Sexual health screening in general practice Chlamydia Trachomatis




 clinics")








 • Urine tests or swabs • High")
















")








 discharge Satellite lesions")









 is a flagellated protozoon • Exclusively")



- Slides: 56
Sexual health screening in general practice Chlamydia, Trachomatis, Gonorrhea, Bacterial Vaginosis and Candida
Common STI’s in General Practice ØChlamydia ØGonorrhea ØTrichomonas ØOther Non- STI’s but genital infections are : ØCandida ØBacterial Vaginoses.
Quick Preview • Genital Chlamydia most common STI : 2012. 206, 912 people tested positive • 64% were under 25 • Highest in men aged 20 -24, women 16 -19 • Highest rates in women 20 -24 & 16 -19 • Rates of STI’s highest in residents of Urban Areas : In London
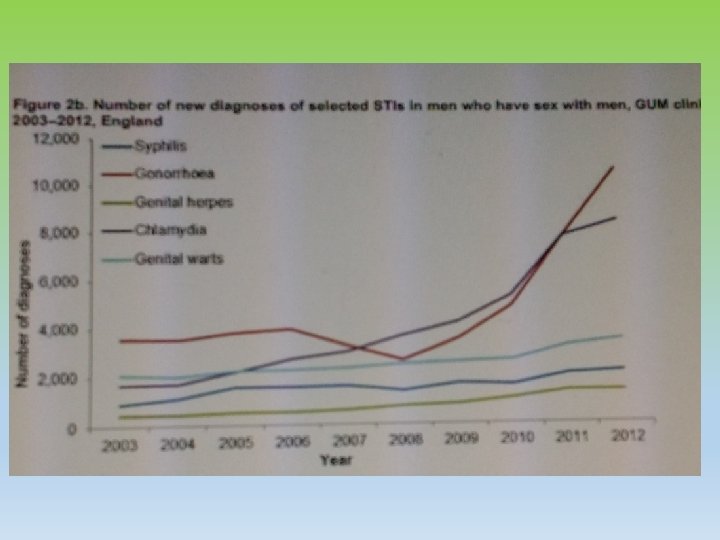
Epidemiology • The graph shows the various STI diagnoses at GUM (genitourinary medicine) clinics in the UK between 2000 and 2010.
Epidemiology • STI diagnosis rose by 5% in 2012 ( up to 448422 from 428, 255 in 2011) • Combined high STI rates in England suggest too many people are putting themselves at risks through unsafe sex esp, young adults and MSM ( men having sex with men). • Chlamydia rose by 46% • Genital warts rose by 16% • Genital herpes rose by 7 % • New Diagnosis of Gonorrhea rose by 21 % from 2011 -2012. 37% in MSM. • Ref: PHE press release, sexually transmitted infection in England 2012, HPR 7 ( 23), 7 /6/2013. • PHE : ‘ Gonorrhea resistance action plan for England wales Feb 2012.
Reasons • No one Knows Clearly Why • Maybe increase in notification and data collection • Global Threat of antibiotics may have contributed to the rise. • Gonorrhoea resistance Action Plan for England wales launched by PHE in 2013. • 2012, > 1. 7 million chlamydia tests were undertaken > 136, 000 diagnosis made.
Chlamydia v. Chlamydia stems from a bacterium chlamydia trachomatis v. Women with chlamydia can infect their newborn infant during delivery v. Symptoms appear 7 -21 days after infection, different for men, women and children. v. Can test 14 days after exposure
Symptoms in Men üInflammation of the urethra üStinging feeling when passing urine üPain or tenderness in the testicles. üAsymptomatic in over 50% üRectal discomfort/proctitis
Signs in Men • Normal • Urethral discharge and/or dysuria • Local complications such as epididymitis
Symptoms in Women • Purulent vaginal discharge • Pain caused by pelvic inflammation • Dysuria • Post coital or inter-menstrual bleeding. • Asymptomatic in 80%
Signs in women • Normal • Cervicitis, muco-purulent discharge • Cervical contact bleeding • Local complications e. g. bartholinitis, signs of pelvic infection
Chlamydia in men and women 43. Mucopurulent cervicitis
Diagnosis • Nucleic acid amplification tests (NAATS) • Urine tests or swabs • High sensitivity and specificity • Chlamydia can not be diagnosed on genital swabs sent for • MC&S e. g. HVS in charcoal swabs
Treatment • Doxycycline 100 mg x 7 days • Azithromycin 1 g stat if compliance is an issue • Alternative regimens • Erythromycin 500 mg bd x 14 days( if pregnancy possible or breast feeding) • Erythromycin 500 mg qds x 7 • Ofloxacin 200 mg bd/400 mg od x 7 days
complications Ø Ø Ø PID/ epididymitis In pregnancy Low birth weight Post-partum endometritis Neonatal conjunctivitis and pneumonia Reactive arthritis In women, ascending infection leads to pelvic inflammatory disease: endometritis, salpingitis, tubal damage, and chronic pelvic pain. PID=the risks of ectopic pregnancy and infertility. Perihepatitis (Fitz. Hugh Curtis Syndrome) and Reiter’s syndrome Autoinoculation may result in chlamydial conjunctivitis
Contact tracing/partner notification • Partner notification should be discussed with all patients identified with genital chlamydial infection. All recent (last 6 months or last previous partner whatever is longer) and current sexual partner • Invited to attend for evaluation. • Treatment should be given even if tests are negative
National Chlamydia Screening Programme • Targets under 25’s • Free and confidential testing • Many outlets: pharmacy, GP’s, DOSH, college and /university's/club toilets! • Website – easy to order postal kits and signposts to local clinics/pharmacies for drop in
Patient Advice • If Chlamydia Trachomatis is left untreated it could lead to serious complications • Need to treat sexual partners • Abstain from sexual intercourse (even with a condom) including oral sex until completion of therapy ( wait 7 days if treatment with Azithromycin) • Side effects of treatment • Advice on safer sexual practices and how to avoid infection in the future
Follow up Emphasise that partner notification has taken place. We can only advise, cannot enforce. • Exclude re infection • Ensure compliance of medication. • Re test after 3 months (BASHH 2013)
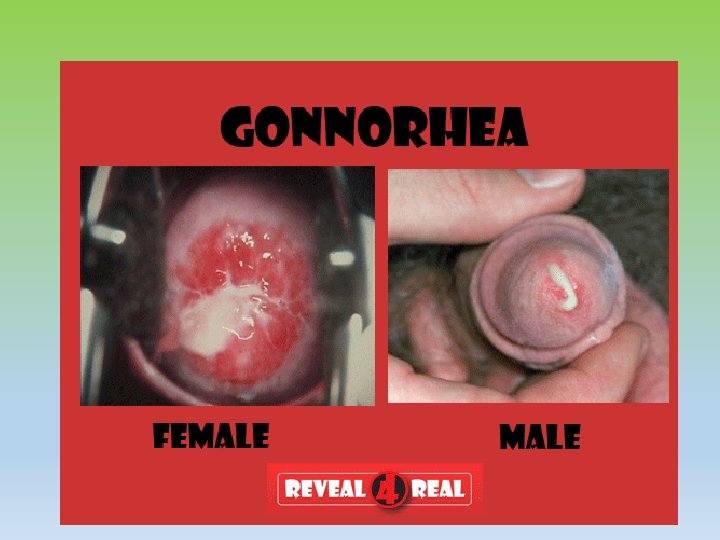
Gonorrhoea • Caused by Neisseria gonorrhoea loves moist, warm areas • In women the cervix is the most common site of infection. The disease can also spread to the uterus and fallopian tubes • Pelvic inflammatory disease can be caused if untreated leading to infertility • Pregnant women can pass it on to the newborn infant when normal delivery leading to severe conjunctivitis
Signs and Symptoms • Early symptoms are often mild, and many women who are infected have no visible symptoms of the disease • Painful burning sensation while urinating Yellowish or bloody discharge from the vagina • Bleeding between periods • Abdominal pain
Symptoms in Men • Burning micturition • Yellowish-white discharge from the penis: also called mucoid from the urethra • Local complications in men Epididymitis Infection of various penile glands
Symptoms in women • Cervicitis • Local complications in women • Discharge mucoid purulent • Bartholinitis • Cervical excitation • Signs of upper genital tract infection • endometritis
Other signs and symptoms • General S/S if affected in other areas include: • Rectal itching • Pharyngeal infection is usually asymptomatic ( If infection has occurred via oro-genital route) • Less commonly disseminated infection occurs by haematogenous spread. • Complications include septicaemia, arthritis, tenosynovitis and skin lesions
Diagnosis • Gonorrhoea and Chlamydia can be isolated from an endocervical swab taken in primary care • Other STIs in particular co-exist with Chlamydia infection and trichomonas
Diagnosis • Isolated from an endocervical swab taken • Other STI’s in particular chlamydia and trichomonas coexist with GC and all patients should be screened for these. • NAATs testing for both gonorrhoea and chlamydia
treatment • Thorough evaluation and tests of cure are necessary to ensure eradication of the organism • Patients should be managed in a GUM clinic • F/U at GUM clinic as symptomatic improvement with treatment does not guarantee eradication of the gonococcus.
Treatment updated 2012 FEB • Gonorrhoea Treatment • In view of increasing antibiotic resistance to gonorrhoea, the British Association now recommend that all gonorrhoea be treated with • Ceftriaxone 500 mg im stat + azithromycin 1 g stat po • We recognise that many surgeries may not have the facilities to administer IM ceftriaxone and these surgeries may wish to refer to the department of sexual health) for treatment of gonorrhoea.
Updated treatment • However if there is ANY DOUBT that the client will attend DOSH, or if for any reason an im injection is inappropriate, these second line regimens are also indicated and should be given by the GP • Cefixime 400 mg po stat + + azithromycin 1 g stat po • OR • Azithromycin 2 g po stat • All clients with a diagnosis of gonorrhoea should have a test of cure to ensure eradication of the organism. • Also please remember that any diagnosis of gonorrhoea made on NAATS testing ALSO requires a culture specimen before treatment, to look for antimicrobial sensitivities
Contact tracing/partner notification • All recent (last 3 months or previous partner if longer) and current sexual partners • In some instances epidemiological treatment is given to named contacts
Bacterial Vaginosis Causative Organism : reduction in lactobacilli and an overgrowth of predominantly anaerobic organisms (Gardnerella vaginalis, Prevotella spp, Mycoplasma hominis, Mobiluncus spp) in the vagina with an increase in vaginal p. H.
Transmission • Can arise and remit spontaneously in women regardless of sexual activity. • Therefore no contact tracing and partner notification is required.
Signs and Symptoms • Asymptomatic • Offensive fishy-smelling vaginal discharge • Less commonly vaginal irritation or mild low abdominal discomfort • Examination may reveal a thin, greyish/white homogenous discharge
Diagnosis • Thin, grey/white homogenous discharge • p. H of vaginal fluid > 4. 5 ( usually not done in general practice) • Positive amine test ( release of fishy odour on adding an alkali-10%KOH) • Clue cells on microscopy, available on most HVS
Treatment • Symptomatic women, pregnant women with a history of recurrent miscarriage and women undergoing some surgical procedures • Metronidazole 400 -500 mg twice daily for 5 -7 days or 2 g stat • Intravaginal clindamycin cream (2%) once daily for 7 days. • Clindamycin 300 mg bd x 7 days. Non-drug treatments
General Advice • Patients should avoid vaginal douching • Use of shower gel • Use of antiseptic agents or shampoo in the bath • No F/U is needed. Recurrence is very common (up to 50% by 3 months) and can be difficult to manage; if so specialist advice may be beneficial
What is this?
Thrush Commonest species is Candida albicans. Symptoms Pruritis Vulval/vaginal soreness Superficial dyspareunia discharge
Signs Vulvo-vaginitis Swelling Linear fissures Variable +/- (non-offensive) discharge Satellite lesions
Diagnosis in primary care • Clinical p. H< 5 • High Vaginal swab ( HVS) but 10 -20% women are asymptomatic vaginal carriers • Tests may be negative if treated recently.
Management • If s/s strongly suggest treat as candida • Recommended regimen • Anti fungal pessary +/- cream for external area • Fluconazole 150 mg stat • Routine advice is more important.
The image above shows a severe case of vaginal thrush with Candida albicans fungal growth at the mouth and around the sides of the cervix.
Associated Factors • Avoid precipitating factors such as soaps, shower gels, sanitary towels which may increase the risk of local response. • ? Wet wipes- used to clean vulval areas
Genital herpes
Herpes Simplex Virus • HSV 1 and 2 • Can infect either mouth or genitals • Cross infect due to autoinoculation • Transmitted by close physical contact when virus is shredded by infected individual • Sporadic shredding can occur even if no active lesions • Lifelong infection with episodic symptoms
Herpes signs and symptoms • Multiple painful blisters • Beware of singles painless blister - ? Chancre of primary syphilis • Malaise – febrile flu like illness • Tingling pain in infected area • Tender lymphadenitis • Local odeama First episode can last 3 w + Recurrent episodes- psychological affects
Complications • Secondary infection of lesions • Auto inoculation to fingers and adjacent skin • Urinary retention • Aseptic meningitis
Management/treatment • Consider referral to DOSH if same day available , if not • Swab base of blister using viral swab (help to know which type HSV) • NATT testing most areas now as better detection rates – check with your local labs What helps? • Saline bathing • Topical anaesthesia eg lidocaine ointment • Oral analgesia • Oral antivirals – more effective than topical ones and no benefit on combining treatments- aciclovir first choice most prescribers • Follow up with DOSH review of recurrent or frequent attacks
Trichomonas Vaginalis • Causative organism Trichomonas vaginalis (TV) is a flagellated protozoon • Exclusively sexually transmitted • 50% of women are asymptomatic • Discharge if present is thin, watery, yellow, offensive, frothy • Can be reported on cervical cytology
Thin, watery discharge from cervix due to TV and strawberry discolouration on the cervix due to TV
References www. bashh. org www. fsrh. org