SESSION 2018 2019 PROGRAM NAME B SC NUTRITION

SESSION : 2018 2019 PROGRAM NAME : B. SC. NUTRITION HONOURS COURSE NAME : BASIC DIETETICS SEMESTER - III

PAPER – C 7 T TOPIC : MODIFICATION IN FEEDING TECHNIQUES

parenteral Feeding Nutrition Concept & Definition: Nutrient preparation directly into vein PN Sterile, nutrient dense solution Infused intravenously Peripheral Venous Access / Central Venous Access Digestive tract Nourish those patients who are digesting & absorbing nutrients not capable of

parenteral Feeding Nutrition Indications: can not eat due to cancer of the pharynx, oesophagus will not eat due to some physiological & other problems should not eat due to surgery of the GI tract, inflammatory bowel diseases can not eat enough due to persistent nausea & anorexia can not be fed adequately by tube feeding hypermetabolic states like burns , severe infections etc.

parenteral Feeding Nutrition Duration: Maximum 48 to 72 hours. Objectives: To provide water & electrolytes q To correct electrolyte imbalance q To make up for the loss of tissue proteins q To provide energy to meet the daily needs of the patient q
 §")
parenteral Feeding Nutrition Venous Access for PN Support: Ø Peripheral Parenteral Nutrition (PPN) § Peripheral veins § Low concentration of solutions § Short duration (less than 10 days) § Does not meet all the nutritional needs of the patient § Short – term nutrition support
 § Central veins § Higher concentration")
parenteral Feeding Nutrition Ø Total Parenteral Nutrition (TPN) § Central veins § Higher concentration solutions § Long duration § Reliably meet a person’s complete nutrient requirements § Long – term nutrition support

parenteral Feeding Nutrition Chemical composition of Parenteral Feed: v Carbohydrates • • • Mainly glucose, fructose, sorbitol & other carbohydrate derivatives Glucose 5% of solutions Higher concentration of glucose Thrombophlebitis Fructose 10 – 15% of solutions Minimum of 100 gm of glucose / day To prevent protein catabolism

parenteral Feeding Nutrition v Amino • • • Acids Protein hydrolysates & synthetic amino acid mixtures L amino acids Commercial amino acids are available in concentrations 3. 5, 5. 5, 7. 5, 8. 5, 10, 11 &15% v Fats • • • Emulsified fats Provide essential fatty acids & calories If toxic results are observed then fats have to be avoided

parenteral Feeding Nutrition v Vitamins • Especially vitamin B 12, folic acid & vitamin K v Electrolytes • • Sodium, potassium, chlorine, phosphorous, calcium & magnesium Trace elements : zinc, copper, chromium, manganese & iodine v Water • • Daily minimum requirement 1. 5 liter If any water losses then these should be made up

parenteral Feeding Nutrition Nutrient Contribution: ü ü 30 – 50% of the daily nutrients Remaining should be given by oral route Advantages: o o o Started easily Simple No delay in calorie intake Does not rely on gastric or intestinal function Less need for interruptions Safe

parenteral Feeding Nutrition Disadvantages / Complications � Catheter related complications o Arrhythmias o Pneumothorax o Thrombosis o Sepsis o Puncture of the subclavian artery � Infections o Septicaemia

parenteral Feeding Nutrition � Metabolic o o complications Hypoglycemia Azotemia Electrolyte disturbances Acid base balance disturbances � Nutritional o o o complications Rapid weight loss Vitamin deficiency Vitamin toxicity Trace element deficiency Essential fatty acid deficiency

parenteral Feeding Nutrition � Liver o o o complications Rise in SGOT Rise in alkaline phosphatase Fatty changes in the liver

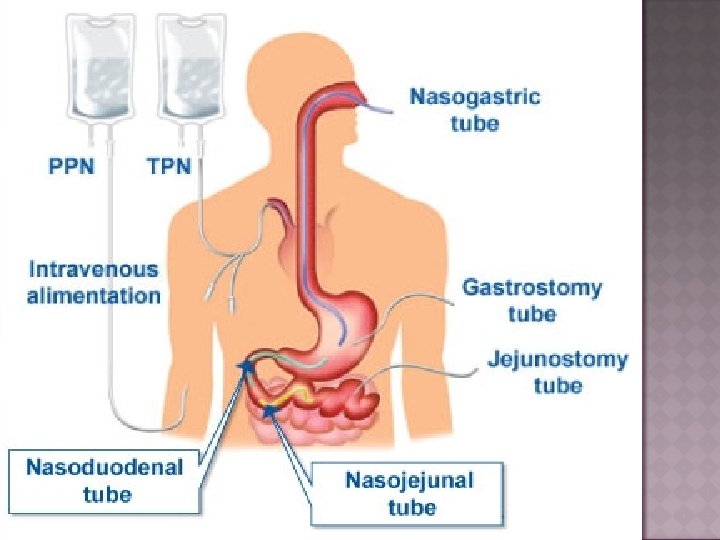
TUBE FEEDING v Concept & Definition: TUBE NOSE Stomach Duodenum Jejunum

TUBE FEEDING q Nasogastric Feeding q Nasoduodenal Feeding q Nasojejunal Feeding These are short term feeding techniques (3 to 4 weeks)

TUBE FEEDING TUBE Surgical Procedure Gastrostomy Jejunostomy These are long term feeding techniques.

TUBE FEEDING v Characteristics § § § of Satisfactory Tube feeding Nutritionally adequate Well tolerated by patients Easily digested Easily prepared Inexpensive

TUBE FEEDING v Indications Those can’t swallow Ø Those who have persistent anorexia Ø Those who are semiconscious or unconscious Ø Those who have to be given unpalatable formula Ø Severely undernourished patients Ø Those who can’t digest & absorb foods Ø Post operative cases Ø

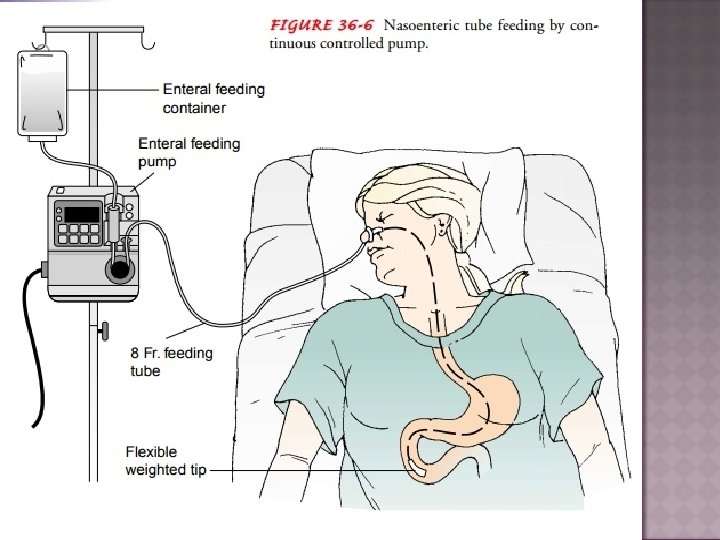
TUBE FEEDING v Apparatus • Tube used in this process – Ryles Tube • Soft, flexible tube • Thin, soft, polythene tube of 2 to 3 mm in diameter • Lubrication purpose – olive oil & liquid paraffin

TUBE FEEDING v Composition of Tube feeding 3 types depending on its composition: Natural liquid foods § Glucose water, fruit juices, coconut water, whole or skim milk, strained soups of cooked vegetables, cereals, sugar solution, molasses etc. § Vegetable oil or cream & non fat dry milk are also incorporated.

TUBE FEEDING Blenderized Feeding ü Ordinary food items which can’t be swallowed should be blenderized & use for tube feeding. ü Foods can be precooked. ü Well tolerated, less commercial formula. expensive than a
 Rice Green gram dal Bread Milk Skim milk powder")
TUBE FEEDING Ingredients (cooked /raw) Rice Green gram dal Bread Milk Skim milk powder Pumpkin Spinach Amount (gm) 75 40 20 200 ml 60 50 50
 Carrots Banana Sugar Refined oil Butter Water Amount (gm)")
TUBE FEEDING Ingredients (cooked /raw) Carrots Banana Sugar Refined oil Butter Water Amount (gm) 50 70 60 20 ml 7 1500 ml

TUBE FEEDING Elemental Diet Normal foods may be replaced by preparation of protein or amino acid, fat & carbohydrate in easily assimilable forms § Commercially supplied polymeric mixtures can also be used. § The commercial preparation possess both advantages & disadvantage. Advantages: Ø Convenience Ø Constant composition Ø Presterilization Ø Minimal preparation time Ø Ease of administration §

TUBE FEEDING Disadvantages: • High cost • Unpleasant taste • Sometime high osmolarity v Contribution of Nutrients Energy: § An average adult patient will require 1500 to 2000 kcal § After surgery, injury, burns or in severe PEM about 3000 kcals should be provided § Inadequate calories can lead to wasting of muscles of the body

TUBE FEEDING Protein § Usually patients are given about 60 - 70 gms of protein except in case of hepatic coma, kidney failure etc. § If there is injury, surgery, burns or severe PEM about 100 to 200 gms of protein are needed. Fat § Fats may be given in the form of emulsion.

TUBE FEEDING Carbohydrate § Glucose, cane sugar, dextrin, maltose may be given to the patients § About 300 – 500 gms of carbohydrate may be given depending on the calorie needs. Fluid § About 2500 – 3000 ml. should be given daily to meet the normal requirements & to compensate for the fluid losses

TUBE FEEDING Electrolytes § Na. Cl, KCl & other such important electrolytes can be given according to the needs. Vitamins § All the essential vitamins may be supplied to the patients through tube feeding

TUBE FEEDING v Advantages q The gastric content can be analyzed. q Unpalatable drugs & formulas can be given. q Usually there are no risk of infections like in case of parenteral feeding. q A lot of fluid can be administered. q It can be continued for a long duration of time. q It is economical. q Adequate nutrition can be easily given by this method.

TUBE FEEDING v Disadvantage GI complications • Vomiting • Diarrhoea • Constipation • Abdominal pain • Gastric irritation Mechanical complications • Tube fractures • Leakage • Obstruction • Irritation

TUBE FEEDING Metabolic complications • Hypovolemia • Hyperkalemia • Hypophosphatemia • Hypertonic dehydration • Fluid overload
- Slides: 34