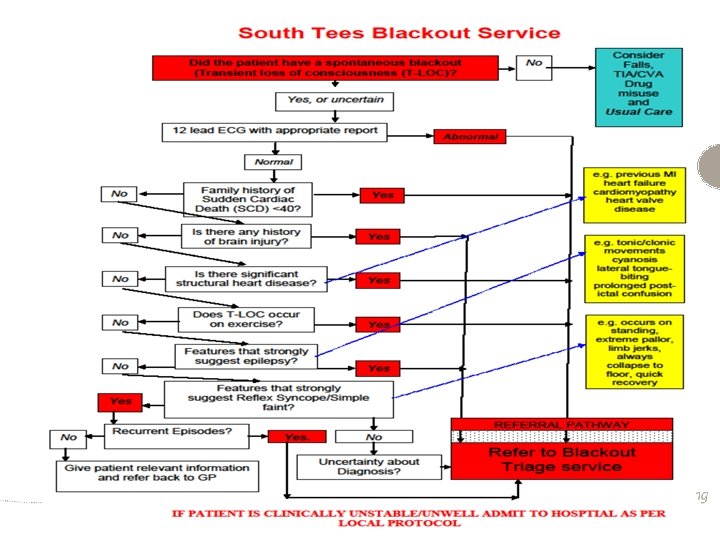
Effective referral pathway • Easier access to specialist review • Eliminates clinical uncertainty, misdiagnosis and inappropriate treatment and unnecessary financial cost • The South Tees blackout clinic has a clear referral pathway used by A&E / AAU / GP practices Ali et al (2009); NICE (2010)

Referrals • • • Accident and Emergency 52% Primary Care 39% Other 9%

South Tees Blackout Service • Nurse triage of all referrals/Nurse led Clinics • Same day access to Consultants • 3 new clinic per week – 18 slots, 1 review clinic per week – 12 slots • One stop shop offering: -History taking/Witness Accounts -Clinical examination -ECG -Echocardiogram -Holter monitoring -EEG/MRI/CT (not same day)

How do we achieve the right diagnosis? • • • Effective triage Structured history taking – medical model Systematic approach – blackout service database Witness accounts Investigations - ECG, ECHO, Holter monitoring, EEG, CT / MRI Exclusion of red flags

‘Red flags’—indicators of high risk of a serious adverse event, needing specialist assessment • Cardiac red flags • Neurological red flags • Abnormal 12 -lead ECG • History of brain injury • Presence of structural heart disease • Features which strongly suggest epilepsy • Family history of sudden cardiac death (SCD) aged <40 years • New neurological deficit • Blackout occurring during exercise • NB No red flags = patient at low risk of a serious adverse event (NICE, 2010)

Is the South Tees model effective?

Comparison of waiting times • The median waiting times for the blackout clinic was 25. 5 days, the first fit clinic 48. 5 days and the general neurology clinic 91. 5 days.

Comparisons • • Investigations 100% of patients seen via the blackout clinic model had ECG performed compared to 35. 7% attending the first fit clinic and 16. 7% attending general neurology. • • Hospital admissions In areas without access to a blackout service admissions were 100% & 54. 5% compared to 17. 6% in the South Tees area.

Diagnosis at first appointment • At the first appointment in the blackout and first fit clinics 91. 8% and 88. 1% respectively received a diagnosis compared to 69. 4% in the general neurology clinic.

Pre blackout service – 46 year old gentleman presents to A&E with blackout • 2001 – A&E (ECG, NAD – discharged, with no further follow up) • 2005 – Re presents to GP with further episodes of blackout • 2005 – GP refers to Consultant Physician (CT head and chest, ECG, • • bloods, CXR – NAD) advises GP to refer to Neurologist 2005 – GP refers to Neurology 2005 – Consultant Neurologist (EEG, ECG, Bloods, Tilt test) Cardiac cause suspected and referral advised. No evidence of this happening in notes. 2009 – Re presents to A&E following RTA after having blackout - Re referred to Neurology 2009 – Neurologist again advises referral to cardiology 2010 – GP refers to cardiology 2010/2011 – Seen by cardiologist who suspects cardiac cause. ECG, 7 day ambulatory ECG NAD. Implantable loop recorder (ILR) implanted 2011 – Ventricular pauses evident on interrogation of ILR 2011 - Permanent pacemaker implanted

Post blackout service – 66 year old gentleman presents to A&E with a blackout (2 episodes) • February 2011 – A&E (ECG NAD) refer to blackout service • February 2011 – Blackout clinic (triage, history taking, cardiac cause suspected - ECG, 72 hr ambulatory ECG NAD). Discussed with cardiologist and listed for ILR • April 2011 – ILR implanted. Ventricular pauses evident on analysis • June 2011 – Permanent pacemaker implanted

Pre blackout service - 26 year old female presents to GP after 2 episodes of blackout • July 2008 – GP refers to Cardiology. (ECG, Tilt test, 72 hour ambulatory ECG, NAD). Cardiologist suggests referral to Neurology • Nov 2008 – GP refers to Neurology • Jan 2009 – Neurology – (EEG, CT scan, history taking, witness account). Epilepsy diagnosed. Medication commenced

Post blackout service – 47 year old gentleman presents to A&E with blackout • March 2012 - A&E. Patient self discharges • Feb 2013 – A&E. Further episode of blackout. (ECG, NAD). Referred to blackout service • March 2013 – Blackout clinic (Triage, history taking, first hand witness account obtained. Epilepsy suspected). Liaise with Consultant Neurophysiologist for same day assessment • Consultant Neurophysiologist – Epilepsy confirmed, antiepileptic drugs commenced. Lifestyle advice given

Benefits of a collaborative approach • • • Clear referral pathway Less need for hospital admission Reduced waiting times Appropriate & focused investigations High rate of diagnosis at first appointment

Benefits of a collaborative approach • • • One point of access to multispecialty and multidisciplinary diagnostic and treatment service including neuropyschology Change in culture within Neurology / Cardiology in terms of the management of blackouts High levels of patient satisfaction Strong links with A&E / MAU Closer liaison with elderly care / falls service

Development and Future Plans …. • Service expansion to cover North Yorkshire/North Tees. June 2018 • Nurse led ILR implant and follow up has already commenced further streamlining the service
![Specialist Nurse-led Implantable Loop Recorder [ILR] Service](http://slidetodoc.com/presentation_image_h2/d28bf054eea6a191a51b5a51465fc2d8/image-27.jpg "Specialist Nurse-led Implantable Loop Recorder [ILR] Service")
Specialist Nurse-led Implantable Loop Recorder [ILR] Service

Background • ILRs have increasingly been used for the clinical evaluation of unexplained syncope in the last decade. • ILRs are used for long-term heart rhythm monitoring to diagnose unexplained syncope or for detection of suspected atrial and ventricular arrhythmias. • Detection of arrhythmias, the most common cardiac causes of syncope, is important, because of the associated mortality risk. • ILRs have been shown to have a high diagnostic yield and shortened the time to diagnosis [43 and 52% with ILR while conventional tests have a diagnostic yield of 6– 20%] [Krahn et al 2001 & Farwell et al 2004].

Cost comparison of two implantable cardiac monitors in two different settings: Reveal XT in a cath lab vs. Reveal LINQ in a procedure room [Kanters et al 2015] • This study documents that miniaturization of technology saves hospital resources. • The insertion of a miniaturized cardiac monitor [ILR] is simpler and faster than the implantation of the previous version. • Owing to the miniaturized size and specifically designed insertion kit, the procedure no longer needs to take place in a cath lab, but can be performed in a less resource intensive setting – procedure ‘clean’ room. • The procedural efficiencies and change in implant location could lead to cost savings although variable in different centres.

Cost comparison of two implantable cardiac monitors in two different settings: Reveal XT in a cath lab vs. Reveal LINQ in a procedure room [Kanters et al 2015] • Labour costs were lower for Reveal LINQ, owing to shorter preparation, procedure time, and reduced recovery time. In addition, physicians could be substituted by less-qualified, and hence, less costly personnel. • Depreciation costs for instruments and equipment were considerably lower for a procedure room as well as overhead costs. • Excluding hospital admission costs there was an estimated 384 euro saving per patient

Pathway Comparison Traditional Pathway Nurse Led Pathway Referrals from Blackout clinic / neuro / cardiologist clinics to waiting list Implant date - admitted to CDU – usually only ILR that day and admitted at 8 am [procedure start time 9 am] Implant date - admitted to CDU at a specified time [staggered throughout day] First case before other device implants Designated ILR list [4 -6 pts – AM / all day twice a month] Cath lab implant / procedure – fully staffed [45 mins] Procedure room implant by x 2 specialist nurses only [30 mins max] Brief explanation given re: monitor [i. e. activator] in cath lab by physiologist [no family/carer involvement] Full explanation of the care-link system including test transmission [full family/carer involvement] Recovery in CDU [60 -120 mins], discharge, LOS 3 -4 hours Recovery in CDU [30 mins i/c carelink], discharge, LOS 1 -1. 5 hours FU [ all face to face] planned - 5/52 then 6/12 intervals FU [telephone but with flexibility of face to face yearly visits] – 3/12 then 6/12 intervals – daily remote monitoring FU No remote monitoring – no early detection of automated events. Significant automated events undiagnosed until planned FU Daily care-link transmissions reviewed by specialist nurse team – prompt evaluation of both automated and pt. activated events
![Quality Assurance [QA] Audit 2016 • Evaluation of new process/way of working • 12](http://slidetodoc.com/presentation_image_h2/d28bf054eea6a191a51b5a51465fc2d8/image-32.jpg "Quality Assurance [QA] Audit 2016 • Evaluation of new process/way of working • 12")
Quality Assurance [QA] Audit 2016 • Evaluation of new process/way of working • 12 months of data – 125 patients • Comparison of old ILR process vs new nurse-led ILR service – – – No. of devices Referral reason/source Referral to implant date Implant date to diagnosis Diagnosis to device implant time Diagnostic outcomes • • • Endpoint of cardiology diagnosis i. e. PPM / ICD Old ILRs no. of automated events vs pt. activated events] Infection rates • Evaluation of the remote monitoring software used to gain diagnosis • Non formal feedback from patients/carers

Pathway Comparison Over 12 months Traditional Pathway Nurse Led Pathway Average - 70 years Average - 64 years No. of devices implanted - 68 No. of devices implanted - 103 [45% increase] Scheduling of Procedure First case before other device implants Scheduling of Procedure Designated ILR list [4 -6 pts – AM / all day twice a month] Referral sources – Nurse-led RAAC 10% – Nurse-led blackout clinic 16. 6% – Neurology 13. 3% – Cardiology clinics 52. 9% – Medics 6. 6% Referral sources – Nurse-led RAAC 5. 8% – Nurse-led blackout clinic 44. 6% – Neurology 6. 7% – Cardiology clinics 42. 7% – Medics 0% Referral to implant date – 49 days Referral to implant date – 35 days Implant to diagnosis time [SND / AVB] – 270 days Implant to diagnosis time [SND / AVB] – 56 days Diagnosis to upgraded device – 31 days Diagnosis to upgraded device - 22 days Diagnosis • 70% SND • 23. 3% AVB • 6. 6% VT Diagnosis • 45. 5% SND • 54. 5% AVB • 1 pt SVT – RFA • 4 pts new AF requiring OAC Complications - 1 explant [opening of wound] Complications - None

Positive benefits of new nurse-led service • Pro-active vs reactive • Carelink software allows for prompt evaluation of symptom correlation / review of automated events • Immediate action regarding significant automated events • Specialist nurse knowledge enhances process • Expedited diagnostic / treatment plan • Listing for appropriate device • Weekly ILR list • Whole process much swifter than old ILR service

Positive benefits of new nurse-led service Nurse – led ILR Implant time saved by taking procedure out of the cath lab: ILR [old] – 45 mins [45 x 103/60=] 77 hrs Equating to: • PPM – 90 mins = 51. 5 cases • ICD – 90 mins = 51. 5 • CRT – 180 mins = 25. 75 • EPS – 90 mins = 51. 5 • AF cryo ablation – 150 mins = 30. 9 • AF RFA – 240 mins = 19. 3

Summary • The wireless data transmission capability of the Reveal LINQ could lead to savings in staff time when patients are monitored remotely • Less need for face to face appointments • Quicker diagnostic times • Increased flexibility and therefore access to this service • Provision of a more cost effective service • Non-medical personnel performing ILR implants enables focus on more complex procedures • Provision of a specialist service in ILR monitoring provides continuity of care

Other aspects of service/Future plans • • • Implant of ILRs for urgent cases [inpatients before discharge] has commenced Nurses now explanting devices Formal patient questionnaire / feedback. Audit in progress Development of the service to sister hospital. Begins this month Training of further staff to implant devices – Sp. N to assist with programming ILR for detection of AF in cryptogenic strokes

Blacked out? Come to James Cook! We know what we’re doing!!
- Slides: 38