Sensory System By Dr Abdel Aziz M Hussein

Sensory System By Dr. Abdel Aziz M. Hussein Assist. Prof. of Medical Physiology Member of American Society of Physiology

Headache

Headache Def: • Pain felt in the head region • It is an example of referred pain from deep structures of head Pain sensitive structures in the head A) Extracranial structures 1. All structures in the scalp , covering skull including skin, fasciae, ms, arteries and nerves 2. Eyes 3. Paranasal sinuses 4. Teeth
 Intracranial structures • Brain is insensitive")
Headache Pain sensitive structures in the head B) Intracranial structures • Brain is insensitive to pain • Some structures are sensitive to pain e. g. 1. Arteries e. g. middle meninegial arteries 2. Venous sinuses 3. Parts of dura covering skull base 4. Cranial nerves carrying pain V, IX, X
 Frontal headache: • Due to")
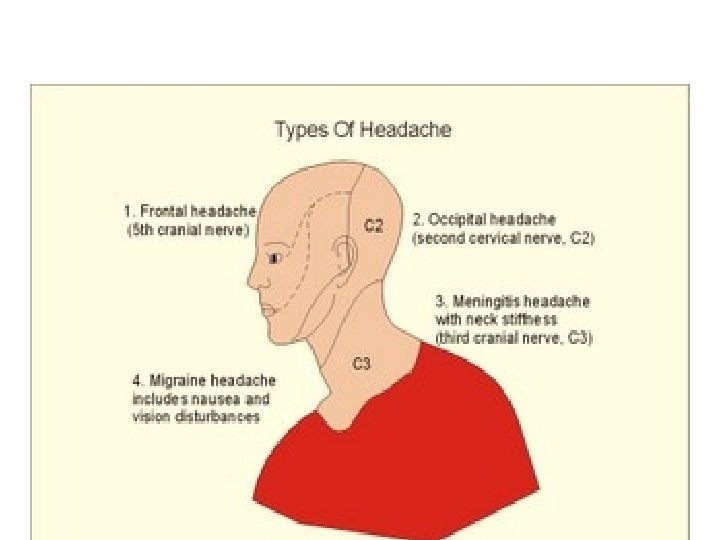
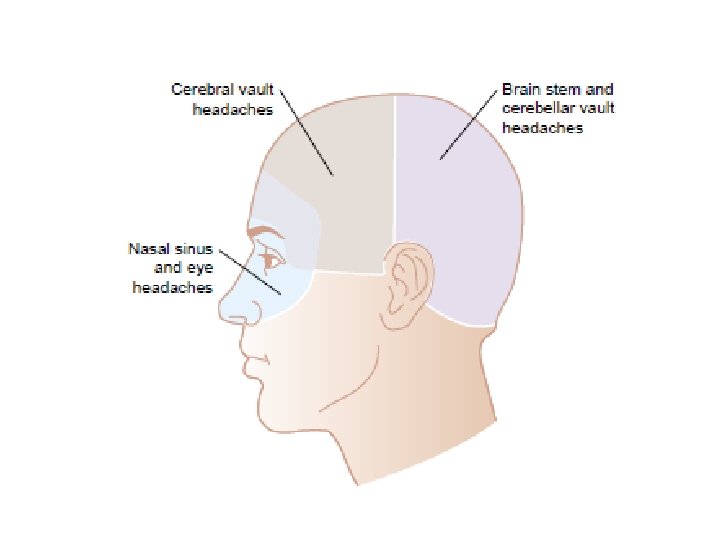
Headache Site of referral of intracranial headache : A) Frontal headache: • Due to stimulation of pain receptors above tentorium (referred by trigeminal nerve) B) Occipital headache: • Due to stimulation of pain receptors below tentorium (referred by 2 nd cervical nerve)

Headache Mechanism: 1. Irritation of pain sensitive structures e. g. in case of meningitis 2. Pressure or traction on pain sensitive structures e. g. in brain tumors 3. Dilatation of pain sensitive structures e. g. arterial dilatation and brain tumors 4. Spasm of ms e. g. spasm of neck and head ms

Headache Causes of Extracranial headache: • Due to stimulation of pain receptors in extracranial structures by; 1. Spasm of head and neck ms due to emotional tension (psychogenic headache). 2. Sinusitis: inflammation of nasal sinuses 3. Eye diseases: a) Glaucoma →increased intraocular pressure b) Errors of refraction e. g. astigmatism and myopia 4. Oral causes: e. g. teeth caries.

Headache Causes of Intracranial headache: 1. Meningeal irritation e. g. meningitis, trauma, alcoholics and constipation (absorption of toxins from rectum which cause meningeal irritation) 2. Brain tumours cause pressure, traction, or dilatation of intracranial pain sensitive structures. 3. Changes in CSF pressure: a) ↓ CSF pressure → compensatory dilatation of blood vessels
 Changes in CSF pressure: b) ↑ CSF pressure")
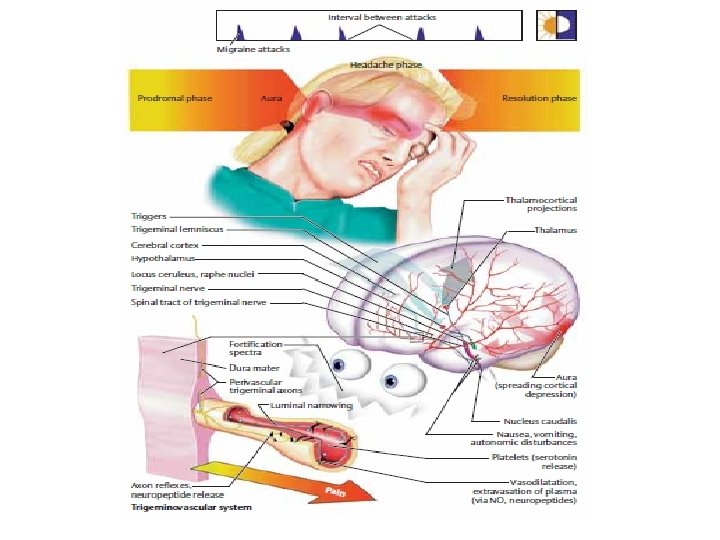
Headache Causes of intracranial headache: 3) Changes in CSF pressure: b) ↑ CSF pressure → pressure and traction on pain sensitive structures e. g. in hydrocephalus 4) Dilatation of intracranial arteries : a. Pulsation of arteries and severe headache as in migraine (due to release of histamine) • Characterized by sudden or paroxysmal attacks of throbbing pain with blurring of vision even nausea and vomiting. b. Hypertension also leads to dilatation of cerebral vessels and headache

Somatic Sensory Cortex

Somatic Sensory Pathways

Somatic Sensory Cortex

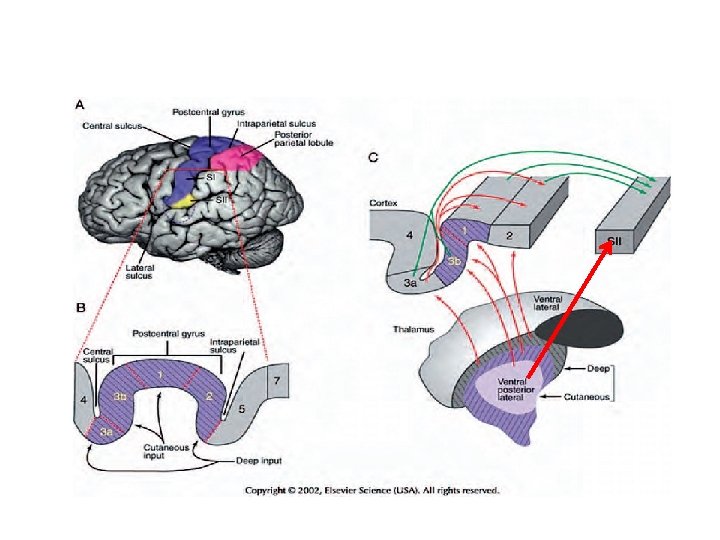
Somatic Sensory Cortex Def. • It is the part of cerebral cortex that is concerned with perception and interpretation of somatic sensations Types: A) Somatic sensory areas: 1. 1 ry somatic sensory area I (area 3, 1, 2) 2. 2 ry somatic sensory area II (area 40) B) Somatic sensory association areas (area 5, 7)

Area 3, 1, 2 Area 5, 7
 Site: • Post central gyrus of the parietal lobe")
1) Site: • Post central gyrus of the parietal lobe
 Structure : • Consists of 6 layers from the surface to inside")
2) Structure : • Consists of 6 layers from the surface to inside
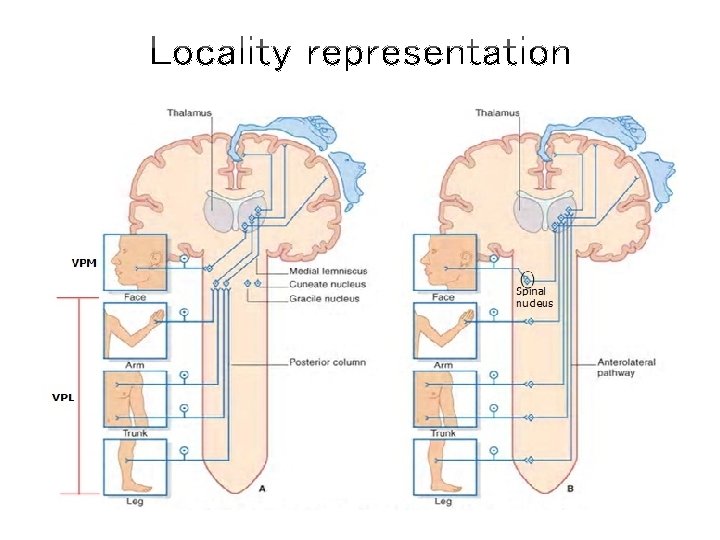
 Body representation: Locality representation 1. Contralateral (crossed) 2. Inverted or upside down 3.")
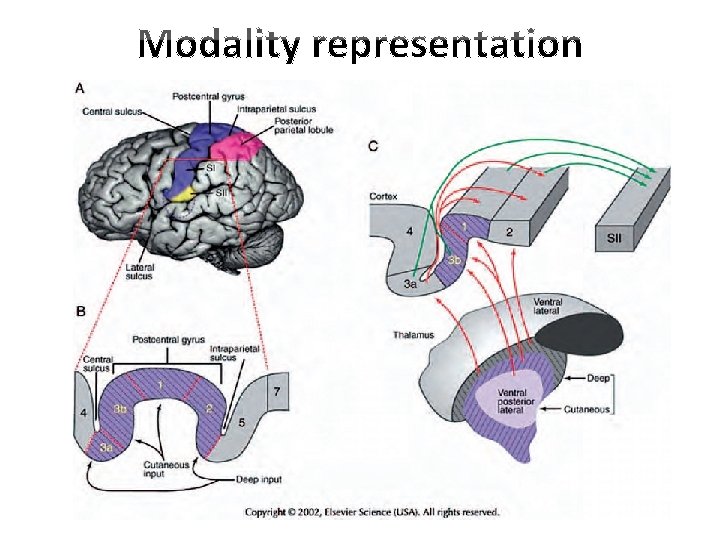
3) Body representation: Locality representation 1. Contralateral (crossed) 2. Inverted or upside down 3. Definite somatotopic organization 4. Proportionate with sensory function of organ or number of receptors Modality representation • Its neurons arranged into columns , each column respond to specific modality • Pain and temp. have no specific columns but few scattered neurons ( ) mechanoceptive columns
 Crossed or contralateral i. e. receives impulses from opposite side of body")
a) Crossed or contralateral i. e. receives impulses from opposite side of body
 Inverted upside down (except face) : head represented in lower part while leg")
b) Inverted upside down (except face) : head represented in lower part while leg represented in upper part
 Definite somatotopic map or organization i. e. each part of the")
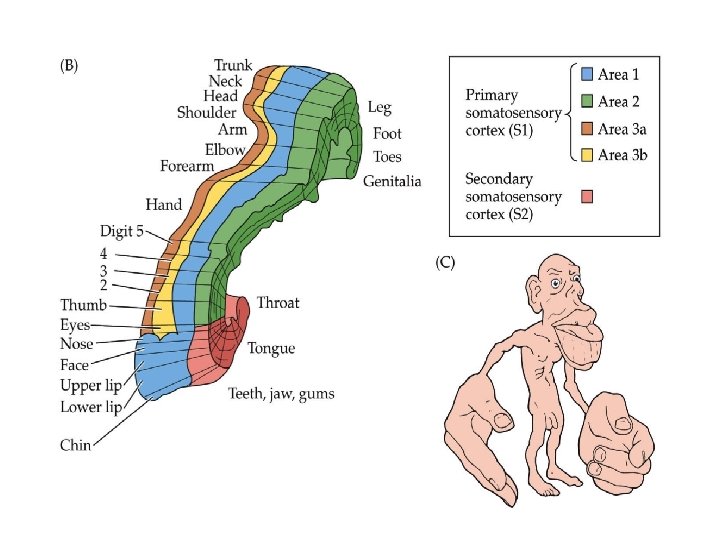
Sensory Homunculus c) Definite somatotopic map or organization i. e. each part of the body has a specific region in SMI

Sensory Homunculus
 Related to functions: size of the represented part is proportionate with its function")
d) Related to functions: size of the represented part is proportionate with its function not its size e. g. fingers, lips and face represented by large, while the trunk represented by small areas. • The peripheral parts of the body are widely represented due to; 1. great number of receptors 2. greater number of the afferents 3. little convergence

Touch sensation Proprioceptive sensations Deep Pressure
 Functions: receives nearly all somatic sensations a) b) c) d) • Fast pain")
3) Functions: receives nearly all somatic sensations a) b) c) d) • Fast pain Fine touch Fine grades of temperature Deep sensations pressure, tension, vibration, position, movements It is concerned with the perception or discrimination of the intensity, locality and fine grades of the sensory stimuli without disclosing their meanings.
 Damage : 1. Inability to localize accurately the site of different stimuli. 2.")
4) Damage : 1. Inability to localize accurately the site of different stimuli. 2. Inability to perceive minute differences in the intensity of sensory stimuli. 3. Astereognosis i. e. inability to recognize the shapes or forms or texture of materials. 4. Loss of fine touch and orientation of different parts of body to each other.
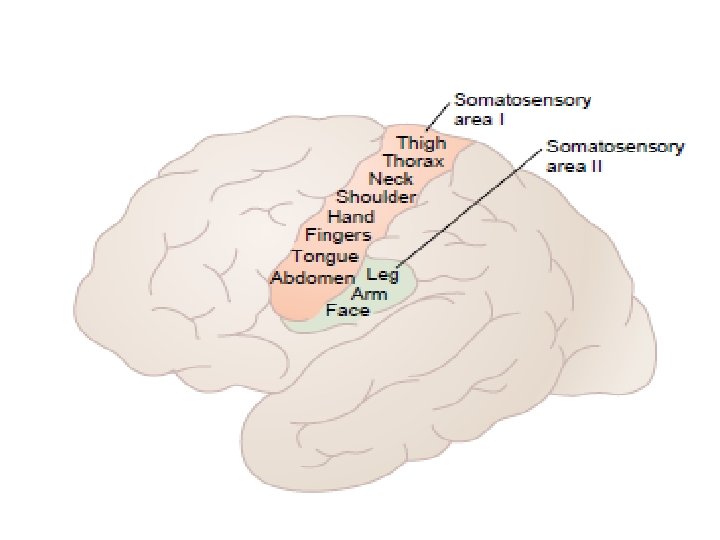
 Site: Site • Parietal lobe posterior and inferior to lower end of area")
1) Site: Site • Parietal lobe posterior and inferior to lower end of area I 2) Representation: • less sharp than area I • Face represented anterior and legs represented posterior • Receives direct input from VPN of thalamus and from the primary somatic sensory cortex
 Functions: • Start the meaning of somatic sensations 4) Damage: • Defect in")
3) Functions: • Start the meaning of somatic sensations 4) Damage: • Defect in learning based on tactile discrimination
 1) Site: • Parietal lobe behind area")
Somatic Sensory Association Area (Area 5, 7) 1) Site: • Parietal lobe behind area I and above area II
 Connections: Area 3, 1, 2 Non specific thalamic nuclei")
Somatic Sensory Association Area 2) Connections: Area 3, 1, 2 Non specific thalamic nuclei PVNT Area 5, 7 Auditory area Visual area
 Functions : 1. Give the meaning of all types")
Somatic Sensory Association Area 3) Functions : 1. Give the meaning of all types of sensations received from primary sensory areas 2. Transmit the pre-analyzed kinesthetic sensory information to brain motor centers that helps in control and coordination of movements.
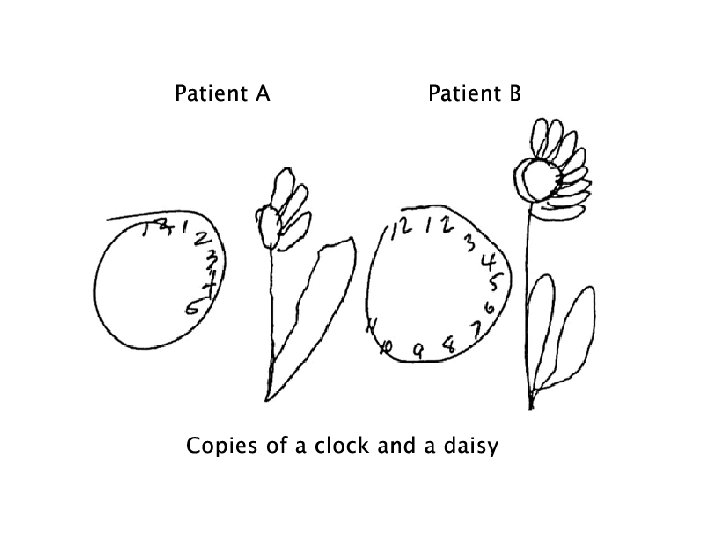
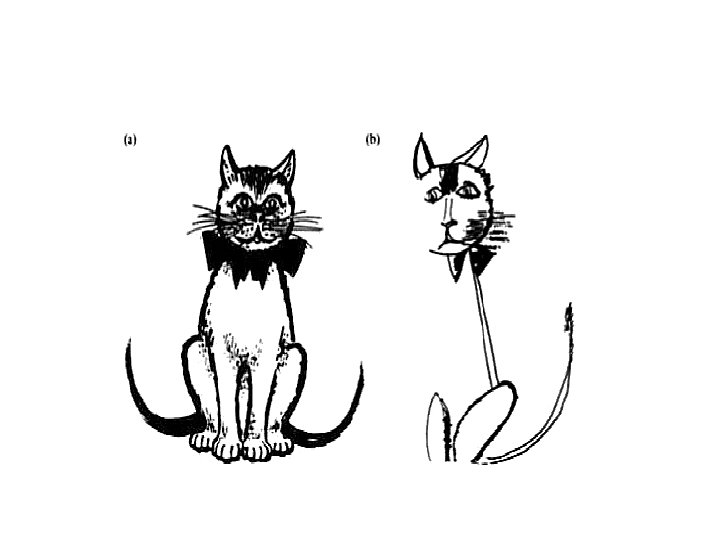
 Lesion : 1. Astereognosis (loss of ability to recognize")
Somatic Sensory Association Area 4) Lesion : 1. Astereognosis (loss of ability to recognize the complex objects). 2. The sensory information from the opposite side of the body are ignored and neglected and even the brain forgets the other ½ of the body and often forgets to use the contralateral side of his body (Parietal lobe neglect).

Sensory Disturbances

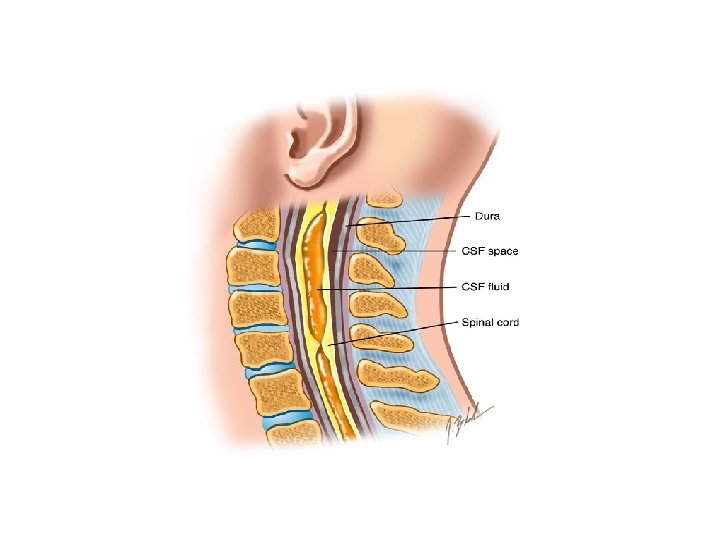
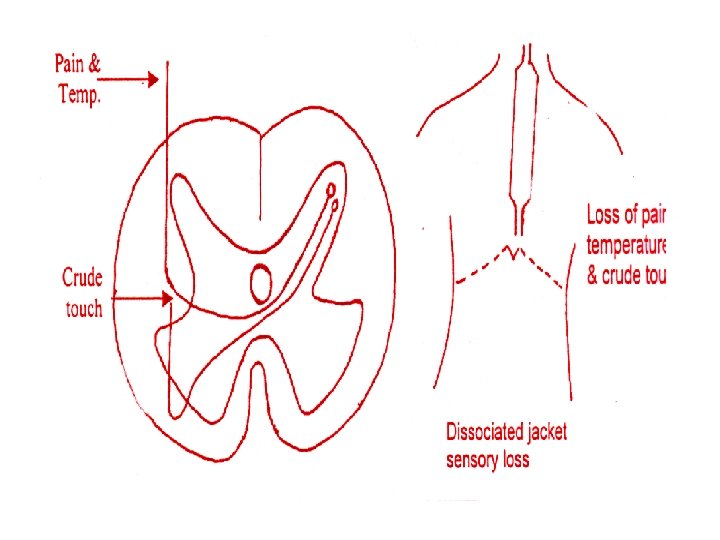
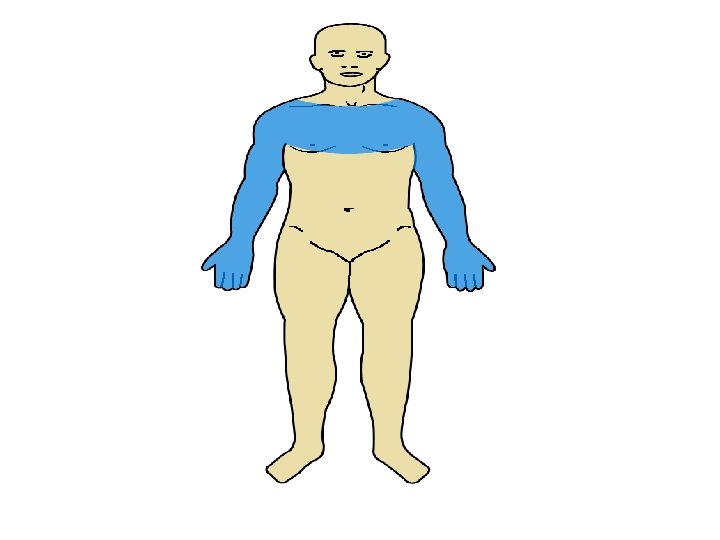
Syringomyelia Def. • Cystic dilatation of central canal of spinal cord Site: • Lower cervical and upper thoracic segments Effect : • Damage of crossing fibers → loss of pain, temp and crude touch only (dissociated) on both sides of body which have jacket distribution
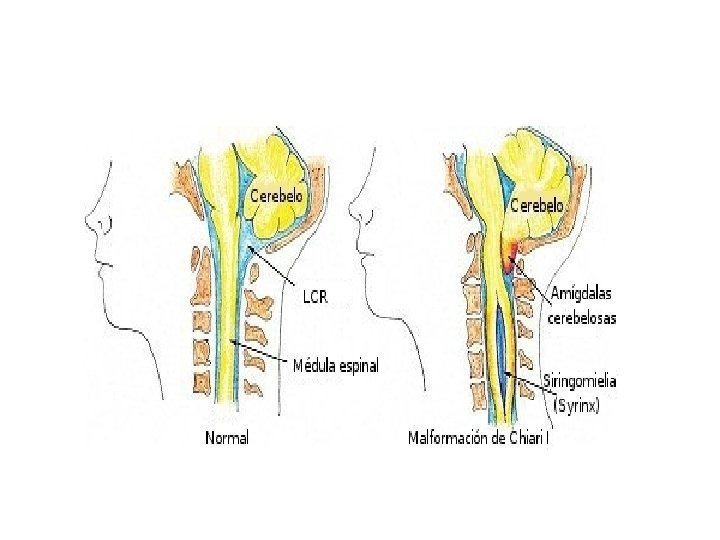

• Pain • Temp. • Crude touch Ventral and lateral spinothalamic tracts

Tabes Dorsalis Def. • Chronic degenerative disease of dorsal root of spinal central to DRG Cause: • Syphilis of CNS Site: • Usually lumbosacral region and cervicothoracic regions Mechanism: • Syphilis causes inflammation leading to irritation followed by compression and degeneration.

 Initial hyperesthesia with frequent attacks of severe pain (may be")
Tabes Dorsalis Manifestations: 1) Initial hyperesthesia with frequent attacks of severe pain (may be referred to skin, muscle or bone) (due to irritation of nerves) 2) Compression and degeneration of nerves results in; a) Loss of pain sensation: • Fast pain is lost 1 st followed later by loss of the slow pain b) Loss of temperature sensation: c) Loss of crude, fine touch, pressure and vibration • This is due to damage of the fibers ascending in the post-column at the level of lesion.
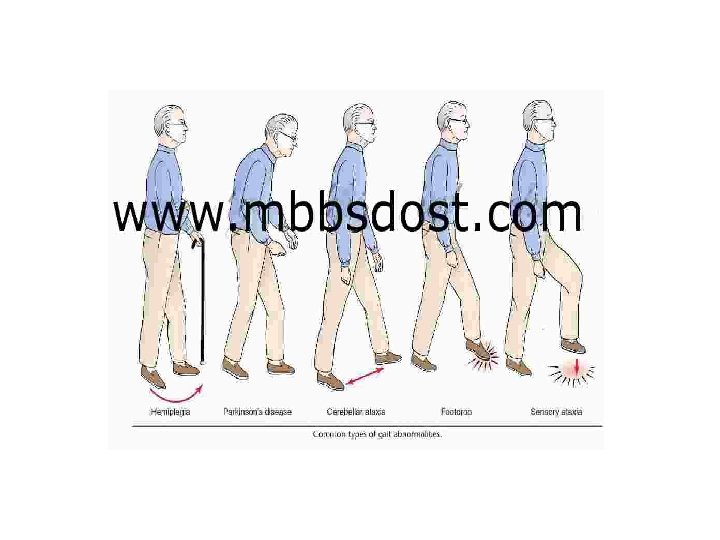
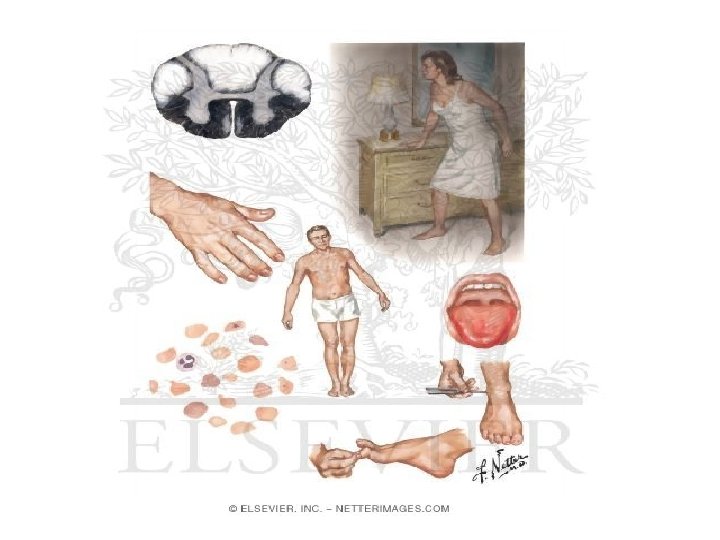
 Loss of kinesthetic sensation: results in; i) Sensory ataxia (uncoordinated")
Tabes Dorsalis Manifestations: d) Loss of kinesthetic sensation: results in; i) Sensory ataxia (uncoordinated voluntary movements due to loss of both senses of position and movements of joints) • This makes the patient moves in a “stamping gait” ii) Positive Romberg’s sign • if the tabetic patient closes his eyes (e. g. ) during washing his face, he sways or may even fall. • This is because of loss of both mechanisms maintaining equilibrium, vision and sense of position. • N. B. : These two signs are important to differentiate sensory and motor ataxia.
 Loss of Reflexes: mediated by the affected segments whether,")
Tabes Dorsalis Manifestations: • e) Loss of Reflexes: mediated by the affected segments whether, 1. Superficial reflexes: (e. g. flexion withdrawal reflex appearance of ulcers in the skin 2. Deep reflexes: (e. g. stretch reflex loss of muscle tone and tendon jerks 3. Visceral reflexes: (e. g. micturition reflex, defecation reflex and erection reflex. • These changes occurs if the sacral roots are damaged on both sides.

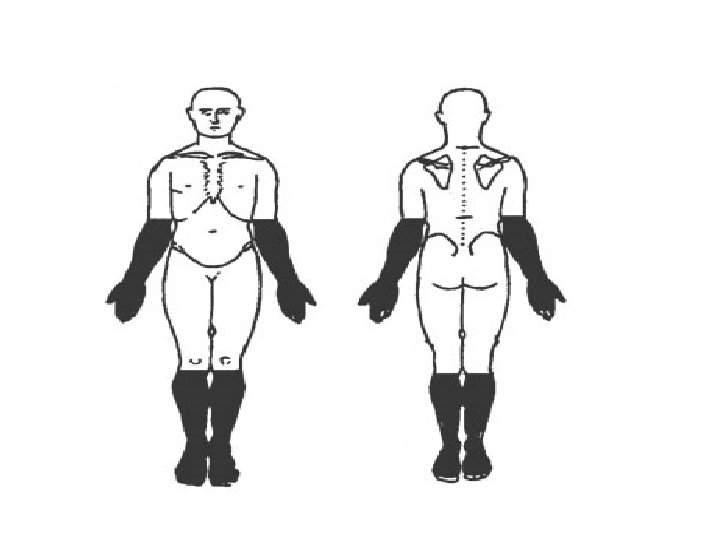
Peripheral Neuritis Def. , • Inflammation or degeneration of peripheral nerves of distal parts of limbs Causes: 1. Vit deficiency 2. Metabolic e. g. DM 3. Toxic e. g. alcohol 4. Infective e. g. viral or bacterial Manifestations: 1. Sensory disturbances : hypothesia or anaethesia of distal parts of limbs (glove and stock) 2. Motor disturbances : paresis or paralysis of distal parts of limbs

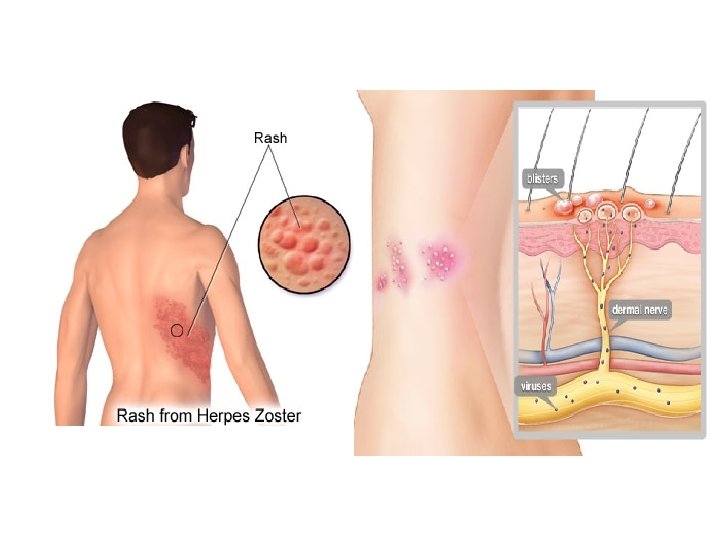
Herpes Zoster • Def. • It’s disease caused by a virus which infects and irritates the cell bodies of the D. R. G. • Site: • Mainly affects thoracic D. R. G. • Manifestations: • Severe attacks of pain in the dermatomal segments supplied by the ganglion.

THANKS
- Slides: 63