SEXUALLY TRASMISSIBLE INFECTION Dr Esraa ALMaini Objective Different

SEXUALLY TRASMISSIBLE INFECTION Dr. Esraa AL-Maini Objective: Different types of infection transmitted sexual intercourse Mode of transmission clinical features treatment
 STIs are infections that are transmitted primarily through")
Once known as Venereal Diseases (VD) STIs are infections that are transmitted primarily through sexual contact with an infected person. STIs are very common. An estimated 15 -16 million new cases occur each year in the U. S. alone. 1 in 4 adolescents will get an STI

Clinical Prevention Guidance The prevention and control of STDs are based on the following five major strategies (5): 1 -accurate risk assessment and education and counseling of persons at risk on ways to avoid STDs through changes in sexual behaviors and use of recommended prevention services; 2 -pre-exposure vaccination of persons at risk for vaccinepreventable STDs; 3 -identification of asymptomatically infected persons and persons with symptoms associated with STDs; 4 -effective diagnosis, treatment, counseling, and follow up of infected persons and 5 -evaluation, treatment, and counseling of sex partners of persons who are infected with an STD.

in order to assess the patient it is necessary to find out the : following n n n n When sexual intercourse last took place Whether this was oral, vaginal What contraception was used? When the women last had a different sexual partner A travel history and knowledge about the origin of partner might indicate risk of tropical infection. Information about previous pregnancies and menstruation Enquire about I. V drug use in the patient and her partners Mix infection possible so full screen should be performed

Partners Need to Be Treated All partners should be examined and · treated

n n To break the chain of infection and prevent re infection, it is essential to avoids to intercourse until she is that her partners has been screen and received appropriate treatment Follow up evaluation and test of cure

STI Pathogens Bacteria ·Chlamydia ·Gonorrhea ·Bacterial Vaginosis* ·Syphilis *Not classified as an STI Virus Parasite ·Herpes · ·Hepatitis · B ·Genital Warts (HPV) ·HIV/AIDS · Pubic Lice Scabies Trichomoniasis

Every Pregnant women Needs Screening Dr. T. V. Rao MD 8

Recommended Screening Tests A serologic test for syphilis should be performed for all pregnant women at the first prenatal visit. Women who are at high risk for syphilis or live in areas of high syphilis morbidity should be screened again early in the third trimester (28 weeks) and at delivery. Any woman who delivers a stillborn infant should be tested for syphilis. All pregnant women should be routinely tested for hepatitis B surface antigen (HBs. Ag) at the first prenatal visit even if they have been previously vaccinated or tested

. All pregnant women aged <25 years and older women at increased risk for infection be routinely screened for Chlamydia trachomatis and N. gonorrhoeae at the first prenatal visit. also should be retested during the third trimester to prevent maternal postnatal complications and chlamydial infection in the neonate. Pregnant women found to have chlamydial infection should have a test of cure to document chlamydial eradication (preferably by nucleic acid amplification testing [NAAT]) 3– 4 weeks after treatment and then retested within 3 months

All pregnant women should be tested for HIV infection during the first prenatal visit. A second test during the third trimester, preferably at <36 weeks' gestation, should be considered for all pregnant women and is recommended for those known to be at high risk for acquiring HIV, importance of retesting during each pregnancy. Women with no prenatal care should be tested for HIV at the time of delivery

Areas of Infection

CHLAMYDIA TRACHOMATIS It is commonest bacterial STD, obligate intracellular bacteria that grows in vitro only in tissue culture infect columnar epithelium of endocervix urethra endometrium fallopain tubes and rectum. This organism can persist for long periods in an asymptomatic carrier state. There s no vaccine available and even though chlamydia antibodies are produced, they do not protect against reinfection.

. Annual screening of all sexually active women aged <25 years is recommended, as is screening of older women at increased risk for infection (e. g. , those who have a new sex partner, more than one sex partner, a sex partner with concurrent partners, or a sex partner who has a sexually transmitted infection

Screening and opportunistic testing: 1 Partner of the patient diagnosed or suspected with infection 2 History of Chlamydia in the last year 3 Patient attending GUM clinics 4 Patients with two or more partners with in 12 monthes 5 Women undergoing termination of pregnancy 6 History of other sexually transmitted infection and HIV n n

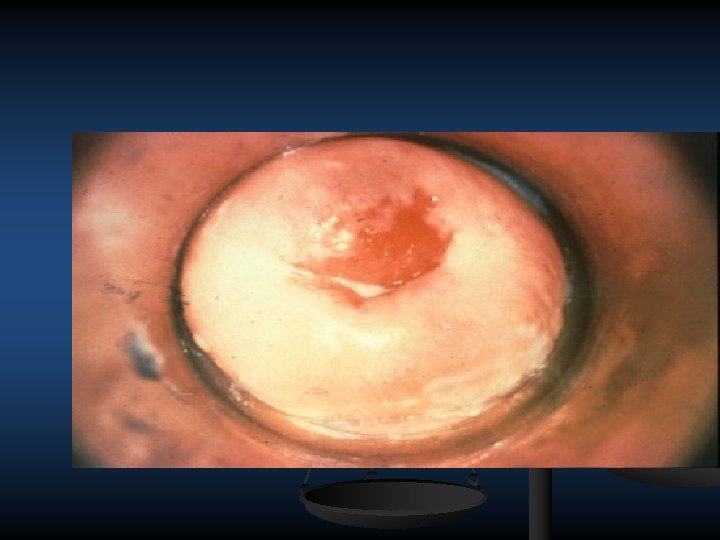
Clinical features: 1 Asymptomatic in 50% of male 2 Or can cause non gonococcal urethritis in male In female 1 Asymptomatic 80%in female 2 Vaginal discharge and lower abdominal pain 3 Postcoital bleeding 4 Intermenstrual bleeding 5 Mucopurulent cervical discharge with contact bleeding 6 Dysuria with urethral discharge

Drips Laboratory Tests for Chlamydia Tissue culture has been the standard Tissue culture expensive not routinely recommended Sensitivity ranges from 60% to 90% Non amplified tests Enzyme Immunoassay (EIA), e. g. Chlamydiazyme ELISA limited sensitivity samples are collected from the endocervix sensitivity and specificity of 85% and 97% respectively useful for high volume screening false positives Nucleic Acid Hybridization (NA Probe), e. g. Gen Probe Pace 2 sensitivities ranging from 75% to 100%; specificities greater than 95% detects chlamydial ribosomal RNA able to detect gonorrhea and chlamydia from one swab need for large amounts of sample DNA 17

Laboratory Tests DNA amplification assays NAATs that are FDA cleared for use with vaginal swab specimens can be collected by a provider or self collected in a clinical setting. 90% sensitive should used replace the old ELIZA polymerase chain reaction (PCR) ligase chain reaction (LCR) first void urine vaginal swab NAATs are not FDA cleared for use with rectal or or opharyngeal swab specimens. 18
 DFA on cx smear, rectal conjunctiva swabs MD Source:")
Chlamydia Direct Fluorescent Antibody (DFA) DFA on cx smear, rectal conjunctiva swabs MD Source: Centers for Disease Control and Dr. T. V. Rao Prevention 19

Chlamydia Symptoms in Women Mucopurulent Cervicitis

Antibiotic treatment Azithromycin 1 g orally in a single dose Doxycycline 100 mg orally twice a day for 7 days Alternative Regimens Erythromycin base 500 mg orally four times a day for Erythromycin ethylsuccinate 800 mg orally four times a day for 7 days Levofloxacin 500 mg orally once daily for 7 days Ofloxacin 300 mg orally twice a day for 7 days

Although the clinical significance of oropharyngeal C. trachomatis infection is unclear and routine oropharyngeal screening for CT is not recommended, available evidence suggests oropharyngeal C. trachomatis can be sexually transmitted to genital sites. therefore, detection of C. trachomatis from an oropharyngeal specimen should be treated with azithromycin or doxycycline.

1. To minimize disease transmission to sex partners, persons treated for chlamydia should be instructed to abstain from sexual intercourse for 7 days after single dose therapy or until completion of a 7 day regimen and resolution of symptoms if present. 2 To minimize risk for reinfection, patients also should be instructed to abstain from sexual intercourse until all of their sex partners are treated. 3 Persons who receive a diagnosis of chlamydia should be tested for HIV, GC, and syphilis. p

4 Test of cure to detect therapeutic failure (i. e. , repeat testing 3– 4 weeks after completing therapy) is not advised unless therapeutic adherence is in question, symptoms persist, or reinfection is suspected IF CHANGE OF PARTNER RESTARTING BETWEEN 3 TO 12 MONTHS IS RECOMMENDED

In pregnancy: PTL Chorioamnionitis Post partum endometritis Neonatal conjunctivitis and pneumnia

GONORRHOEA It is the 2 nd most common bacterial STI Chronic a symptomatic infection is common. It infect columnar epithelium No vaccine No immunity, even antibodies present

Clinical features: 1 Most of infected female are asymptomatic 2 Increase vaginal discharge with lower abdominal pain 3 dysuria with urethral discharge 4 proctitis with rectal bleeding discharge and pain 5 Endometritis 6 Mucopurluent urethral discharge 7 pelvic tenderness with cervical exittion In male more than 70% have symptoms sever urethritis, green urethral discharge, also cause exudative tonsillitis, conjunctivitis, proctitis in female and homosexual male
 on gram stained")
DX 1 Demonstrating typical gram –ve intracellular diplococcic (columnar cubical epith) on gram stained smear of end cervical and rectal pharynx swabs if symptomatic infection

Gonorrhea Gram Stain Dr. T. V. Rao MD Source: Cincinnati STD/HIV Prevention Training Center 30

Culture required co 2 7%, blood agar antibiotic to inhibit growth of other bacteria(Thayer. Martin or Transgrow media culture) 2 -Nnuclic acid amplification test(NAATs) 3 -Nuclic acid hybridization tests 4 -Serological test not useful

Treatment: 1 Screen both partners and refer them to genitourinary medicine clinic 2 Counselled regarding the long term implications of infection leading to chronic pelvic pain and tubal infection and subfertilty 1 Azithromycin 1 g single dose 2 Amoxycillin 1 g +probencid 2 g single dose 3 ciprofloxacin 500 mg single dose 4 single dose cefixime 400 mg Sex partner should screened fully Treat other associated infection Abstinence during treatment at least 7 days ,

in pregnancy it is safe to use Amoxycillin cefixime. n Swabs repeated if; n 1 If there is any doubt of compliance , n 2 if symptoms persistent n 3 suspecions of resistance n Swab should be repeated within week following treatment to check for complete cure n

COMPLECATIONS OF CHLAMYDIA AND GC 1 -Fitz –hugh –curytis syndromeintra abd spread of GC can cause per appendicitis, per hepatitis patient presented with right hypochondria pain tenderness, pyrexia. Examination: usually sign of salpingitis, laparoscopy (fine violin string adhesions)seen between the liver capsule and visceral peritoneum , treatment 3 weeks antibiotic per hepatitis cured 2 -Ritters syndrom or sexually acquired reactive arthritis, uveitis and rash 3 -PID 4 -Adult conjunctivitis
, 30% of")
HERPS SIMPLEX VIRUS Incurable STD HSV 1 caused oral lesion (cold sores), 30% of genital herps HSV 2 cause genital lesion and 90%of recurrent genital herps. The ferquency of reurranceis much heigher in type 2 than in type 1 Infection is frequently sub clinical, presentation can occur many years later as newly acquired infection 10 20% of infected person know that they are infected 70% of transmissions are from asymptomatic infected person with no visible lesion

n n C. F. PRIMARY HERPS Presents up to 3 weeks after acquisition wide spread lesion involve vulva, vagina , cx painful vesicles coalesce in to multiple ulcers, per urethral involvement may cause sever pain , urine retention , rectal infection after oro genital sex or anal intercourse , primary pharyngeal. Systemic symptoms may be also present such as fever, headache , malaise and lymphadenopathy. Acute cervicitis may be present. the lesion heal without scarring in 14 21 days

n n n RECURRENT HERPS After primary herpes, virus colonizes the neuron in the dorsal root ganglia establishing latent infection, intermittent infection when virus particles are produce and tract down the axons to the skin. Ulcer, vesicles in the same area or area supply by the same dermatome

The clinical diagnosis of genital herpes can be difficult, because the painful multiple vesicular or ulcerative lesions typically associated with HSV are absent in many infected persons. A patient's prognosis and the type of counseling needed depend on the type of genital herpes (HSV-1 or HSV-2) causing the infection; therefore, the clinical diagnosis of genital herpes should be confirmed by type-specific laboratory testing. Both typespecific virologic and type-specific serologic tests for HSV should be available in clinical settings that provide care to persons with or at risk for STDs. Persons with genital . herpes should be tested for HIV infection

Diagnosis Collecting serum from vesicle by syringe Swab the ulcer demonstrating the virus by electron microscopy Tissue culture Serological test differentiated between type 1 and 2

Treatment 1 analgesics 2 bathing in salt and water 3 lignocaine gel to sore area cyclovir 400 mg orally three times a day for 7– 10 days Acyclovir 200 mg orally five times a day for 7– 10 days Valacyclovir 1 g orally twice a day for 7– 10 day. OR Famciclovir 250 mg orally three times a day for 7– 10 days * Treatment can be extended if healing is incomplete after 10 days of therapy.

n n n n The spectrum of severity varies 1 asymptomatic shedding of virus 2 apparently trivial ulcers resembling small abrasion on the vulva, 3 locolized clusters of vesicles and ulcers over an area 1 2 cm diameter 4 wide spread or chronic ulceration resembling a primary infection can be seen in pregnant female if a women is immune suppressed, large atypical chronic ulcers may develop 5 a herpetic ulcer persisting for more than 1 month in ADIS individual DX Swabbing small ulcer in female if initial swab –ve repeated if ulcer recurs

Recurrent episodes Attack will resolve quickly with out specific treatment keep the area by washing with salt and water to avoid sexual intercourse until fully healed. Antiviral therapy for recurrent genital herpes (6 8 per year) can be administered either: as suppressive therapy to reduce the frequency of recurrences episodically to ameliorate or shorten the duration of lesions

n Some persons, including those with mild or infrequent recurrent outbreaks, benefit from antiviral therapy; therefore, options for treatment should be discussed. Many persons prefer suppressive therapy, which has the additional advantage. Safety and efficacy have been documented among patients receiving daily therapy with acyclovir for as long as 6 years and with valacyclovir or famciclovir for 1 year of decreasing the risk for genital HSV 2 transmission to susceptible person.

Recommended Regimens Acyclovir 400 mg orally twice a day Valacyclovir 500 mg orally once a day*(less effective than others with those with infequent recurrences) Valacyclovir 1 g orally once a day Famiciclovir 250 mg orally twice a day somewhat less effective for suppression of viral shedding

Episodic Therapy for Recurrent Genital Herpes Effective episodic treatment of recurrent herpes requires initiation of therapy within 1 day of lesion onset or during the prodrome that precedes some outbreaks. The patient should be provided with a supply of drug or a prescription for the medication with instructions to initiate treatment immediately when symptoms begin.

Recommended Regimens Acyclovir 400 mg orally three times a day for 5 days Acyclovir 800 mg orally twice a day for 5 days Acyclovir 800 mg orally three times a day for 2 days Valacyclovir 500 mg orally twice a day for 3 days Valacyclovir 1 g orally once a day for 5 days. OR Famciclovir 125 mg orally twice daily for 5 days. OR Famciclovir 1 gram orally twice daily for 1 day. OR Famciclovir 500 mg once, followed by 250 mg twice daily for 2 days
 acyclovir therapy should be provided for patients who have severe")
Severe Disease Intravenous (IV) acyclovir therapy should be provided for patients who have severe HSV disease or complications that necessitate hospitalization (e. g. , ) or CNS complications (e. g. , meningoencephalitis). The recommended regimen is acyclovir 5– 10 mg/kg IV every 8 hours for 2– 7 days or until clinical improvement is observed, followed by oral antiviral therapy to complete at least 10 days of total therapy. HSV encephalitis requires 21 days of intravenous therapy. Impaired renal function warrants an adjustment in acyclovir dosage.

COMPLECATIONS n n 1 Psychological distress 2 neurological involvement during primary herpes , aseptic meningitis , transverse myelitis, autonomic neuropathy 1 2 months resolve. HSV 2 cause encephalitis in adult 3 Herpes keratitis cause corneal scarring blindness 4 disseminated infection, pneumonitis, or hepatitis

Management of Sex Partners Symptomatic sex partners should be evaluated and treated in the same manner as patients who have genital herpes. Asymptomatic sex partners of patients who have genital herpes should be questioned concerning histories of genital lesions and offered type specific serologic testing for HSV infection.

n n very early vulvae affect small area, so antiviral treatment for 5 days for all patients presenting with the first attack even if clinical suspicious of 2 nd episodes An infected mother can transmit the virus to her infant during delivery resulting insignificant fetal mortality and morbidity.

n n n n SYPHILIS Systemic STD caused by treponema pallidum , the first manifestation painless ulcer (chancre), commonest site in (cx)pass unnoticed resolve with out treatment after few weeks. 2 nd syphilis as systemic eruption 1 non itchy maclopapular rash 3 Warts like (condylomata –lata) seen in intertrigon areas perianally 3 mucous patch, linear snail tract ulcer on mucosal surface 4 generilized L. N. sensoryneural deafness

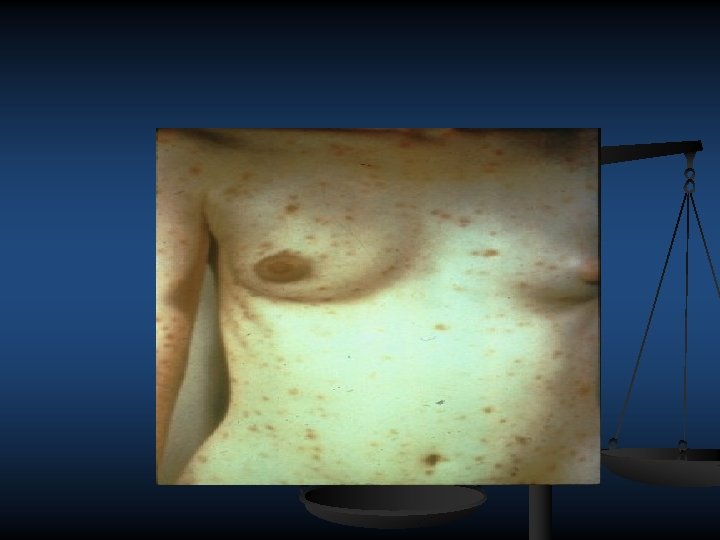


Second Stage Syphilis Flu-like symptoms and rash. Rash is brownish red and can appear on any part of the body.

n n n n n DX Primary syphilis by demonstrating M. O. by dark field microscopy –spiral M. O. (clear serum from the lesion) Serological test (fluorescent treponemal antibody) TPHT (TP haemagglutination assay) TPPA (T. P. particle agglutination) Non specific VDRL, RPR (rapid plasma regain) These test –ve in early primary syphilis 2 ndsyphilis 1 demonstrating M. O. from mucosal lesion 2 serelogical test +ve VDRL –ve with in years after 2 ndsyphilis –relapse for up to 2 years , infection can be transmitted to asexual partner

n n n TREATMENT Procain pencillin 1. 2 mu daily IM 12 day Benzathin pencillin 2. 4 million unit IM repeated after 7 days Doxycycillin 100 mg twice for 14 days Erythromycin 500 mg for 14 days If infection more than 1 year treatment extended to 21 days parental or oral for 28 days

HUMAN PAPILLOMA VIRUS 100 type, strain at least 40 of which can infect the genital area Most HPV infections are self limited and are asymptomatic or unrecognized causing hand warts can spread to genital area , asymptomatic infection may be carried for years the virus infection skin of the vulva , perineum the vagina cx, rectum orogenital contact leads to warts developing in mouth lips multiple slowly increase in size spread to perianal skin can ,

n n Oncogenic, high risk HPV infection (e. g. , HPV types 16 and 18) causes most cervical, penile, vulvar, vaginal, and oropharyngeal cancers and precancers whereas nononcogenic, low risk HPV infection (e. g. , HPV types 6 and 11) causes genital warts and recurrent respiratory papillomatosis

 that prevents")
HPV Vaccines There are several HPV vaccines n a bivalent vaccine (Cervarix) that prevents infection n with HPV types 16 and 18, a quadrivalent vaccine (Gardasil) that prevents n infection with HPV types 6, 11, 16, and 18, and a 9 valent vaccine that prevents infection with n HPV types 6, 11, 16, and 18, 31, 33, 45, 52, and 58.

The bivalent and quadrivalent vaccines offer n protection against HPV types 16 and 18, which account for 66% of all cervical cancers, and the 9 valent vaccine protects against five additional types accounting for 15% of cervical cancers. The quadrivalent HPV vaccine also protects against types 6 and 11, which cause 90% of genital warts.

All HPV vaccines are administered as a 3 dose series of IM n injections over a 6 month period, with the second and third doses given 1– 2 and 6 months after the first dose, respectively. The same vaccine product should be used for the entire 3 dose series. For girls, either vaccine is recommended routinely at ages 11– 12 years and can be administered beginning at 9 years of age (16); girls and women aged 13– 26 years who have not started or completed the vaccine series should receive the vaccine. The quadrivalent or 9 valent HPV vaccine is recommended routinely for boys aged 11– 12 years; boys can be vaccinated beginning at 9 years of age n

These tests should not be used for male partners of women with HPV or women aged <25 years, for diagnosis of genital warts, or as a general STD test.
. If left untreated, anogenital")
In most patients, treatment results in resolution of the wart(s). If left untreated, anogenital warts can resolve spontaneously, remain unchanged, or increase in size or number. Because warts might spontaneously resolve within 1 year

No definitive evidence suggests that any one n n recommended treatment is superior to another n limited data exist regarding the efficacy or risk for complications associated with combination therapy n Treatment regimens are classified as either patient applied or provider administered modalities

Recommended Regimens for External Anogenital Warts Patient-Applied: Imiquimod 3. 75% or 5% cream Podofilox 0. 5% solution or gel Follow up visits after several weeks of therapy Sinecatechins 15% ointment†

Imiquimod is a patient applied, topically active n immune enhancer that stimulates production of interferon and other cytokines. Imiquimod 5% cream should be applied once n at bedtime, three times a week for up to 16 weeks. Similarly, imiquimod 3. 75% cream should be n applied once at bedtime, but is applied every night
 is a patient applied n antimitotic drug that causes wart necrosis. Podofilox")
Podofilox (podophyllotoxin) is a patient applied n antimitotic drug that causes wart necrosis. Podofilox solution (using a cotton swab) or podofilox gel (using a finger) should be applied to anogenital warts twice a day for 3 days, followed by 4 days of no therapy. This cycle can be repeated, as necessary, for up to four cycles. The total wart area treated should not exceed 10 cm 2, and the total volume of podofilox should be limited to 0. 5 m. L per day. If possible, the health care provider should apply the initial treatment to demonstrate proper application technique and identify which warts should be treated
.")
Sinecatechins is a patient applied, green tea n extract with an active product (catechins). Sinecatechins 15% ointment should be applied three times daily (0. 5 cm strand of ointment to each wart) using a finger to ensure coverage with a thin layer of ointment until complete clearance of warts is achieved. This product should not be continued for longer than 16 weeks

Provider–Administered: Cryotherapy with liquid nitrogen or cryoprobe OR Surgical removal either by tangential scissor excision, tangential shave excision, curettage, laser, or electrosurgery OR Trichloroacetic acid (TCA) or bichloroacetic acid (BCA) 80%– 90% solution

TCA solution has a low viscosity comparable with that of water and can spread rapidly and damage adjacent tissues if applied excessively. A small amount should be applied only to the warts and allowed to drtreatment can be repeated weekly if necessary n

Recommended Regimens for Cervical Warts Cryotherapy with liquid nitrogen Surgical removal TCA or BCA 80%– 90% solution Management of cervical warts should include consultation with a specialist. For women who have exophytic cervical warts, a biopsy evaluation to exclude high grade SIL must be performed before treatment is initiated.

Recommended Regimens for Vaginal Warts Cryotherapy with liquid nitrogen. The use of a cryoprobe in the vagina is not recommended because of the risk for vaginal perforation and fistula formation. OR Surgical removal OR TCA or BCA 80%– 90% solution

n Female with warts are not at increase risk of cancer, screen done every 3 years, recent sexual partner should examine for genital warts and other STI


HIV INFECTION n Retro virus, single strand RNA 20% of those infected with HIV experience an acute seroconversion illness a few weeks after acquisition (fever , rash , generalized L. N)the steady decrease in immune function over few years and present as recurrent and oral , vaginal candidacies , herpes zoster , frequent prolonged episodes of oral , genital herpes or persistent warts regular administration of antifungal may be necessary to control candidacies with out treatment median time for AIDS 10 years onset defined by life threatening opportunistic infection or malignancies associated with immune deficiency.

NATURAL COURSE OF HIV/AIDS

Stage 1 - Primary n n n Short, flu like illness occurs one to six weeks after infection Mild symptoms Infected person can infect other people

Stage 2 - Asymptomatic n Lasts for an average of ten years n This stage is free from symptoms n There may be swollen glands n The level of HIV in the blood drops to low levels n HIV antibodies are detectable in the blood

Stage 3 - Symptomatic n The immune system deteriorates n Opportunistic infections and cancers start to appear.

Stage 4 - HIV AIDS n The immune system weakens too much as CD 4 cells decrease in number.

Opportunistic Infections associated with AIDS CD 4<500 n n n n Bacterial infections Tuberculosis (TB) Herpes Simplex Herpes Zoster Vaginal candidiasis Hairy leukoplakia Kaposi’s sarcoma

Opportunistic Infections associated with AIDS CD 4<200 n Pneumocystic carinii n Toxoplasmosis n Cryptococcosis n Coccidiodomycosis n Cryptosporiosis n Non hodgkin’s lymphoma

TB & HIV CO-INFECTION n n TB is the most common opportunistic infection in HIV and the first cause of mortality in HIV infected patients (10 30%) 10 million patients co infected in the world.

n n n VOROLOGY is a retrovirus , single strand of RNA, reverse transcriptase is carried with in the core to enable proviral DNA to be produce in an infected cell. the outer membrane protein gp 120 , bind to cd 4 receptors which are present on Helper lymphocytes macrophages , dendritic cell and microglial cell. Another viral protein P 24 surrounds the RNA and enzymes present with in the core of the virus which enters the cytoplasm of an infected cell the drugs target reverse transcriptase or viral proteases

n n n DX 1 antibodies to gp 120 2 P 24 antigen during seroconversion s detectable 3 monitor the disease by measuring the level of CD 4 lymphocyte in the peripheral blood. 4 PCR technology we can measure the viral concentration of viral RNA in the plasma high level so rapid disease development

Through Bodily Fluids Blood products n Semen n Vaginal fluids n

Intra. Venous Drug Abuse Sharing Needles Without sterilization Increases the chances of n contracting HIV Unsterilized blades n n

Through Sex Unprotected Intercourse Oral n Anal n n

Mother-to-Baby n n n Before Birth During Birth After birth during breast feeding

n n Transmission In developing countries HIV spread through vaginal intercourse In developed countries through homosexual or I. V. drug user and heterosexual Genital ulcer Chlamydia , GC , BV. All risk factor for transmission and acquisition , so good control of STD should decrease incidence of HIV infection

n the aim of therapy is to reduce the level in the plasma to zero with a combination of antiretroviral agents with each cycle of replication of virus , which takes 48 h single point mutation arise , which will confer reduced sensitivity to anti viral agents if therapy is effective CD 4 lymphocyte count rises progressively and at least partial immune restoration occurs HIV , infects long lived memory cells, so eradicated and cure is unlikely ever after several years of treatment

n Combination of antiretroviral drugs are prescribed these include 2 or more of nucleoside analogue reverse transcriptase inhibitors (zidovudine) and non nucleoside analogue reverse transcriptase inhibitors(nevirapine) and one or more of protease inhibitors(nelfinaver)

n n If succeful the immune system improves after a few months These drug have potential interaction with Other drug , they increase the rate of break down of synthetic estrogen in oral CCP If immune deficiency has already occur treatment and prevention opportunistic infection are needed regular antifungal agent to control oral and vaginal candidacies, ganciclovir to prevent CMV infection
 drugs for HIV/AIDS can generally use")
HIV and Contraception Generally, women taking antiretroviral (ARV) drugs for HIV/AIDS can generally use any contraceptive method. There is one exception: Ritonavir or ritonavir boosted ARVs may make combined hormonal methods and progestin only pills less effective. These women can use progestin only injectables, implants, and other methods. n Women taking only other classes of ARVs can use any hormonal method. Contraception with protection n n Male condom (latex and vinyl) Female condom Nonoxynol 9 (antiviral spermicidal cream)1 Diaphragm 1 1 Partial protection if used without condom 96
 present despite aggressive surgical")
GYNAECOLOGICAL MANIFESTATION n n n 1 Hpv infection (genital warts) present despite aggressive surgical treatment , so persistent atypical warty lesion of skin or vulva should be biopsie 2 HPV 16 18 can result in ca cx , VIN, cytological of cx should done annually 3 PID requires longer courses of antibiotic 4 Post partum endometritis is common 5 HSV eruption of 2 nd genital herpes may become wide spread sever and persist for weeks if not diagnosed and treated, genital herpes often present as deep painful ulceration 6 Although all HIV infected female are urged to use condoms to prevent them transmitting the infection to others they should also be advised to used a more reliable form of contraception.

n Medication prescribed for HIV infection women plan to become pregnant the means of reduction he risk of vertical transmission should be discuses with her as should to the consequences for the child of possibly losing his or her mother in child hood if the partner is HIV negative the couple should be assisted to perform artificial insemination by providing information and syringes and pipettes , infertility treatment to HIV infected women controversial
 is a DNA virus that is")
Hepatitis B Virus The hepatitis B virus (HBV) is a DNA virus that is transmitted mainly in blood, but also in other body fluids such as saliva, semen and vaginal fluid. Drug users who share needles are at high risk n

n Clinical features n n n The HBV has an incubation period of 6 weeks to six months Hepatitis B is a virus that infects the liver but many people with hepatitis B viral infection have nosymptoms.

Diagnosis: HBs. Ag is not infec tious , HBs. Ag is detectable in serum in almost all cases of acute and chronic HBVe. Ag can be detected in liver tissue of persons with acute or chronic HBV infect. HBe. Ag is detected in the serum of persons with high virus titers and indicates high infectivity. The presence of anti HBs indicates immunity to HBV. ) Antibody to HBe. Ag (anti-HBe) becomes detectable when HBe. Ag is lost and is associated with low infectivity. Serum antibody to HBc. Ag (Ig. M anti HBc) indicates recent infection with HBV. n

Prevention: 1 Transmission that can be prevented through vaccination and immunization active vaccine provides ongoing protection from subsequent exposure in the household. 2 women who screen negative her partner positive barrier method should use to provide protection against acquiring the infection.

Two products have been approved for hepatitis B n prevention: hepatitis B immune globulin (HBIG) for postexposure prophylaxis and hepatitis B vaccine HBIG provides temporary (i. e. , 3– 6 months) n protection from HBV infection (The recommended dose of HBIG is 0. 06 m. L/kg. Hepatitis B vaccine contains HBs. Ag produced in n yeast by recombinant DNA technology and provides protection from HBV infection n

Three different 3 dose schedules for both n monovalent hepatitis B vaccines (i. e. , Engerix B and Recombivax HB); these vaccines can be administered at 0, 1, and 6 months; 0, 1, and 4 months; and 0, 2, and 4 months. A 4 dose schedule of Engerix B at 0, 1, 2, and 12 months is licensed for all age groups. If the vaccine series is interrupted after the first or second dose of vaccine, the missed dose should be administered as soon as possible. The series does not need to be restarted after a missed dose

If indicated, anti HBs testing should be performed 1– 2 months after administration of the last dose of the vaccine series. Persons determined to have anti HBs levels of <10 m. IU/m. L after the primary vaccine series should be revaccinated with a 3 dose series and tested again for anti HBs 1– 2 months after the third dose. Persons who do not respond to revaccination should be tested for HBs. Ag. If HBs. Ag positive, the person should receive appropriate management

Management Women who screen positive for hepatitis B should be referred to a hepatologist for ongoing monitoring for the long term consequences of chronic infection, for example hepatocellular carcinoma.

Chancroid Caused by ; H. ducreyi The combination of a painful genital ulcer and tender Suppurative inguinal adenopathy suggests the diagnosis of Chancroid A probable diagnosis of Chancroid, for both clinical and surveillance purposes, can be made if all of the following criteria are met: 1) the patient has one or more painful genital ulcers; 2) the patient has no evidence of T. pallidum infection by dark field examination of ulcer exudate or by a serologic test for syphilis performed at least 7 days after onset of ulcers; Dr. T. V. Rao MD 107
 the clinical presentation, appearance of genital ulcers and, if present, regional lymphadenopathy")
Chancroid 3) the clinical presentation, appearance of genital ulcers and, if present, regional lymphadenopathy 4) a test for HSV performed on the ulcer exudate is negative. Dr. T. V. Rao MD 108

Chancroid A definitive diagnosis of Chancroid requires the identification of H. ducreyi on special culture media that is not widely available from commercial sources; even when these media are used, sensitivity is <80% Dr. T. V. Rao MD 109

Treatment Successful treatment for chancroid cures the infection, resolves the clinical symptoms, and prevents transmission to others. In advanced cases, scarring can result despite successful therapy. Recommended Regimens Azithromycin 1 g orally in a single dose. OR Ceftriaxone 250 mg IM in a single dose. OR Ciprofloxacin 500 mg orally twice a day for 3 days. OR Erythromycin base 500 mg orally three times a day for 7 days Azithromycin and ceftriaxone offer the advantage of single dose therapy

Management Considerations Patients should be tested for HIV infection at the time chancroid is diagnosed. If the initial test results were negative, a serologic test for syphilis and HIV infection should be performed 3 months after the diagnosis of chancroid.

Follow-Up Patients should be re examined 3– 7 days after initiation of therapy. If treatment is successful, ulcers usually improve symptomatically within 3 days and objectively within 7 days after therapy.
 the diagnosis is incorrect,")
n n n If no clinical improvement is evident, 1) the diagnosis is incorrect, 2) the patient is coinfected with another STD, 3) the patient is infected with HIV, 4) the treatment was not used as instructed, or 5) the H. ducreyi strain causing the infection is resistant to the prescribed antimicrobial.

. The time required for complete healing depends on the size of the ulcer; large ulcers might require >2 weeks Clinical resolution of fluctuant lymphadenopathy is slower than that of ulcers and might require needle aspiration or incision and drainage, despite otherwise successful therapy. Incision and drainage might be preferred because of reduced need for subsequent drainage procedures.

Management of Sex Partners Regardless of whether symptoms of the disease are present, sex partners of patients who have chancroid should be examined and treated if they had sexual contact with the patient during the 10 days preceding the patient's onset of symptoms.
 Granuloma inguinale is a genital ulcerative disease caused by the intracellular")
Granuloma Inguinale (Donovanosis) Granuloma inguinale is a genital ulcerative disease caused by the intracellular gram negative bacterium Klebsiella granulomatis (formerly known as Calymmatobacterium granulomatis). The disease occurs rarely in the United States, although it is endemic in some tropical and developing areas, including India; Papua, New Guinea; the Caribbean; central Australia; and southern Africa (192, 193). Dr. T. V. Rao MD n 116
 Clinically, the disease is commonly characterized as painless, slowly progressive ulcerative")
Granuloma Inguinale (Donovanosis) Clinically, the disease is commonly characterized as painless, slowly progressive ulcerative lesions on the genitals or perineum without regional lymphadenopathy; subcutaneous granulomas (pseudoboboes) might also occur. The lesions are highly vascular (i. e. , beefy red appearance) and bleed easily on contact. Dr. T. V. Rao MD n 117
 The causative organism is difficult to culture, and diagnosis requires visualization")
Granuloma Inguinale (Donovanosis) The causative organism is difficult to culture, and diagnosis requires visualization of dark staining Donovan bodies on tissue crush preparation or biopsy. No FDA cleared molecular tests for the detection of K. granulomatis DNA exist, but such an assay might be useful when undertaken by laboratories that have conducted a CLIA verification study. Dr. T. V. Rao MD n 118
 The causative organism is difficult to culture, and diagnosis requires visualization")
Granuloma Inguinale (Donovanosis) The causative organism is difficult to culture, and diagnosis requires visualization of dark staining Donovan bodies on tissue crush preparation or biopsy. No FDA cleared molecular tests for the detection of K. granulomatis DNA exist, but such an assay might be useful when undertaken by laboratories that have conducted a CLIA verification study. Dr. T. V. Rao MD n 119
 Clinically, the disease is commonly characterized as painless, slowly progressive ulcerative")
Granuloma Inguinale (Donovanosis) Clinically, the disease is commonly characterized as painless, slowly progressive ulcerative lesions on the genitals or perineum without regional lymphadenopathy; subcutaneous granulomas (pseudoboboes) might also occur. The lesions are highly vascular (i. e. , beefy red appearance) and bleed easily on contact. Dr. T. V. Rao MD n 120
 is n caused by C. trachomatis serovars")
Lymph granuloma Venereum Lymph granuloma venereum (LGV) is n caused by C. trachomatis serovars L 1, L 2, or L 3. The most common clinical manifestation of LGV among heterosexuals is tender inguinal and/or femoral lymphadenopathy that is typically unilateral. Dr. T. V. Rao MD 121

Lymph granuloma Venereum Diagnosis is based on clinical suspicion, n epidemiologic information, and the exclusion of other Aetiologies for proctocolitis, inguinal lymphadenopathy, or genital or rectal ulcers. C. trachomatis testing also should be conducted, if available. Dr. T. V. Rao MD 122

Lymph granuloma Venereum Genital and lymph node specimens (i. e. , lesion swab or bubo aspirate) can be tested for C. trachomatis by culture, direct immunofluorescence, or nucleic acid detection. NAATs for C. trachomatis are not FDA cleared for testing rectal specimens, although some laboratories have performed the CLIA validation studies that are needed to provide results for clinical management. Additional molecular procedures (e. g. , PCR based genotyping) can be used to differentiate LGV from non LGV C. trachomatis, but these are not widely available. Dr. T. V. Rao MD n 123

THANK YOU
- Slides: 124