Sepsis Starts with SIRS Severe systemic response to

















- Slides: 19
Sepsis
Starts with SIRS ▪ Severe systemic response to a condition that provokes an acute inflammatory reaction ▪ SIRS is nonspecific and can be caused by ▪ Ischemia ▪ Trauma ▪ Reperfusion injury ▪ Multisystem injury
As time goes by § § § § Decreased LOC Respiratory Depression Diminished bowel sounds Jaundice Oliguria or anuria Increased pulmonary arterial pressure Decreased cardiac output
Diagnostics ▪ ABG ▪ Hypoxemia with either respiratory or metabolic acidosis ▪ CBC may reveal decreased hemoglobin and hematocrit as well as leukocytosis ▪ If sepsis is severe, may have very low white count ▪ X-rays may indicate fractures, C-spine injury, pulmonary infiltrates, or abnormal air or fluid in the chest or abdominal cavities ▪ Additional tests that may be performed include MRI, CT scan, and angiography
Nursing Interventions ▪ Maintain airway ad breathing with use of mechanical ventilation and supplemental oxygen ▪ Monitor VS, )2 sat, hemodynamic parameters, & cardiac rhythm ▪ Administer IV fluids ▪ Monitor labs ▪ Monitor I & O ▪ Administer meds ▪ Provide emotional support to pt and family ▪ Explain diagnostic tests & treatments
Septic shock ▪ Characterized by low systemic vascular resistance and an elevated cardiac output ▪ Occurs in response to infections that release microbes or immune mediators ▪ Tumor necrosis factor ▪ Interleukin-1
Organisms that account for up to 70% of cases ▪ Gram negative bacteria ▪ E coli ▪ Klebsiellosis pneumoniae ▪ Serratia ▪ Enterobacter ▪ Pseudomonas
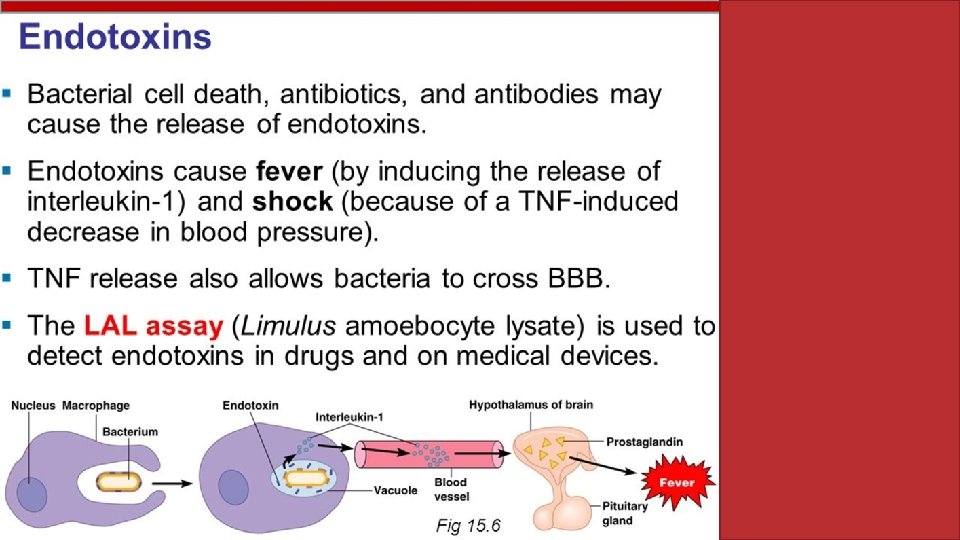
Endotoxins ▪ Some bacteria release endotoxins ▪ In response, macrophages secrete TNF and interleukins ▪ These mediators are responsible for increased release of ▪ Platelet activating factor ▪ Prostaglandins ▪ Leukotrienes ▪ Thromboxane A 2 ▪ Kinins ▪ complement
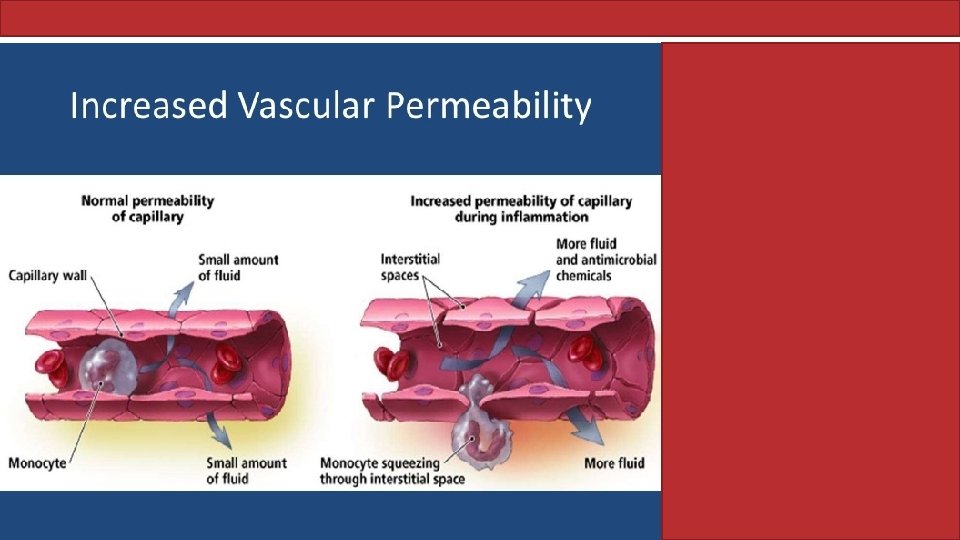
Compromised Capillaries ▪ Consequences of the immune activity: ▪ ▪ ▪ Vasodilation and vasoconstriction Increased capillary permeability Reduced systemic vascular resistance Microemboli Elevated cardiac output ▪ Endotoxins also stimulate the release of histamine ▪ Causes further capillary permeability
Heart trouble ▪ TNF, PAF, and other inflammatory mediators depress myocardial function ▪ This leads to decreasing cardiac output ▪ Results in multisystem organ failure
Who’s at greatest risk ▪ Elderly patients ▪ Also, anyone with impaired immunity
So what do you look for ▪ Patient history ▪ Disorder or treatment that causes immunosuppression ▪ History of invasive tests or treatments ▪ History of surgery ▪ History of trauma ▪ Signs ▪ May have fever and chills ▪ 20% may be hypothermic
Phase facts ▪ Hyperdynamic phase ▪ ▪ ▪ ▪ Early/warm Increased cardiac output Peripheral vasodilation Decreased systemic vascular resistance Altered LOC Rapid, shallow respirations Decreased urine output Rapid, full, bounding pulse ▪ Hypodynamic phase ▪ Decreased cardiac output ▪ Peripheral vasoconstriction ▪ Variable to increased systemic vascular resistance ▪ Inadequate tissue perfusion ▪ Pale and possibly cyanotic skin color ▪ Mottling of extremities ▪ Lethargy ▪ Decreased or absent urine output ▪ Cold and clammy skin ▪ Absence or decreased peripheral pulses ▪ Hypotension
Diagnostics ▪ Positive blood cultures ▪ CBC ▪ Presence or absence of anemia & leukopenia ▪ Severe or absent neutropenia ▪ Usually thrombocytopenia ▪ ABG ▪ Metabolic acidosis ▪ Hypoxemia ▪ Low Paco 2 that progresses to increased Paco 2 ▪ BUN and creatinine increased ▪ Coags are increased, platelets are decreased, and fibrin split products are increased ▪ CXR may reveal pna or ARDS ▪ ECG may show ST depression and inverted T waves ▪ Amylase & lipase may show pancreatic insufficiency ▪ Hepatic enzyme levels are elevated due to liver ischemia ▪ Blood glucose levels are initially elevated and then decrease
Initial nursing actions ▪ Assess ABCs ▪ Closely monitor cardiopulmonary status ▪ Monitor oxygen saturation and ABG results ▪ Prepare for possible intubation ▪ Semi-fowlers ▪ Keep pt quiet and comfortable
Vital moves ▪ Continuously VS monitoring ▪ Observe skin color and check cap refill ▪ Monitor for SBP, immediate intervention if this drops below 90 ▪ Monitor MAP; notify MD if this drops below 65 -70 ▪ If pt already has an invasive line, prepare to DC and send for culture ▪ Prepare to insert new lines ▪ Obtain blood culture ▪ Start antibiotics (prefer within an hour)
Vital moves cont’d ▪ Continuous cardiac monitoring ▪ Monitor I & O ▪ Administer IV fluids but monitor fluid overload ▪ Administer positive inotropic agents as ordered ▪ Monitor labs-watch for possible DIC ▪ Provide emotional support and family education