Shared Practice Mark Haslam Cheltenham General Hospital Cheltenham























- Slides: 26
Shared Practice Mark Haslam Cheltenham General Hospital
Cheltenham
3 Cases over 24 hrs…
1. • 57 year old, collapsed at home • Admitted AE 1430 hrs • GCS 4 (E 1 M 2 V 1) • Sedated, intubated & ventilated • Transfer to CT
CT
• Large intracerebral haematoma in the region of right temporal lobe with extension of the acute bleed into the ventricles and subarachnoid spaces around the right cerebral hemisphere. • Localised mass effect with shift of the midline structures to the left. • There is transtentorial herniation with obliteration of the temporal horn of the right ventricle, as well as descent of the cerebral tonsil into the foramen magnum in keeping with markedly raised intracranial pressure.
Entry in AE notes • “Reg NS says not for transfer. Surgery of no benefit. For transfer ITU for ventilation. Possible organ donation” • “Might benefit from mannitol”
Family discussion in ICU • Described as un-survivable injury • Daughter indicated that her mother wanted to be a donor. • Family allowed time to travel to Cheltenham • Standard critical care
The next day. . • Organ donation referral made • Sedation stopped – GCS 3 – extubated to air at 2300 hrs • Retrieval team stood down
• 0500 – localised • 1800 – obeyed commands – E 1 – M 6 – V 2 • Re referred to Neurosurgeons • Intubated, CT & CT angiogram, transferred…
2. • • • 73 yr old male Admitted AE 2200 hrs Collapse GCS 3 at presentation Sedated, intubated and ventilated CT • Subarachnoid haemorrhage • Referred neurosurgeons – described as unsurvivable injury
• Transferred to critical care – Allow family discussion – Explore organ donation • Sedation hold – Reached for ETT • Transferred to neurosurgical centre
3 • 50 yr old woman • Presents to AE with collapse following sudden onset headache • GCS 4 • Ventilated for CT • Subarachnoid haemorrhage • Referred to neurosurgeons – Declined but suggest giving hypertonic saline…
• Re referred 2 hours later and transferred….
• 3 patients: – All refused initially by neurosurgical team – Two managed as un-survivable – All three eventually taken for active treatment and survived.
Problems. .
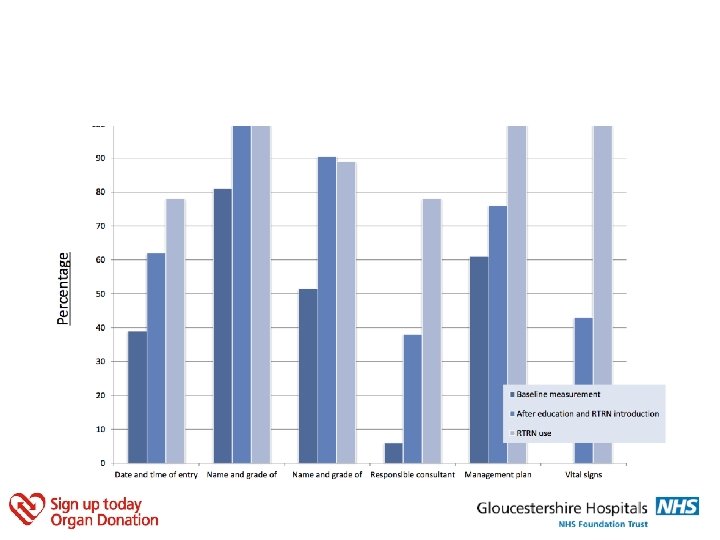
Standard • • • Date and Time of entry Name and Grade of doctor making referral Name and Grade of doctor consulted Consultant responsible Management plan documented clearly Vital signs of patient
Baseline • Retrospective audit • 3 month period – Head-injury – Skull fracture – Subarachnoid haemorrhage • 69 patients, 33 discussed with neurosurgery
Baseline results • • • Date and Time of entry Name/Grade of doctor making referral Name and Grade of doctor consulted Consultant responsible Management plan documented clearly Vital signs of patient 39% 81% 51% 6% 61% 0%
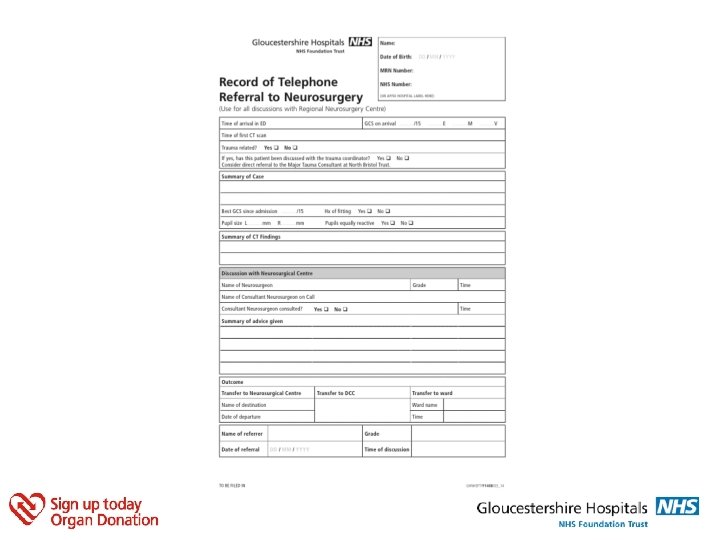
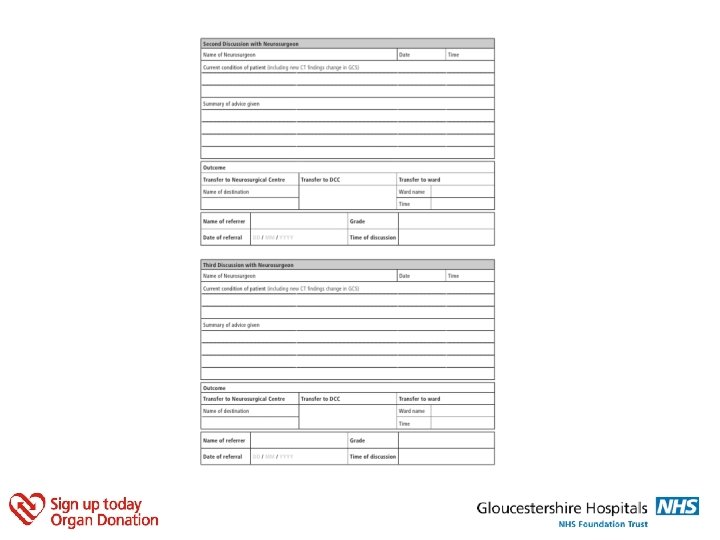
The form…
Strategy • Initial audit presented in ED • Case studies included in presentations • The 'Record of Telephone Referral to Neurosurgery' was introduced to the ED department. • After two weeks, feedback was collected. Following feedback, the location of the RTRN form was publicised more widely. • Re-audit then took place over another 3 month period
Future. .