SEVERE ASTHMA BY ARSHAD EJAZI INTRODUCTION Asthma is

SEVERE ASTHMA BY ARSHAD EJAZI

INTRODUCTION Asthma is a chronic inflammatory disorder of the airway associated with reversible airway hyperesponsiveness that leads to recurrent episodes of wheezing , breathlessness , chest tightness and coughing, particularly at night or in the early morning.

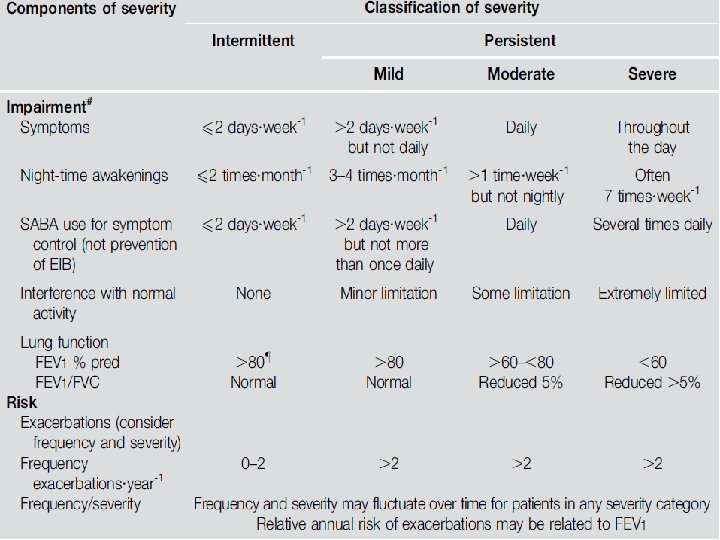
CATEGORIES : 1. INTERMITTENT ASTHMA 2. MILD PERSISTANT ASTHMA 3. MODERATE PERSISTANT ASTHMA 4. SEVERE ASTHMA Third Expert Panel Report(ERP-3) Classification

SEVERE ASTHMA

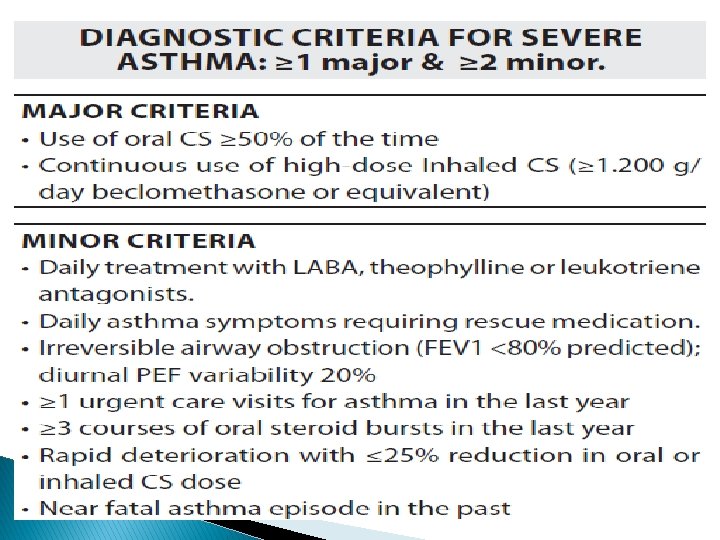
Ø Those patients who require oral corticosteroids to remain under control and those with ongoing asthma symptoms despite maintainence therapy of moderate asthma(ie high dose of ICS combined with LABA), should be regarded as severe asthma. Ø 10% of asthma population represent severe asthmatics

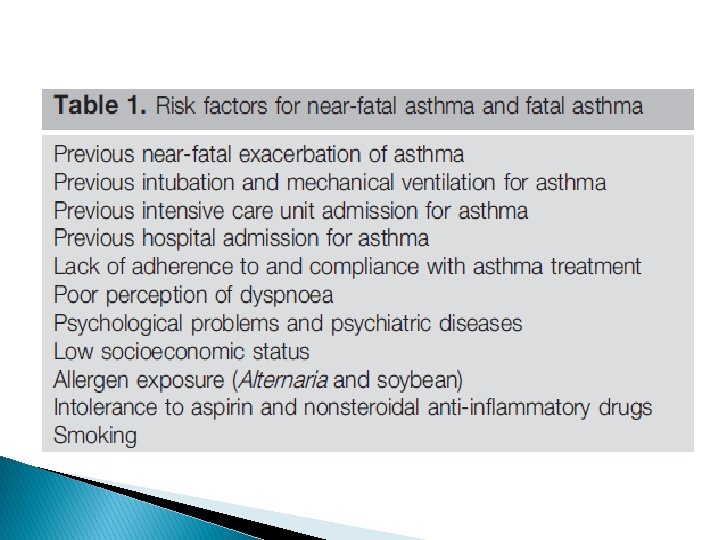
FATAL & NEAR FATAL ASTHMA q FATAL ASTHMA � A severe asthma exacerbation resulting in death. q NEAR � Is FATAL ASTHMA associated with hypercapnea, respiratory acidosis and respiratory arrest requiring intubation & mechanical ventilation.

PATHOGENESIS

Allergens Acquired Immunity Particulates, Pollutants, Virus, Endotoxin, Bacteria Ig. E Activated TH 2 Cells ICS TLR Macrophages and Epithelial Cells X Eosinophilic Asthma Innate Immunity X LABA Neutrophilic Asthma Inflammatory cell activation X LABA hyperresponsiveness

AIRWAY INFLAMMATION Ø Decrease production of protective mediators including PGE 2 &15 HETE acid. Ø Defective apoptotic inflammatory cell because of increase BCL 2 in asthma. Ø Severity of distal lung inflammation may be equally or even more important that of proximal.
 to the small airway")
Ø Increased inflammatory cell recruitment (mainly chymase +ve mast cell) to the small airway compared to medium or large airway.

FIXED AIRWAY OBSTRUCTION q INTRODUCTION � A considerable proportion of asthmatic have persistent & progressive airflow limitation over time depite aggressive T/t with LABA, high dose ICS, oral GC � Post bronchodilator FEV 1/FVC below the lower limit of normal in a patient of asthma taking high dose of ICS during a stable phase of disease for at least 4 wk q PATHOLOGY � Increase airway smooth musle mass, subepithelial thickening, increase extracellular matrix component.

RISK FACTORS Ø Childhood respiratory disease Ø Smoking Ø Female sex Ø Adult onset nonatopic & respiratory inflammation Ø Fungal infection Ø Clinical Significance Ø Poor prognosis Ø Frequent unpredictable serious asthmatic attack Ø Permanent exercise limitation

INFLAMMATORY CELLS 1. EOSINOPHIL Ø Increased level associated with disease severity, airway obstruction & hyperreactivity Ø Increased reticular basement membrane thickening Ø Increased TGF-β expression Ø Counts on BAL & sputum are more sensitive than biopsy

2. NEUTROPHIL Ø Neutrophilic mediators like LT B 4 , IL 8 , inflammatory protein 1 a & TNF A are increased. Ø Neutrophilia is associated with absence of atopy, worse asthma control, more symptomatic, lower lung function Ø EGFR is increased and its expression in bronchial epithelium correlated with IL 8.

3. LYMPHOCYTES & CYTOKINES � Predominantly � Increased CD 4+ T cells bearing IL-2 R q IL-17 Neutrophilic recruitment IL-13 correlate with Eosinophilia q IL-5 q TGF-β 1 Mediate severity through q critical cytokine in regulating the function & recruitment of Eosinophil remodelling

ALLERGIC AND NONALLERGIC FACTOR

GENES AND SEVERE ASTHMA Pathogenesis of asthma

GWAS OF SEVERE ASTHMA q. Genome q GENE Ø Ø Ø wide association study ASSOCIATED WITH SEVERE ASTHMA ADAM 33 HHIP/rs varint on chromosome 4 q 31 IL-4 R ADRB 2 CYSLTR 2 ALOX 5

GENES RELATED TO ASTHMA SEVERITY q ADAM 33 gene located on chr 20 p 13 � Asthma susceptiblity & severity gene � Predictor of increased decline in FEV 1 q IL 4 receptor gene PHARMACOGENETICS Ø ADRB 2 responsible for variablity to bronchodilator response(ie decrease response to SABA than LABA)

PHENOTYPES 1. ALLERGIC SEVERE ASTHMA 2. LATE ONSET HYPEREOSINOPHILIC ASTHMA 3. LATER ONSET SYMPTOM PRONE SEVERE ASTHMA

1. ALLERGIC SEVERE ASTHMA � Incidence � Develop � High 40 -50% disease in childhood number of allergic skin test Ig. E level, greater Environmental exposure , family H/O asthma � T-helper � Both cell (Th) type 2 immune response eosinophilic & neutrophilic inflammation associated

2. LATE ONSET HYPEREOSINOPHILIC Ø 25% of patient have persistent large airway tissue eosinophilia , despite continued treatment with high dose systemic & ICS. Ø They are healthy until late 20 s Ø Preceeding Ø Both factors are URTI, LRTI, Sinusitis blood & lung eosinophil are increased Ø Increased Proeosinophilic/Th 2 cytokine IL-5

� High level of TGF B 2 & a thicker subepithelial basement membrane. � Increased in numbers of CD 3, CD 4 & CD 8 Tcells � More exacerbation & near fatal events

ASPIRIN INDUCED ASTHMA � TRIAD-chronic rhinosinusitis , moderate to severe asthma & nasal polyposis. � Peak age of onset B/W 29 & 34 � Previous exposure to aspirin is not a risk factor for its development. � But once established , ingestion of aspirin or other NSAIDS induces an acute worsening of asthma & rhinosinusitis. � Responds poorly to steroids.

3. LATER ONSET SYMPTOM PRONE � Primarily in female, with onset of disease in 5 th decade � In obese with natural or surgical menopause � Less airway obstruction � Lesser duration of disease � Paucity of inflammation � Very little is known about the pathogenesis

Clinical phenotypes of asthma P. Haldar et al AJRCCM, 2008

NEW APPROACH TO PHENOTYPING OF ASTHMA-CLUSTER ANALYSIS Ø Early onset severe asthma – symptom predominant. Ø Late onset severe asthma – inflammation predominant.

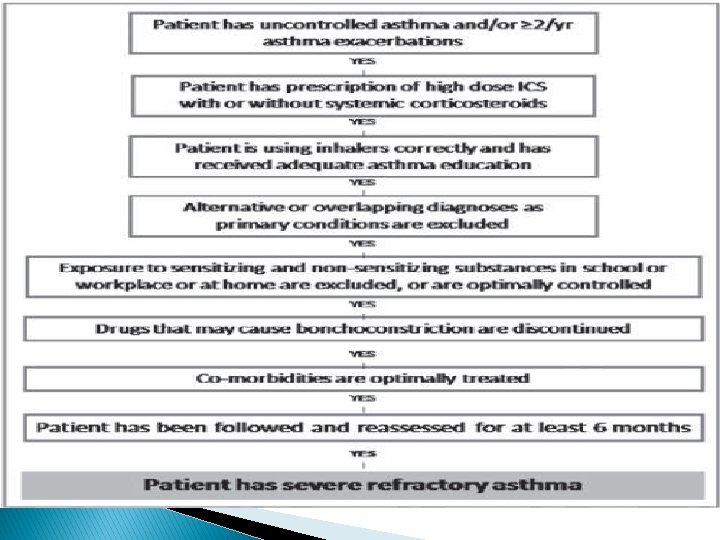
EVALUATION � Patient should be evaluated within the first 6 months.

IS ASTHMA CORRECT DIAGNOSIS �A significant proportion of severe asthma patient may not have asthma. � To confirm correct diagnosis at initial evaluation

ALTERNATIVE DIAGNOSIS

CHECK FOR COMORBIDITIES q RHINOSINUSITIS � 51 -95% of difficult to treat asthmatics are found to have upper airway disease. � Severity of rhinosinusitis appear to correlate with asthma severity. q GASTRO-OESOPHAGEAL REFLUX � The presence of symptoms of GERD should be evaluated.

q. VOCAL CORD DYSFUNCTION � It consist of paradoxical adduction of vocal cords during inspiration. � Diagnosis is difficult to determine. � Variable flattening of inspiratory loop on spirometry. � Indirect Laryngoscopy required for correct diagnosis. q OBSTRUCTIVE SLEEP APNEA � � � High prevalance in patients with severe asthma(50%-96%). Contributing to poor asthma control. Mainly in patient with nocturnal symptoms.

ALLERGIC BRONCHOPULMONARY ASPERGILLOSIS � Occurs most commonly in patient with asthma & atopy � Prevalance � Asthma of ABPA in asthma is 12. 9%. is one of the major diagnostic criteria of ABPA. q PSYCHIATRIC � Anxiety DISORDERS & depression

ASSESS ADHERENCE TO TREATMENT � Confirm � Rule about appropriate inhaler technique. out psyshological dysfunction associated like depression. � Ask about side effects of drug.

MEDICAL HISTORY TO BE ASKED
 � EXHALED")
DIAGNOSTIC TESTS � PULMONARY FUNCTION TEST � IMAGING (CHEST RADIOGRAPH & HRCT) � EXHALED NITRIC OXIDE (ENO) � SERUM Ig. E & PERIPHERAL BLOOD EOSINOPHIL. � ALLERGY SKIN TEST Ø VOLUME DIFFUSING CAPACITY. Ø AIRWAY CHALLENGE TEST. Ø BLOOD GAS ANALYSIS. Ø BAL.

A PRACTICAL APPROACH TO SEVERE ASTHMA

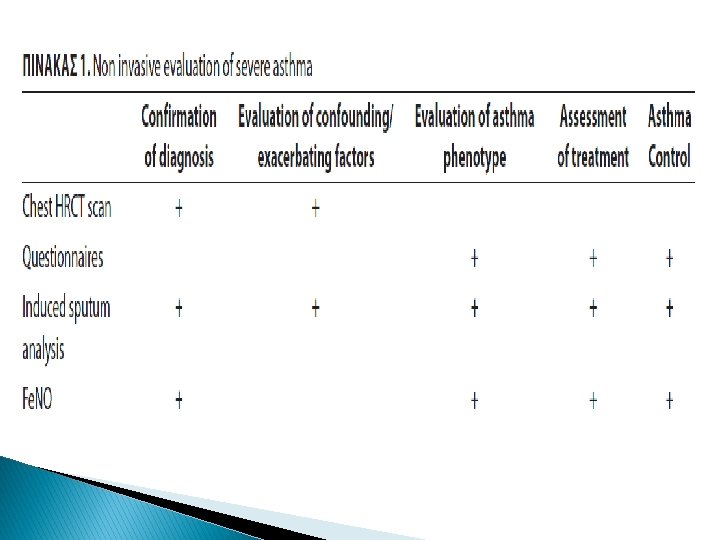
NON INVASIVE ASSESSMENT OF SEVERE ASTHMA � Technique of assessment
 The evidence Supporting the concept of FENO in")
FRACTION OF EXHALED NITRIC OXIDE (FENO) The evidence Supporting the concept of FENO in diagnosis & management of asthma include. A. Increase FENO in patient with asthma is highly correlated with eosinophilic airway inflam. B. The use of ICS results in a fall in FENO, in a dose response relationship. Measurement of FENO is highly reproducible, well tolerated safe, relatively quick & simple to perform.

INDUCED SPUTUM PROCEDURE EUROPEAN RESPIRATORY SOCIETY rec- 8 MINUTES

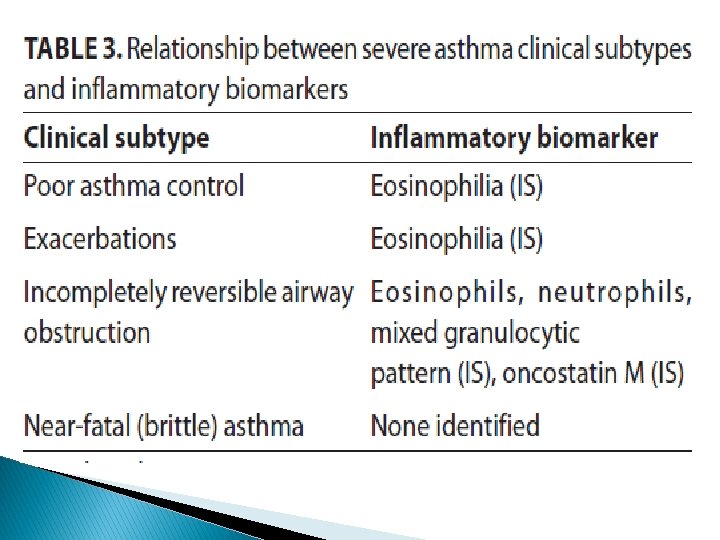
� Sputum processing provides a differential cell count. � Phenotypes on the basis of sputum cell count. 1. 2. Ø Ø Eosinophilic Neutrophilic Contra indication Low FEV 1 is a relative C/I Benefit of sputum eosinophil directed management are more clearly seen. Ø Sputum eosinophilia is associated with a clinically favourable short term response to ICS.
 Ø In severe asthma acidification of exhaled breath can be")
EXHALED BREATH CONDENSATE (EBC) Ø In severe asthma acidification of exhaled breath can be detected by a low EBC p. H. Ø The levels of other markers like RANTES and endothelin-1 are reported to be elevated in the EBC of pt. with severe asthma and poor control. ELECRONIC NOSE(e-NOSE) Ø The pattern of exhaled Volatile organic Compounds can be assessed using the e-nose.

HIGH RESOLUTION COMPUTED TOMOGRAPHY � To differentiate condition that can masquerade asthma like panacinar emphysema, ABPA, broncholitis obliterans. � No definitive criteria that confirm the use of HRCT in evaluation of Severe asthma. � It can be used in order to correlate severe asthma and airway thickening in the research setting.

QUESTIONNAIRES Ø GINA suggested the use of validated instrument for assessing the clinical control of asthma in a reproducible manner. Validated asthma control instruments(ASI) include are: 1. Asthma control test(ACT). Ø 2. Asthma control questionnaire(ACQ). 3. Asthma therapy assessment questionnaire(ATAQ).

MANAGEMENET OF SEVERE ASTHMA

GINA 2006: Asthma treatment steps as needed rapidacting β 2 -agonist Oral glucocorticosteroid (lowest dose) *in children <6 yrs: moderate-dose ICS anti-Ig. E antibodies

SEVERE ASTHMA TREATMENT Ø Step 4 & 5 management approach of GINA guideline i, e, . High dose of ICS & inhaled LABA , along with additional medication, such as oral steroids, leukotriene-antagonists and theophylline.
 Long-acting B 2 -agonistis(LABA) Ø")
CURRENT TREATMENT IN SEVERE ASTHMA Ø Inhaled corticosteroid (ICS) Long-acting B 2 -agonistis(LABA) Ø Combination therapy(ICS+LABA) Ø Anti-leukotrienes(LTRAs) Ø Theophylline Ø Ø Anti-Ig. E monoclonal antibody(omalizumab) Ø Macrolides Long-acting anticholinergics Ø immunosuppressives Ø
 Ø High dose ICS(>1200µg/day of beclomethasone) constitute the basis of T/t. Ø")
INHALED CORTICOSTEROIDS(ICS) Ø High dose ICS(>1200µg/day of beclomethasone) constitute the basis of T/t. Ø Optimal starting & maintenance of ICS for severe asthma are not clearly documented. Ø Ciclesonide a newer ICS compound significantly reduced the need for oral steroid.
 Ø Improve lung function. Ø Asthma control days. Ø Asthma related")
COMBINATION THERAPY (ICS+LABA) Ø Improve lung function. Ø Asthma control days. Ø Asthma related quality of life. Ø Reduces the risk of hospitalisation & ER visits. ANTI-LEUKOTRIENES Ø As add on therapy for of T/t of severe asthma. Ø It may lead to clinical benefit in aspirin intolerant asthma.
 Ø")
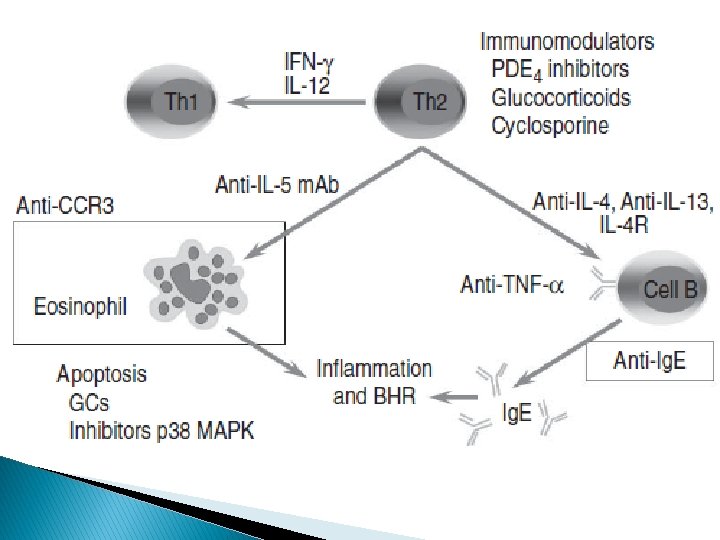
OMALIZUMAB Ø Glycosylated Ig. G Mab binds to Ig. E receptor(Fce. R I) Ø Approved by FDA in severe persistent allergic asthma Ø Add on therapy in ≥ 12 years patient & having a positive skin test Ø Decreased number of exacerbation& ER visit, improve lung function & quality of life Ø Administered through sc route Ø ADR- Anaphylaxis, chrug strauss syndrome
 � Anti-IL-4")
FUTURE FORMS OF TREATMENT � Anti-TNF-α monoclonal antibody � Anti-CD 25 (Daclizumab) � Anti-IL-4 � Anti-IL-5 � Anti-IL monoclonal antibody (Mepolizumab) 9 � Anti-IL 13 � Phosphodiesterase (PDE)Inhibitors(roflumilast) � Bronchial thermoplasty

BRONCHIAL THERMOPLASTY Ø Half of patient with severe asthma do not have their symptoms controlled despite compliance with medication. Ø Increased airway smooth muscle mass has been found on autopsy in patient with fatal or severe asthma. Ø Improve QOL, asthma symptom & reduce exacerbations requiring corticosteroid

Approach in Severe asthma

THANK YOU
- Slides: 62