Severe Sepsis and Septic Shock Management Dr Alex

















 70 60 50 Sepsis 6 40 Resusc Both 30 Mortality 20")
 Mortality % 567 (100) 34. 7 Sepsis Six 347")



 For each hour’s")



- Slides: 30
Severe Sepsis and Septic Shock Management Dr Alex Hieatt, EM Consultant MEHT Dr Ron Daniels, Chair of the UK Sepsis Trust and Global Sepsis Alliance (Slides with permission. )
Questions What defines the sepsis syndrome? What defines severe sepsis? What defines septic shock? What is the single most important intervention in the management of severe sepsis and septic shock? 5. How often is 4 achieved within an hour? 6. What is the mortality from septic shock? 1. 2. 3. 4.
Questions 7. How many patients die each year in the UK from severe sepsis and septic shock? 8. How many people die each year in the UK from lung cancer? 9. How many people die each year in the UK from bowel cancer and breast cancer combined? 10. How much does sepsis cost the UK health economy each year?
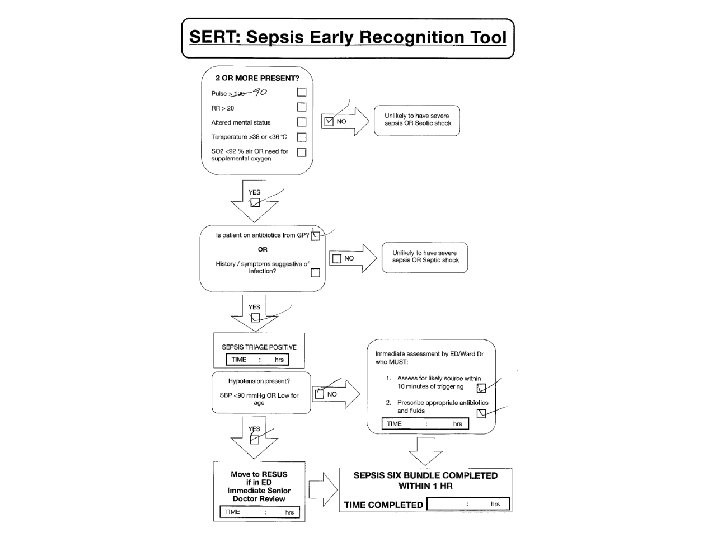
Answers �Sepsis syndrome � 2 SIRS criteria � HR > 90 � RR > 20 � T <36 or >38⁰C � Altered mental status � WBC <4 or >12 x 109 /L � BM >7. 7 mmol/L in a non diabetic �Suspected or newly diagnosed infection
Severe Sepsis = Sepsis syndrome + evidence of organ dysfunction Clinical �Need for O 2 pre hospital or on admission �Low blood pressure SBP<90 mm. Hg OR SBP drop >40 mm. Hg from normal OR MAP <65 mm. Hg OR DBP<60 �Not passed urine for > 8 hours OR UO< 0. 5 mls/kg/hr for 2 hours �Jaundiced �New confusion or decreased conscious level Chemical �INR > 1. 5 OR APTT > 60 s �Platelets <100 x 109 /L �Lactate >2 mmol/L �Creatinine>177 µmol/L OR Rise of > 50% over baseline �Bilirubin > 37 µmol/L
Septic Shock �Severe Sepsis and: �Lactate > 4 mmol/L �Refractory hypotension after 30 mls/kg ofvolume resuscitation
Dr Ron Daniels http: //www. youtube. com/watch? v=po. N 0 u. B BJem. M
Breast cancer
Breast cancer
Bowel cancer Breast cancer
Breast cancer Bowel cancer Annual U K sepsis d eaths
Global Sepsis Alliance / UK Sepsis Trust
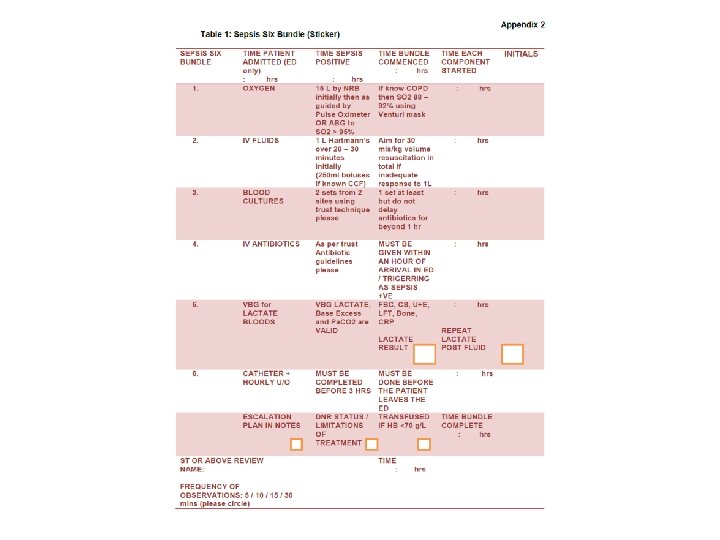
The Sepsis Six 1. Give high-flow oxygen via non-rebreathe bag 2. Take blood cultures and consider source control 3. Give IV antibiotics according to local protocol 4. Start IV fluid resuscitation Hartmann’s or equivalent 5. Check lactate 6. Monitor hourly urine output consider catheterisation within one hour. . plus Critical Care support to complete EGDT
Perspective Severe Sepsis 240 No. cases per 100, 000 per annum NNT ‘basic’ care NNT invasive care Acute coronary syndrome 208 Sepsis Six (our data) 4 Clopidogrel 48 First hour antibiotics 6 β-blockade 42 Aspirin 26 Thrombolysis 15 PCI over thrombolysis 33 EGDT (Rivers) Resusc Bundle (SSC) 6 18
Compliance, GHH (%) 70 60 50 Sepsis 6 40 Resusc Both 30 Mortality 20 10 0 Apr-09 Jun-09 Aug-09 Oct-09
Mortality Total Cohort size (%) Mortality % 567 (100) 34. 7 Sepsis Six 347 (61. 2) 44. 0 Sepsis Six 220 (38. 8) 20. 0 RRR % (‘NNT’) - 46. 6 (4. 16)
First hour antibiotics in 27%. . .
Begin IV antibiotics as early as possible, and always within the first hour of recognising severe sepsis (1 D) and septic shock. (1 B) Citation: Kumar A et al. Crit Care Med 2006: 34(6) Retrospective, 15 years, 14 sites n = 2, 154 median 6 h, 50% administered in 6 h Only 5% first 30 minutes- survival 87% 12% first hour- survival 84%
Effective Antimicrobial Therapy & Survival in Septic Shock 1. 0 survival fraction 0. 8 0. 6 0. 4 0. 2 0. 5 0. 51 12 23 34 45 56 69 912 12 -2 24 4 -3 36 6 + 0. 0 0 - fraction of total patients cumulative antibiotic initiation time from hypotension onset (hrs) Kumar et al. CCM. 2006: 34: 1589 -96.
Running average survival in septic shock based on antibiotic delay (n=2154) For each hour’s delay in administering antibiotics in septic shock, mortality increases by 7. 6% Funk and Kumar Critical Care Clinics 2011 (in press)
For each year, for every 100 k in the local population. . 20 lives saved 285 fewer bed days 168 fewer CC bed days Direct costs for survivors reduced by £ 0. 25 M For Italy, that’s 12, 200 lives and € 182 million. Every year.
Useful Tools file: ///C: /Users/ali/Desktop/S 4/Survive%20 Sepsis%20 on%20 the%20 App%20 Store%20 o n%20 i. Tunes. htm https: //itunes. apple. com/gb/app/survivesepsis/id 580791653? mt=8 http: //www. youtube. com/watch? v=Cr. UHn YIZbp. M https: //itunes. apple. com/gb/app/nhsscotland-news-sepsisscreening/id 657497806? mt=8