Severe Myocarditis A 2012 update Alain Combes Service

Severe Myocarditis: A 2012 update… Alain Combes Service de Réanimation i. CAN, Institute of Cardiometabolism and Nutrition Hôpital Pitié-Salpêtrière, AP-HP, Paris Université Pierre et Marie Curie, Paris 6 www. reamedpitie. com

Definition - Etiologies ¢ ¢ ¢ «Myocarditis» is defined as inflammation of the heart muscle Histology: cellular infiltrate and myocyte necrosis Etiologies: l Infectious diseases • Viruses: Coxsackie, Adenovirus, HIV, Parvovirus B 19, HHV 6 (H 1 N 1) • Bacteria • Parasites (Toxoplasma, Chagas) • Fungi l l Hypersensitivity (Drugs) Autoimmune and systemic diseases • Lupus, Wegener, Eosinophilic, Sarcoidosis, Giant cell l l Myocardial toxins (Cocaine, chemotherapy) Peripartum

¢ 6. 3 millions military recruits over 25 yrs l l 126 non-traumatic sudden deaths, autopsy performed 10% of myocarditis-related deaths

Clinical manifestations ¢ ¢ From asymptomatic EKG abnormalities to overt cardiac failure… Clinical features: l l l Preceding viral illness, flu-like syndrome Fever Chest pain, mimicking acute coronary syndromes Tachycardia Arrhythmia Sudden death: • 10% of cases (Eckart, Ann. Int. Med, O 4) l Clinical signs of heart failure • Minimal, slow evolution • Fulminant, leading to refractory cardiogenic shock in a few days

EKG ¢ EKG findings l l l l ¢ Sinus tachycardia Diffuse ST-T wave abnormalities Prolonged QT interval Bundle branch block (LBBB++) Myocardial infarction pattern Complete heart block Supraventricular tachyarrhythmias Ventricular tachyarrhythmias May be normal…

EKG mimicking AMI

EKG: LBBB

Laboratory Findings
")
Biology: Troponin (Smith, Circ, 97)

Many patients with acute/fulminant myocarditis will undergo coronary artery angiography…

Other laboratory findings ¢ Non specific tests l l l ¢ Leucocytosis/leucopenia, Eosinophilia+++ Mononucleosic syndrome Sedimentation rate, CRP, PCT… Specialized tests l Virological diagnosis • Serology (limited value) • Cultures: throat and stools • PCR (blood, CSF, tissues) l Inflammation: • Antinuclear Ab, ANCA, Angiotensin Conversion Enzyme ¢ Research tests l l Autoantibodies (mitochondria, myosin, b-receptor) Immunohistochemical myocardial studies (research)

Doppler Echocardiography

¢ Fulminant myocarditis Markedly decreased LV EF l Near normal LV dimension l Increased septal thickness l ¢ Acute myocarditis Markedly decreased LV EF l Dilated LV l Normal septal thickness l

Doppler Echocardiography ¢ Other findings Regional wall motion abnormalities l Diastolic dysfunction l Change in echocardiographic image texture: l • Increased brightness • Heterogeneity Thrombi l Pericardial effusion l

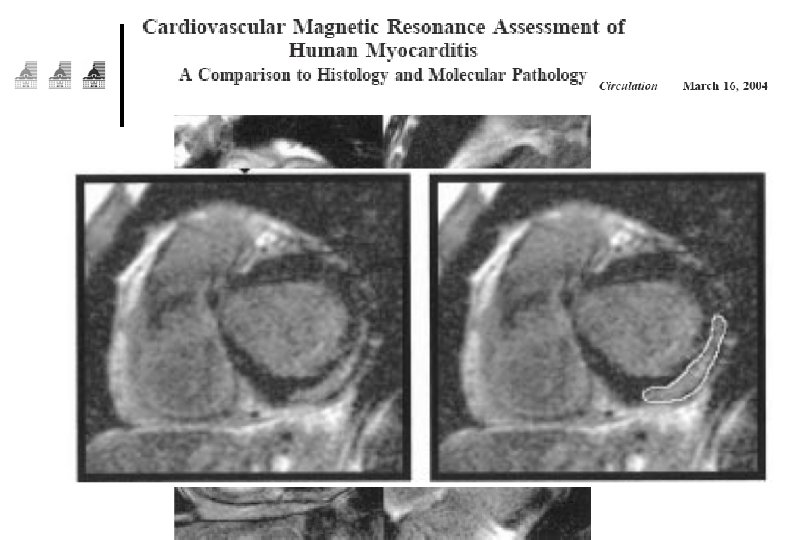
Cardiac MRI… The new diagnostic gold standard?

Cardiac MRI ¢ ¢ Combination of l T 1 -weighted and T 2 -weighted l Gadolinium contrast-enhanced MRI +++ Visualize localization, activity and extent of inflammation l l One or several foci in the myocardium Foci most frequently located in lateral free wall Frequent subepicardial lesions Can guide myocardial biopsies+++

Still indication for myocardial biopsies?
 l Active")
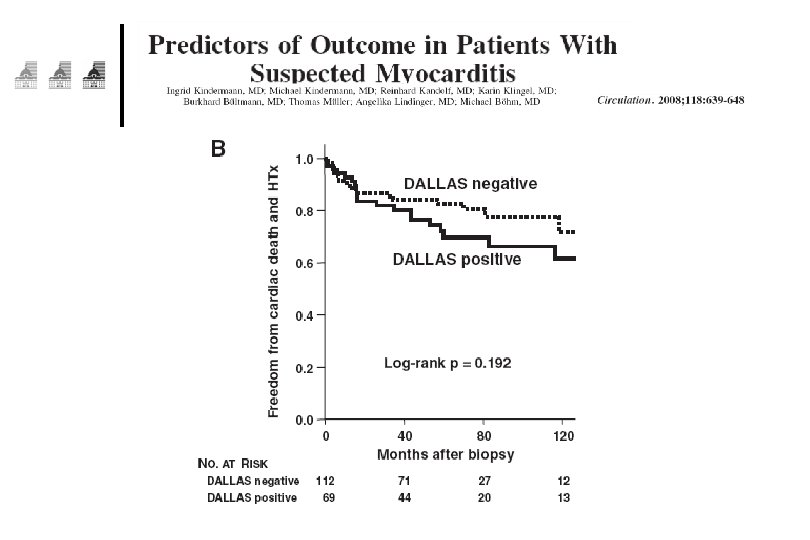
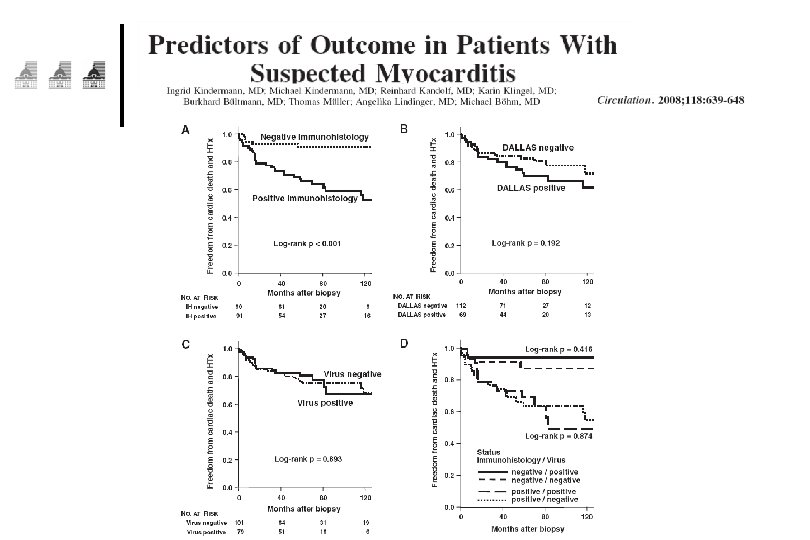
Histology: Dallas Criteria ¢ ¢ 3 histological grades (Aretz, Hum Pathol, 87) l Active Myocarditis : • Cellular infiltrate +, myocyte necrosis + l Borderline Myocarditis : • Cellular infiltrate +, myocyte necrosis l Negative Biopsy : • Cellular infiltrate -, myocyte necrosis Distribution and diffusion of the cellular infiltrate l l ¢ Focal, confluent or diffuse Mild, moderate, severe However, low to moderate sensitivity/specificity

Histology: Dallas Criteria Borderline Active
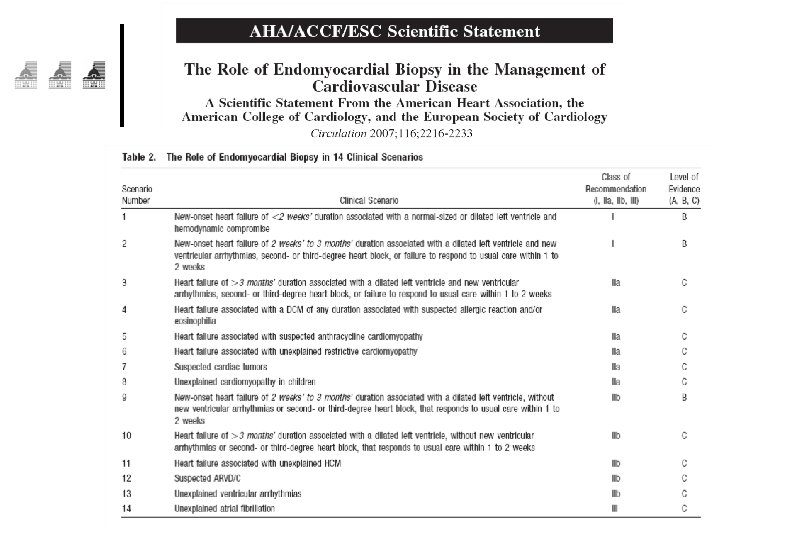

Grade 1, Level B: .

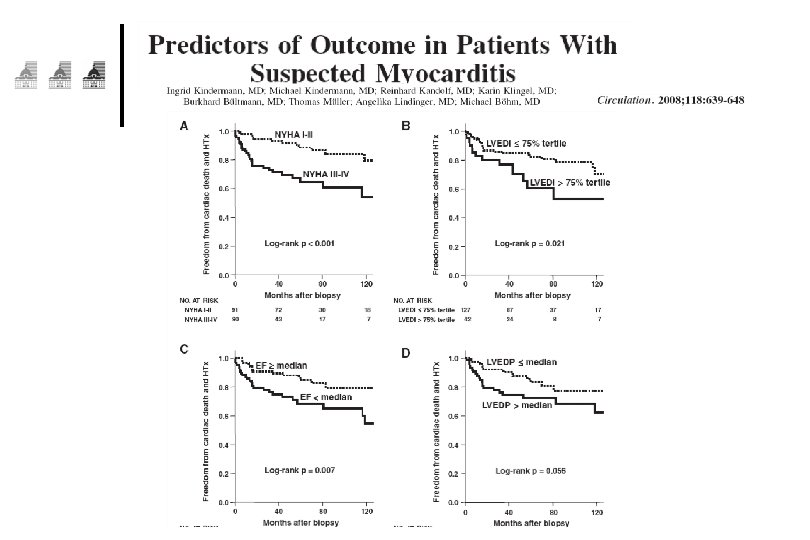
Prognosis
 P=0. 05 (132 patients)")
Prognosis Mc. Carthy, NEJM, 2000 Survie sans transplantation (15 patients) P=0. 05 (132 patients)

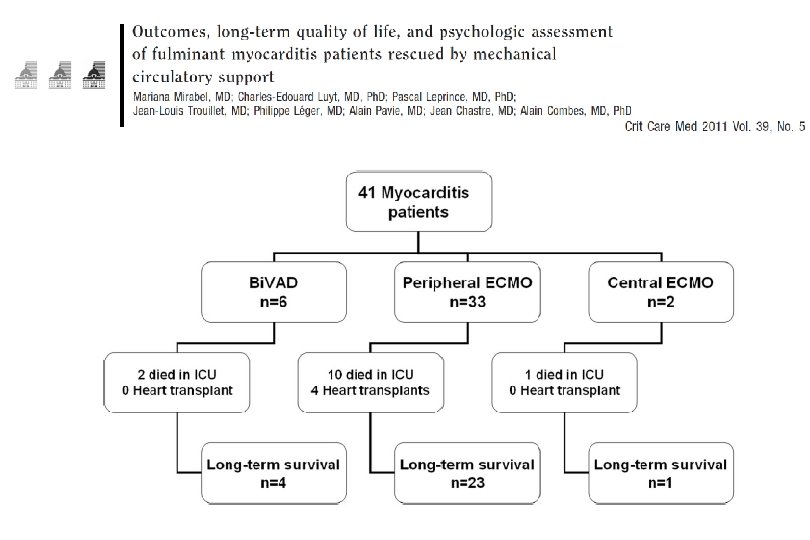
2003 - 2009 ¢ 41 patients refractory cardiogenic shock due to fulminant myocarditis ¢ Mean age 38± 12 years l 66%, women l ¢ Mechanical assistance Thoratec Bi. VAD (n=6) or l ECMO (n=35) l
 patients had heart transplantation Independent predictors of ICU")
Long term survival: 68% 4 (10%) patients had heart transplantation Independent predictors of ICU death determined at admission: SAPS II >56 (OR, 10. 23) and troponin Ic >12 microg/L (OR, 7. 49)
![¢ Complete follow-up for 26 survivors ¢ Median follow-up was 525 [92– 2400] days](http://slidetodoc.com/presentation_image/652a90f8bbe6a1731ca1c534ceb4f6e5/image-31.jpg "¢ Complete follow-up for 26 survivors ¢ Median follow-up was 525 [92– 2400] days")
¢ Complete follow-up for 26 survivors ¢ Median follow-up was 525 [92– 2400] days ¢ Mean LVEF was 57± 9% ¢ l ≥ 60% for 12 non-transplant and all 4 transplanted l 40– 60% for 10 nontransplanted survivors 21 patients had percutaneous femoral ECMO l 10 still complained of paresthesia/peripheral neurological defect l 2 had persistent leg ischemia requiring surgical repair for 1 and amputation for the other

Treatment

Treatment ¢ Supportive care always indicated l l l ¢ Bed rest Diuretics, vasodilators ACE inhibitors, angiotensin-receptor blockers Aldosterone antagonists b-blockers, (with caution in the acute phase) Vasopressors/inotropic agents in case of shock Mechanical assistance +++ l l May be urgently needed if fulminant form or rapid deterioration of hemodynamic status Patients should rapidly be transferred to experienced centers Bridge to recovery: • ECMO+++, First line assistance (Heart transplantation)

ECMO vs. Bi. VAD for fulminant myocarditis?

P = ns

T bilirubin mol/dl Creatinine mol/dl
 patients had heart transplantation Independent predictors of ICU")
Long term survival: 68%, 4 (10%) patients had heart transplantation Independent predictors of ICU death determined at admission: SAPS II >56 (OR, 10. 23) and troponin Ic >12 g/L (OR, 7. 49)

Specific/Novel treatments ¢ Immunosuppression l First line therapy if • Giant cell • Systemic autoimmune diseases l l l ¢ Immunomodulation/Stimulation l l ¢ Corticosteroids Cyclosporine, Tacrolimus Azathioprine IV Immune globulins Interferon Antiviral agents, vaccination

Myocarditis Treatment Trial ¢ ¢ 111 randomized patients, LVEF<45% Histologically proven myocarditis Immunosuppression protocol Placebo vs prednisone + Cyclosporine or azathioprine Mason, NEJM, 1995

IV immune globulin Mc. Namara, Circ, 2001 ¢ ¢ ¢ 62 patients with DCM, randomized, LVEF<40% Placebo vs IVIg P = NS

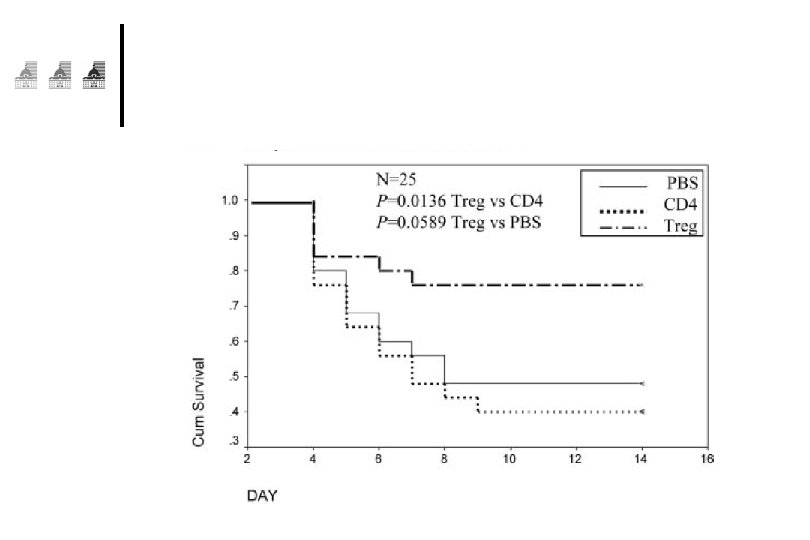
Tailored immune-modulating strategies Liu, Circ, 2001 Phase III

Immunomodulation vs Immunosuppression ¢ Interféron b chez les patients avec persistance virale entero-adénovirus l l l ¢ Kuhl, Circ, 2003 22 patients, Dysfonction VG, génome viral + Interféron: Clearance virus, amélioration FE Immunosuppression: prednisone+imurel l Frustaci, Circ, 03 • 41 patients, myocardite active, Dysfonction VG • 21 répondeurs, 20 non rep • Répondeurs: Auto. AC +, génome viral- (sauf Hep C) l Wojnicz, Circ 01 • 84 patients CMD, HLA surexprimé sur myocytes • Traitement de 3 mois • Amélioration dans groupe traité: 71% vs 31%


Conclusion ¢ ¢ ¢ Myocarditis is a rare and severe condition l Especially the fulminant form Diagnosis based on clinical features, EKG, Echo, Troponin, MRI l Myocarditis can mimic acute coronary syndromes Mechanical circulatory assistance may be urgently needed if rapid hemodynamic deterioration Immunosuppression during the acute phase l Giant cell l Systemic autoimmune diseases Significant progresses in the understanding of the pathophysiology of the disease in recent years l Help design tailored immune-modulating strategies

La Pitié: Louis XIV, 1656… To 2012… La Chapelle Institut de Cardiologie
- Slides: 57