SEMESTER II PAPER CC3 T TOPIC EXCITABLE TISSUE

SEMESTER: II PAPER: CC-3 T TOPIC: EXCITABLE TISSUE: MUSCLE Monoj Maiti, State Aided College Teacher, Department of Physiology, Bajkul Milani Mahavidyalaya, Kismat Bajkul, 721655, Purba Medinipur, W. B. Email id. maitimonoj@gmail. com Contact No. : 8343069741/ 8759921286
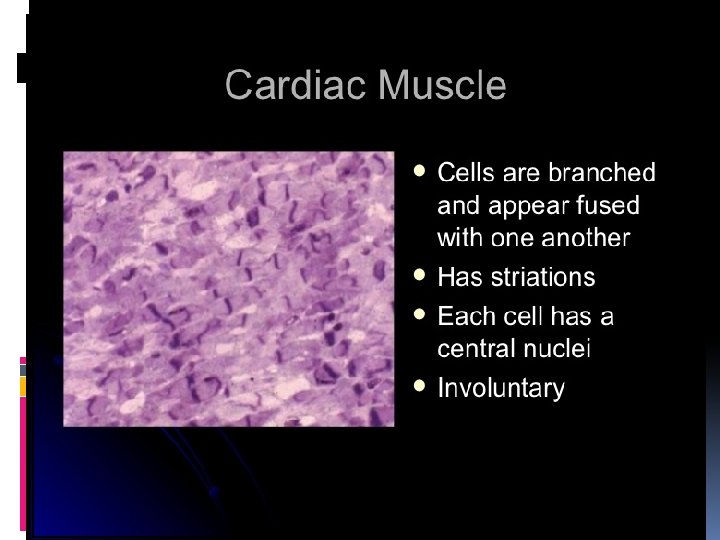
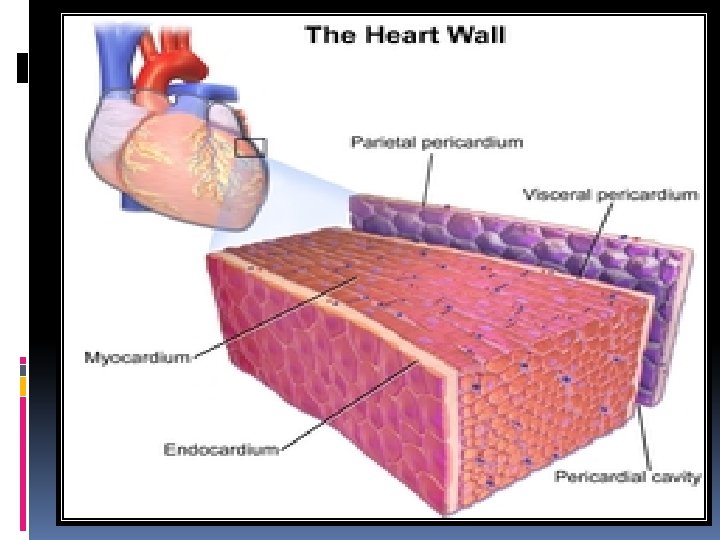

Structure of Cardiac Muscle Cardiac muscle tissue or myocardium forms the bulk of the heart. The heart wall is a threelayered structure with a thick layer of myocardium sandwiched between the inner endocardium and the outer epicardium (also known as the visceral pericardium). The inner endocardium lines the cardiac chambers covers the cardiac valves, and joins with the endothelium that lines the blood vessels that connect to the heart. On the outer aspect of the myocardium is the epicardium which forms part of the pericardium, the sack that surrounds, protects, and lubricates the heart. [1] Within the myocardium, there are several sheets of cardiac muscle cells or cardiomyocytes. The sheets of muscle that wrap around the left ventricle closest to the endocardium are oriented perpendicularly to those closest to the epicardium. When these sheets contract in a coordinated manner they allow the ventricle to squeeze in several directions simultaneously – longitudinally (becoming shorter from apex to base), radially (becoming narrower from side to side), and with a twisting motion (similar to wringing out a damp cloth) to squeeze the maximum possible amount of blood out of the heart with each heartbeat. [2] Contracting heart muscle uses a lot of energy, and therefore requires a constant flow of blood to provide oxygen and nutrients. Blood is brought to the myocardium by the coronary arteries. These originate from the aortic root and lie on the outer or epicardial surface of the heart. Blood is then drained away by the coronary veins into the right atrium

Intercalated discs The cardiac syncytium is a network of cardiomyocytes connected by intercalated discs that enable the rapid transmission of electrical impulses through the network, enabling the syncytium to act in a coordinated contraction of the myocardium. There is an atrial syncytium and a ventricular syncytium that are connected by cardiac connection fibres. [7] Electrical resistance through intercalated discs is very low, thus allowing free diffusion of ions. The ease of ion movement along cardiac muscle fibers axes is such that action potentials are able to travel from one cardiac muscle cell to the next, facing only slight resistance. Each syncytium obeys the all or none law. [8] Intercalated discs are complex adhering structures that connect the single cardiomyocytes to an electrochemical syncytium (in contrast to the skeletal muscle, which becomes a multicellular syncytium during mammalian embryonic development). The discs are responsible mainly force transmission during muscle contraction. Intercalated discs consist of three different types of cell junctions: the actin filament anchoring adherens junctions, the intermediate filament anchoring desmosomes, and gap junctions. They allow action potentials to spread between cardiac cells by permitting the passage of ions between cells, producing depolarization of the heart muscle. However, novel molecular biological and comprehensive studies unequivocally showed that intercalated discs predominantly consist of mixed-type adhering junctions named area composita (pl. areae Compositae) representing an amalgamation of typical desmosomal and fascia adhaerens proteins (in contrast to various epithelia). [9][10][11] The authors discuss the high importance of these findings for the understanding of inherited cardiomyopathies (such as arrhythmogenic right ventricular cardiomyopathy).

Clinical significance Diseases affecting cardiac muscle are of immense clinical significance, and are the leading cause of death in developed nations. [24] The most common condition affecting cardiac muscle is ischaemic heart disease, in which the blood supply to the heart is reduced. In ischaemic heart disease, the coronary arteries become narrowed by atherosclerosis. [25] If these narrowings gradually become severe enough to partially restrict blood flow, the syndrome of angina pectoris may occur. [25] This typically causes chest pain during exertion that is relieved by rest. If a coronary artery suddenly becomes very narrowed or completely blocked, interrupting or severely reducing blood flow through the vessel, a myocardial infarction or heart attack occurs. [26] If the blockage is not relieved promptly by medication, percutaneous coronary intervention, or surgery, then a heart muscle region may become permanently scarred and damaged. [27] Heart muscle can also become damaged despite a normal blood supply. The heart muscle may become inflamed in a condition called myocarditis, [28] most commonly caused by a viral infection[29] but sometimes caused by the body's own immune system. [30] Heart muscle can also be damaged by drugs such as alcohol, long standing high blood pressure or hypertension, or persistent abnormal heart racing. [31] Specific diseases of heart muscle, called cardiomyopathies, can cause heart muscle to become abnormally thick (hypertrophic cardiomyopathy), [32] abnormally large (dilated [33] [34] cardiomyopathy), or abnormally stiff (restrictive cardiomyopathy). Some of these conditions are caused by genetic mutations and can be inherited. [35] Many of these conditions, if severe enough, can damage the heart so much that the pumping function of the heart is reduced. If the heart is no longer able to pump enough blood to meet the body's needs, this is described as heart failure.

Properties of Cardiac Cells The muscle cells of the heart are unique and responsible for the electrical stimulation that leads to proper mechanical function. Myocardial cells have several different electrophysiologic properties: automaticity, excitability, conduc tivity, contractility, rhythmicity, and refractoriness. Knowledge of these distinctive abilities aid in accurate cardiac rhythm interpretation.
- Slides: 25