Sepsisen oppdatering og bakgrunn for tiltakspakken Pasientsikkerhetsprogrammet 8

Sepsis-en oppdatering og bakgrunn for tiltakspakken! Pasientsikkerhetsprogrammet 8 mars 2017 Hans Flaatten KSK/Intensiv Bergen

Hvorfor?

Sepsis: et komplisert forløp Initial håndtering • Diagnostikk • Start behandling: Respirasjons og sirkulasjonssvikt Kildekontroll • Antibiotika • Fjerne fokus Intensivbehandling • Organsvikt Rehabilitering

Tidligere definisjoner Sitert i 7427 andre artikler! Chest 1992 MODS & SIRS

SIRS kriteriene ?

Dårlig presisjon N Engl J Med 2015; 372: 1629 -38

JAMA 23 februar 2016
 • Etter ferdig arbeide")
Prosess • Arbeidsgruppe etablert av ESICM og SCCM (17 personer) • Etter ferdig arbeide har forslaget vært på “høring” i en rekke foreninger som har gitt støtte til definisjonene: • Academy of Medical Royal Colleges (UK); American Association of Critical Care Nurses; American Thoracic Society (endorsed August 25, 2015); Australian–New Zealand Intensive Care Society (ANZICS); Asia Pacific Association of Critical Care Medicine; Brasilian Society of Critical Care; Central American and Caribbean Intensive Therapy Consortium; Chinese Society of Critical Care Medicine–China Medical Association; Critical Care Society of South Africa; Emirates Intensive Care Society; European Respiratory Society; European Resuscitation Council; European Society of Clinical Microbiology and Infectious Diseases and its Study Group of Bloodstream Infections and Sepsis; European Society of Emergency Medicine; European Society of Intensive Care Medicine; European Society of Paediatric and Neonatal Intensive Care; German Sepsis Society; Indian Society of Critical Care Medicine; International Pan Arabian Critical Care Medicine Society; Japanese Association for Acute Medicine; Japanese Society of Intensive Care Medicine; Pan American/Pan Iberian Congress of Intensive Care; Red Intensiva (Sociedad Chilena de Medicina Cri tica y Urgencias); Sociedad Peruana de Medicina Critica; Shock Society; Sociedad Argentina de Terapia Intensiva; Society of Critical Care Medicine; Surgical Infection Society; World Federation of Pediatric Intensive and Critical Care Societies; World Federation of Critical Care Nurses; World Federation of Societies of Intensive and Critical Care Medicine.

Hvordan skal vi forstå sepsis? • Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated host response to infection. • Sepsis is a syndrome shaped by pathogen factors and host factors (eg, sex, race and other genetic determinants, age, comorbidities, environment) with characteristics that evolve over time. • What differentiates sepsis from infection is an aberrant or dysregulated host response and the presence of organ dysfunction.

Organdysfunksjon ved sepsis • Sepsis-induced organ dysfunction may be occult; therefore, its presence should be considered in any patient presenting with infection. • Conversely, unrecognized infection may be the cause of new-onset organ dysfunction. Any unexplained organ dysfunction should thus raise the possibility of underlying infection.

Den nye terminologien Sepsis Septisk sjokk Infeksjon Sepsis inkluderer nå varierende grader av organdysfunksjon, og alvorlig sepsis forsvinner derfor som begrep

Kliniske kriterier: Sepsis hos kritiske syke • Bruk av SOFA skår • Organ dysfunction can be identified as an acute change in total SOFA score ≥ 2 points consequent to the infection. • A SOFA score = 2 reflects an overall mortality risk of approximately 10% in a general hospital population with suspected infection
 • Patients with")
Kliniske kriterier: pasienter med akutte infeksjoner • q. SOFA (quick SOFA) • Patients with suspected infection who are likely to have a prolonged ICU stay or to die in the hospital can be promptly identified at the bedside with q. SOFA, ie, • alteration in mental status • systolic blood pressure ≤ 100 mm Hg, • or respiratory rate ≥ 22/min.

Kliniske kriterier: Septisk sjokk • Septic shock is a subset of sepsis in which underlying circulatory and cellular/metabolic abnormalities are profound enough to substantially increase mortality. • Patients with septic shock can be identified with a clinical construct of sepsis with • persisting hypotension requiring vasopressors to maintain MAP 65 mm Hg AND • having a serum lactate level >2 mmol/L (18 mg/d. L) despite adequate volume resuscitation. • With these criteria, hospital mortality is in excess of 40%.

Pasientsikkerhetsprogrammet 2017

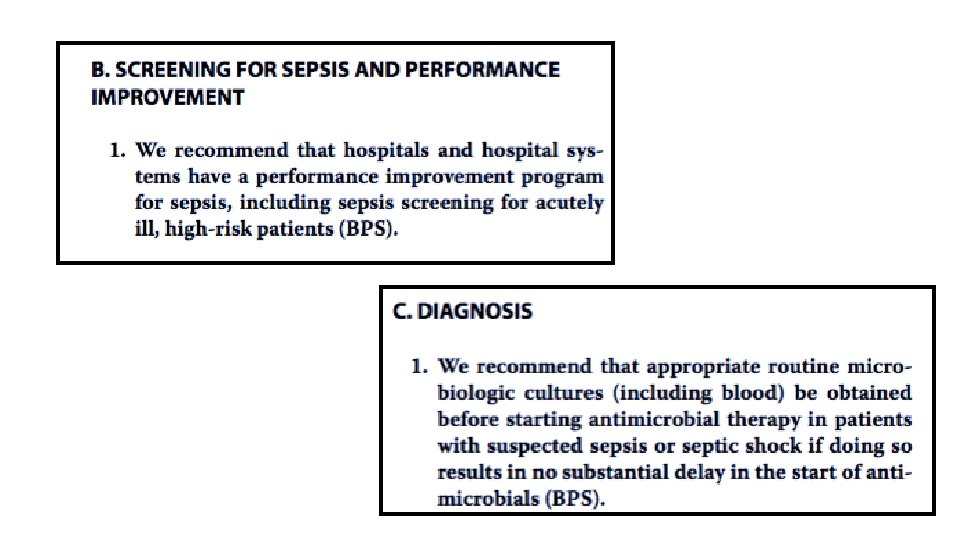
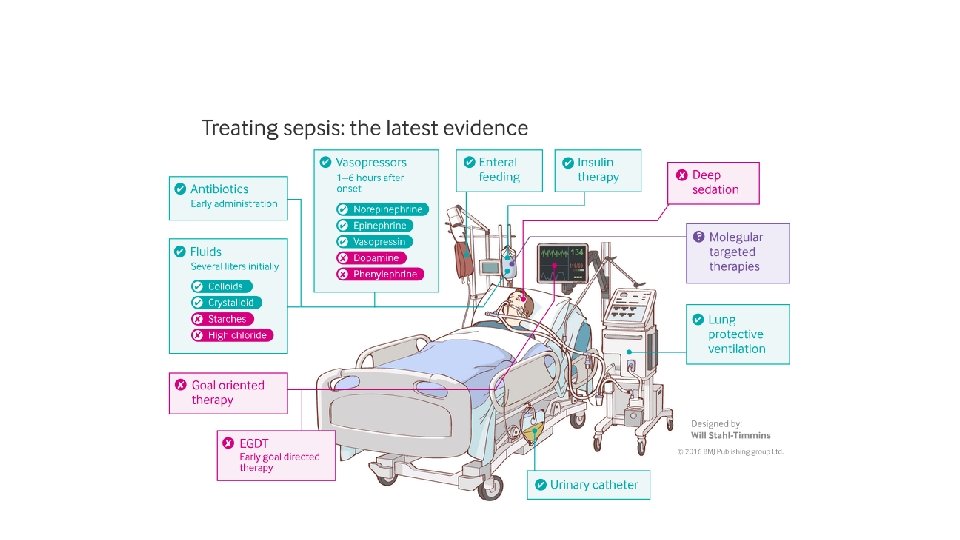
Tiltakene

ABCDE • Sikre vitale funksjoner: • Respirasjon • Sirkulasjon • Bevissthet Mål: MAP ≥ 65 mm. Hg

Tiltakene

SOFA skår Grad Sirkulasjon* Respirasjon# Nyrefunksjon CNS Koagulasjon Lever MAP og bruk av vasopressor MAP ≥ 70 MAP < 70 Pa. O 2/Fi. O 2 ratio (k. Pa) >53 39, 9 -53 Kreatinin/DU μmol/l & ml <110 110 -170 GCS 15 13 -14 TPK x 103/μl > 150 < 150 Bilirubin μmol/l <20 20 -32 DA ≤ 5; Dobutamin DA > 5; NA/A ≤ 0, 1 NA/A > 0, 1 26, 6 – 39, 8 171 -299 10 -12 < 100 33 -101 13, 3 – 26, 5 300 -440 < 500 ml/24 t >440 < 200 ml/24 t 6 -9 < 50 102 -204 <6 < 20 >204 0 1 2 3 4 < 13, 3 *alle doser gitt i µg/kg/min, DA= Dopamin, NA=Noradrenalin, A=Adrenalin # 3 eller 4 poeng bare for pasienter på respirator (NIV+IPPV)

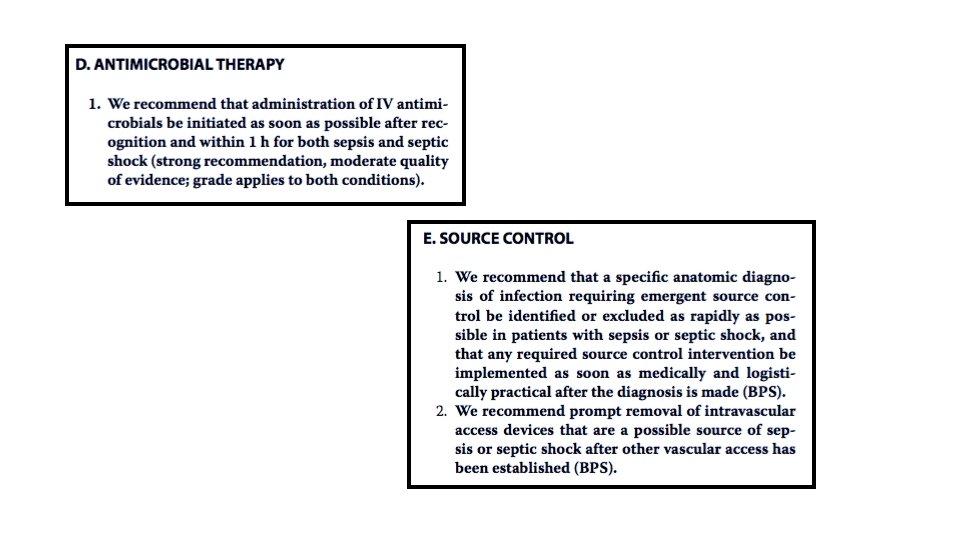
Tiltakene
: 301 -308.")
JAMA. 2017; 317(3): 301 -308.

From: Prognostic Accuracy of Sepsis-3 Criteria for In-Hospital Mortality Among Patients With Suspected Infection Presenting to the Emergency Department JAMA. 2017; 317(3): 301 -308. doi: 10. 1001/jama. 2016. 20329 Figure Legend: Flow Diagram of Study to Validate q. SOFA Scoringq. SOFA indicates quick Sequential Organ Failure Assessment. Date of download: 2/2/2017 Copyright © 2017 American Medical Association. All rights reserved.

From: Prognostic Accuracy of Sepsis-3 Criteria for In-Hospital Mortality Among Patients With Suspected Infection Presenting to the Emergency Department JAMA. 2017; 317(3): 301 -308. doi: 10. 1001/jama. 2016. 20329 Figure Legend: Receiver Operating Characteristic Curves for In-Hospital Mortalityq. SOFA indicates quick Sequential Organ Failure Assessment; SIRS, systemic inflammatory response syndrome; and SOFA, Sequential [Sepsis-related] Organ Failure Assessment. The area under the receiver operating characteristic curves for q. SOFA is 0. 80 (95% CI, 0. 74 -0. 85); SOFA, 0. 77 (95% CI, 0. 71 -0. 82); SIRS, 0. 65 (95% CI, 0. 59 -0. 70); and severe sepsis, 0. 65 (95% CI, 0. 59 -0. 70). Date of download: 2/2/2017 Copyright © 2017 American Medical Association. All rights reserved.

In conclusion, q. SOFA scores were associated with inhospital mortality, hospital admission, ICU admission, and hospital length of stay in adult ED patients likely to be admitted both with and without suspected infection. q. SOFA is an easy tool that can be used in the ED to predict outcomes. Further prospective validation of the q. SOFA is required before widespread use.

ICD-10 koder for sepsis, endringer 2017 Endringsdokument for norsk utgave av ICD-10 2016 -2017 Direktoratet for e-helse 27. 09. 2016
 og infeksjonskoder")
Forslag • I tillegg tilandre sepsiskoder (eks A 40 og A 41) og infeksjonskoder foreslår vi at det også brukes koden: • R 65. 1 ved sepsis (ny definisjon) hvor det foreligger dokumentasjon av organsvikt, eks ved SOFA skår økning ≥ 2 poeng • R 57. 2 ved septisk sjokk (ny definisjon) • Da vil en lettere både på egen institusjon samt fra NPR enkelt kunne hente ut informasjon om omfanget av sepsis ved norske sykehus!

According to family spokesman Bob Gunnell, was "septic shock due to unspecified natural causes. "
- Slides: 32