Sensory Processing and Self Regulation Sarah Macneil Sarni









 patterns Attention & concentration difficulties Sleep")


 • Deep pressure touch with Therapressure Brush and • Joint")













- Slides: 27
Sensory Processing and Self Regulation Sarah Macneil Sarni Peters Paediatric Network Meeting 6. 11. 14
Our senses Five senses • Sight, Touch, Hear, Taste, Smell Two “body position” senses Proprioceptive sense: • From our muscles and joints • Gives us sense of body awareness (not reliant on vision) Vestibular sense: • From our inner ear • Direction, rotation, speed
Sensory Processing • The way our nervous system receives, filters, organises and integrates the messages from our senses in order to produce an appropriate motor and behavioural response • Efficiently making sense of our body and the environment
Sensory Processing Dysfunction • Pathways and systems to process, organise and filter the sensory information being received don’t function as they should • “a traffic jam in the brain”
How do you get going in the morning? • What helps you to get the day started right?
Sensory Processing
A 5 year old girl Primary sensory symptoms: Secondary symptoms: Motor skills: • Fluctuating arousal • Can be anxious • Sleep issues • Planning issues • Clumsy • Difficulty holding a pencil • Leans on other people/furniture Irritated & Bothered by: • • • Clutter Loud noises New noises Background noise Inconsistent eye contact Coping styles & strategies: Sensory seeker: • Movement • Tactile • Oral (chewing) Can be seen as controlling Tantrums Likes routines
Sensory Defensiveness • Sensory Defensiveness is the over activation our protective senses • People with sensory defensiveness respond to harmless sensations as if they were irritating, dangerous, or even painful.
Brain function & Sensory defensiveness
Common secondary issues: o o Abnormal arousal (alertness) patterns Attention & concentration difficulties Sleep difficulties Social / emotional issues (fear, anxiety) Common coping strategies: o o Seeking behaviours Withdrawal or aggression Inflexibility / fixed in ways Cognitive strategies eg. self talk
Fluctuating levels of Arousal
What we can do about SD • Educate parents and teachers about SD • A Sensory Diet of daily activities • Professionally guided treatment – Therapressure Program (Wilbarger protocol) – Oral-tactile Technique
Therapressure Program (Wilbarger Protocol) • Deep pressure touch with Therapressure Brush and • Joint compressions • Must be applied every 90 -120 minutes 8 -10 times per day.
Therapressure Program Evidence • Current studies: – small samples; – single subject case studies • All studies however present positive findings • Not conclusive support, but clinical use justified • Additional well-controlled studies are needed
Related research / theory base • Evidence from Massage – ↑serotonin ↑dopamine ↑endorphins ↓cortisol • Evidence from Acupuncture ↑endorphins (short term benefits on pain) ↑serotonin (over time, this level remains higher)
Oral Tactile Technique • A professionally guided treatment for Oral Defensiveness • Involves: – 3 sweeps of moderate touch input (not deep pressure) across front and upper part of inside of mouth – Gentle proprioception through lower jaw by pressing on bottom teeth – 2 -3 times • Must be applied 6 -7 times per day
Arousal Theory • A state of the nervous system describing how alert one feels. • To attend, concentrate and perform tasks in a manner suitable to the situational demands, one’s nervous system must be in an optimal state of arousal for that particular task
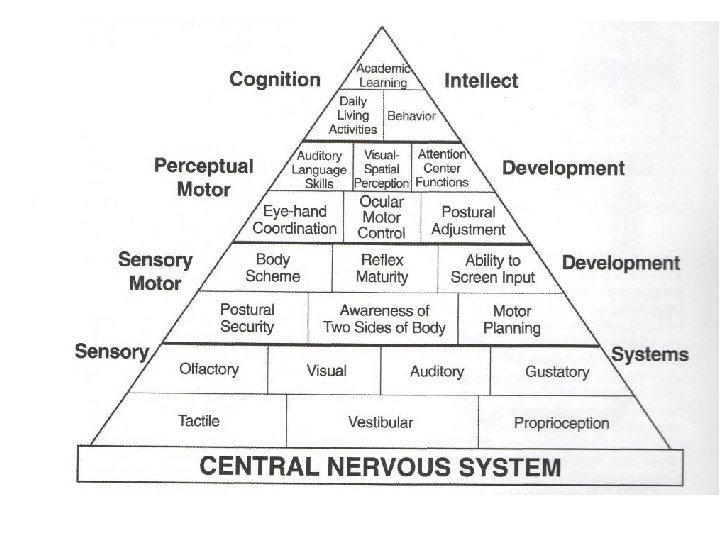
Self Regulation • A person’s ability to change the level of arousal appropriate to a given task or situation • Need to be focused and self regulated to do any of the “top of the pyramid” activities effectively
Top Down vs Bottom Up • Brainstem – responsible for the 4 A’s incl. regulation of automatic bodily functions • Cerebellum - processes the information it receives from the body (muscles and joints) - has connections to brainstem and cortex • Cortex – “the thinking part” -makes and expresses meaning of things - Responsible for higher level cognitive skills
Top Down • Use of cortex to “talk yourself” into appropriate level of alertness • Traditional approach to regulating behaviour
Bottom Up • Use of cerebellum to alter arousal state • Provide input to the cerebellum which communicates with brainstem to alter state of alertness • So what types of input should we be providing via the cerebellum for the bottom-up approach?
5 Ways to influence Self Regulation • Mouth – suck/blow, bite/crunch, chew, lick • Move - joint & muscle activity, bouncing, swinging, spinning • Touch - deep pressure, light touch, joint & muscle work incl fidgeting • Look - light, darkness, colours • Listen – music, noise, quiet
How do you get going in the morning? • • • Consider our list? Mouth Move Touch Look Listen
Sensory Diet Out of bed Stamping up to kitchen Breakfast Smoothie with straw, crunchy cereal Crab walk to teeth and dress Kinder (variety of tasks) Afternoon/evening Trampoline, outdoor incl. monkey bar, water bottle through straw, bear hugs, wrestling Dinner time “dynamic seat” Bedtime massage, quiet music, tuck in tight, lava lamp
Summary • Education – parents, families, teachers, children themselves • Understanding of top down vs bottom up approach • Sensory diet as part of normal routine • Equipping families and schools with tools to assist self regulation
References • Sensory Defensiveness – A comprehensive treatment approach workshop manual • How does your engine run? A leaders guide to the Alert Program for self regulation • Out of the mouth of babes – discovering the developmental significance of the mouth • http: //spdfoundation. net/