Seminar Complicated Cystitis Physical examination Vital signs Febrile

Seminar Complicated Cystitis

Physical examination Vital signs : Febrile? ? PV MIUB : Atrophy Vagina : Atrophy Cervix : No lesion Uterus : Normal size Adnexa : No mass

Problem List Terminal Dysuria

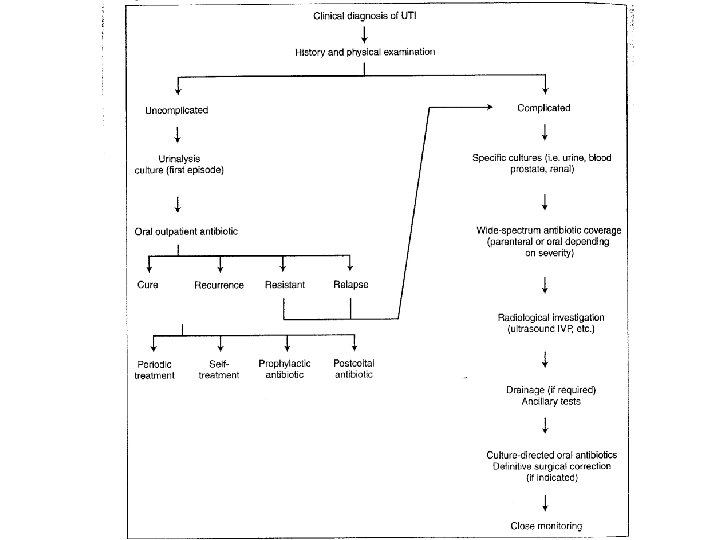
Differential Diagnosis • Cystitis • Vaginitis • Urethritis

Investigation • Urinalysis • Urine culture • Pap smear

Urinalysis Color Yellow Clarity Cloudy SG 1. 025 p. H 6. 0 Prot 3+ Glu Negative Keto Negative Blood Bili Uro Nitri Leuco Microscopic Examination result WBC Numerous/HP RBC Many/HP Epith Squamous cell 3 -5/HP Epith Translational cell 0 -1/HP 3+ Negative Normal Negative 2+

Urine culture • Streptococcus SPP. 5000 CFU/ml • Corynebacterium SPP. 5000 CFU/ml

Pap smear • Normal

Impression Cystitis
 1 tab po bid x 3 day")
Treatment • Norfloxacin (400) 1 tab po bid x 3 day
 Urinalysis Color Yellow Clarity Cloudy SG 1. 020 p. H 5.")
Second visit (25/7/2540) Urinalysis Color Yellow Clarity Cloudy SG 1. 020 p. H 5. 5 Prot 1+ Glu Negative Keto Negative Blood Bili Uro Nitri Leuco Microscopic Examination result WBC Many/HP RBC 10 -15/HP Epith Translational cell 1 -2/HP 2+ Negative Normal Negative 2+

. . 7 months later. .
 Urinalysis Color Yellow Clarity Turbid SG p. H Prot Glu Keto")
Third visit (2/2/2541) Urinalysis Color Yellow Clarity Turbid SG p. H Prot Glu Keto 1. 025 5. 5 2+ Negative Blood Bili Uro Nitri Leuco Microscopic Examination result WBC Many/HP RBC 30 -35/HP Epith Squamous cell rare/HP Epith Translational cell rare/HP 3+ Negative Normal Negative 3+
 • Impression: Cystitis • Medications: Norfloxacin (200 mg) 2 tab PO")
Third visit (2/2/2541) • Impression: Cystitis • Medications: Norfloxacin (200 mg) 2 tab PO bid pc #28 • Follow up 7 days, UA before visit doctor
 • Chief complaint: อาการไมดขน • PV: Normal • UA: พบ WBC,")
Fourth visit (9/2/2541) • Chief complaint: อาการไมดขน • PV: Normal • UA: พบ WBC, RBC numerous ไมพบแบคทเรย
 r Urinalysis Color Yellow Clarity Turbid SG p. H Prot Glu")
Fourth visit (9/2/2541) r Urinalysis Color Yellow Clarity Turbid SG p. H Prot Glu Keto 1. 025 5. 5 3+ 3+ Negative Blood Bili Uro Nitri Leuco Microscopic Examination result WBC Numerous/HP RBC 3 -5/HP Epith Translational cell rare/HP Bact Bacilli & Cocci few/HP 3+ Negative Normal Negative 3+
 Impression Chronic cystitis suspected for underlying disease")
Fourth visit (9/2/2541) Impression Chronic cystitis suspected for underlying disease
 • Medications: Norfloxacin (200 mg) 1 tab qid pc PO #20")
Fourth visit (9/2/2541) • Medications: Norfloxacin (200 mg) 1 tab qid pc PO #20 • Urine culture • Follow up 3 days

Problem list Persistant pyuria Persistant hematuria Noresponse to medication

Differential Diagnosis Chronic cystitis Urolithiasis

Chronic cystitis • Unresolved or persistent bladder infection • 3 or more bouts of bladder infection occurring in the course of 1 year
 Associated with Infectious vaginitis Urethitis Renal infection")
Chronic cystitis Infectious Tuberculosis (Sterile pyuria) Associated with Infectious vaginitis Urethitis Renal infection

Non infectious Calculi Hormonal deficiency - Senile Vaginitis - Urethitis Interstitial cystitis Allergic cystitis Radiation cystitis Chemotherapeutic agent >>Cystitis
 • Non infectious Hormonal deficiency")
Differential Diagnosis Chronic cystitis • Infectious Tuberculosis (Sterile pyuria) • Non infectious Hormonal deficiency - Senile Vaginitis - Urethritis Interstitial cystitis Urolithiasis

Differential Diagnosis Urolithiasis
 • Urine culture results: negative • CXR normal • and plan")
Fifth visit (13/2/2541) • Urine culture results: negative • CXR normal • and plan for IVP at 23/2/2541

Indication for IVP • To detect radioluscent calculi. • Recurrent urinary infection to find out renal abnormality. • Congenital abnormalities of the Urinary tract like horse shoe kidney, double ureters etc. • Neoplastic disease of the urinary tract. • In abdominal and renal trauma. • To study obstructive diseases of urinary tract.
 • IVP: - No opaque stone - Focal caliectasis of left")
Sixth visit (23/2/2541) • IVP: - No opaque stone - Focal caliectasis of left lower pole kidney, possibly non opaque stone - Contract bladder with thicken wall, most likely chronic cystitis Impression: Frequent UTI & Abnormal lower pole of left kidney • Consult urologist
 • • Terminal dysuria and Nocturia Reevaluate IVP Normal study Plan")
Seventh visit (27/2/2541) • • Terminal dysuria and Nocturia Reevaluate IVP Normal study Plan for cystoscope at 7/4/2541 Medications: Flavoxate, Imipramine

Indication for cystoscope (1 frequent or persistent urinary tract infections (2 blood in the urine (hematuria( (3 loss of bladder control (incontinence ( (4 abnormal cells found in urine sample (5 painful urination or unexplained pelvic pain associated with urination (6 poor bladder emptying due to prostate enlargement or stricture of the urethra (7 any abnormal growth, lesion, or tumor seen on other imaging studies.
 • Cystoscope findings: – Generalized hyperemia of bladder mucosa – Bleeding")
Eighth visit (7/4/2541) • Cystoscope findings: – Generalized hyperemia of bladder mucosa – Bleeding when dilatation with water – No tumor mass – Impression: Interstitial cystitis – Biopsy bladder was done • Plan: Urine culture 3 days, Urine AFB • Rx: Norfloxacin • Follow up 2 week
 • Terminal dysuria, Nocturia เพมขนเปน 10 ครง • No CVA tenderness")
Ninth visit (24/4/2541) • Terminal dysuria, Nocturia เพมขนเปน 10 ครง • No CVA tenderness • Biopsy result: Granulomatous inflammation consistent with tuberculosis • Urine AFB stain: negative • Plan: Start HRZE, CXR, Sputum AFB 3 days • Rx: Imipramine
 • Urine Culture : Mycobacterium tuberculosis • นด 3 เดอน UA")
Tenth visit (19/6/2541) • Urine Culture : Mycobacterium tuberculosis • นด 3 เดอน UA before visit

TB cystitis

TB cystitis • Chronic cystitis that refuse to response to adequate therapy • Finding of pus without bacteria in a methylene blue stain or culture of urine sediment • Gross /Microscopic hematuria • Non tender , enlarged epididymis with beaded or thickened vas • Chronic draining scrotal sinus • Induration or nodulation of prostate and thickening of one or both seminal vesicles (especially in a young man )

Seminar Complicated Cystitis
- Slides: 48