SelfManagement and Recovery Training Program Approach Principles and




 § § § Social Support 2, 3 Structure Strategies")
 are the most widely")
 SMART Recovery Peer led Facilitator led Free, widely available Free,")
 §")
 Age 18 -72 years")
 Employment Status Unemployed 37%")


 stated the benefit of")
 reported")
 maintained membership")



")











- Slides: 32
Self-Management and Recovery Training: Program Approach, Principles, and Mechanisms for Change Justin R. Watts Ph. D. NCC Assistant Professor University of North Texas Department of Disability and Addiction Rehabilitation Deirdre O’Sullivan Ph. D. CRC Associate Professor The Pennsylvania State University Educational Psychology, Counseling, and Special Education 4 th Annual Recovery Conference
Program Objectives § Overview of peer support groups and mechanisms that support recovery § Discussion of SMART Recovery model § Discuss developing research related to SMART Recovery
Issues Related to Treatment § 22. 7 million individuals needed treatment for drug or alcohol use in 2013 1 § 2. 5 Million (9%) received treatment at a specialty facility § Barriers to Treatment § § § Cost No health insurance Transportation Employer and community stigma Lack of education regarding treatment options
Peer Support Groups § Most widely utilized form of treatment 1 § Supplemental and free option § Those who attend demonstrate higher rates of remission § Reduced involvement, less likelihood of abstinence § Relapse Rate in the US is estimated to be 60% 2, suggesting a need for continued support post-treatment
Peer Support (Mechanisms for Change) § § § Social Support 2, 3 Structure Strategies to cope with cravings Alternative activities Opportunity to establish recovery goals Learning § New behaviors and attitudes which promote sobriety § Self-efficacy
Peer Support Groups § 12 -Step (Alcoholics Anonymous, Narcotics Anonymous) are the most widely utilized models § Consistently, positively, significantly associated with abstinence 4 § The large body of research related to 12 -step has likely overshadowed research on alternative programs 5 § Most of the mechanisms credited to promoting change are not unique to one program § Recovery occurs via many pathways § Individuals are unique with distinct needs, strengths, preferences, goals, culture and backgrounds, including trauma experiences that affect and determine their pathway(s) to recovery 6
12 -Step (Alcoholics Anonymous) SMART Recovery Peer led Facilitator led Free, widely available Free, less widely available, online option Sponsors utilized Does not use sponsor model Utilizes 12 -Steps Utilizes CBT, REBT, MI Disease Model Free will model (self-empowerment) Recovery and membership generally life-long commitment Members are invited to stay involved after gaining independence from addiction Recovery occurs through surrender to higher power, working the 12 -steps Recovery occurs through, building and maintaining motivation coping with urges managing thoughts, feelings and behaviors living a balanced life
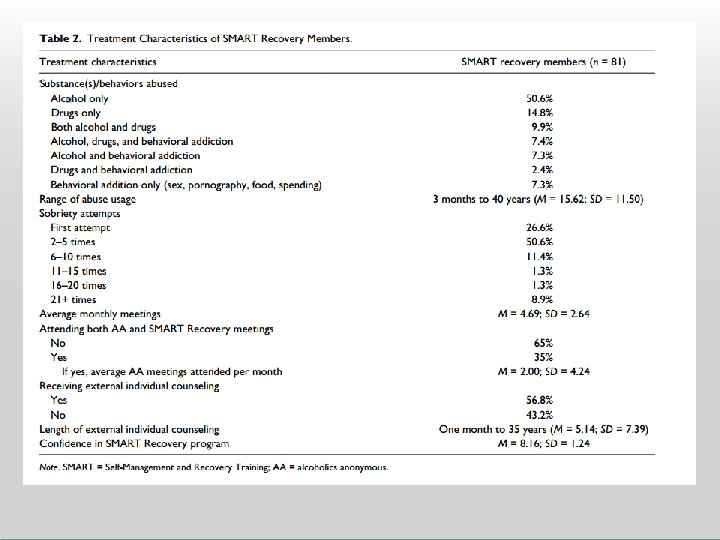
Methods § Participants were self-selected adult participants affiliated with SMART Recovery (facilitators included) § Phase 1 = participants who were affiliated > 3 months § Phase 2 = participants who were affiliated < 3 months § Overall response rates 54% - 74% § Descriptive data was gathered related to health, SUD history, demographics, motivations for attending SMART Recovery meetings
Demographic Characteristics of Established SMART Recovery Members (n = 81) Age 18 -72 years (M=49. 7: SD = 13) Gender Male 66. 7% Female 33. 3% Ethnicity White 90. 1% Hispanic 3. 7% Asian American/PI 2. 5% African American 1. 2% Other 2. 5% Education Bachelor’s 37% Graduate Degree 29. 6% Some College 17. 3% Associate’s 8. 6% High school degree 4. 9% Some high school 2. 5%
Demographic Characteristics of Established SMART Recovery Members (n = 81) Employment Status Unemployed 37% Employed 63% Full Time 36. 7% Part Time 63. 3% Marital Status Married/Partnered 43. 2% Single 34. 6% Divorced 18. 5% Separated 3. 7% Disability Status Without 35% With 65% Psychiatric 51% Physical 40% Both 9%
SMART members’ ranking of the top 3 factors facilitating recovery
Established members’ reasons for attending SMART Recovery 1. Alignment with SMART Recovery program’s philosophy, principles, and format. 2. Difficulties with surrendering to a higher power, and the adoption of a powerlessness identity. 3. Attending both 12 -step meetings and SMART Recovery meetings. 4. Outlier responses
Alignment with SMART Program Philosophy § Thirty-three participants (51. 6%) stated the benefit of connecting with SMART Recovery philosophy, principles, and format as compared to 12 step models § The cognitive-behavioral approach utilized is a foundational appeal for many members § This essence was captured in one participant who stated, “I’ve had good results with [cognitive behavioral therapy]. I sometimes see the rituals of 12 step programs as obstacles” § “What attracted me to SMART were the trained facilitators and the conversation - I feel much more supportive using reason - makes a lot more sense to me then (sic) 12 steps which you have to rely on an addict to help you through”
Difficulty surrendering to a higher power: powerlessness identity § Seventeen participants (26. 6%) reported switching as a result of viewing the low utility for a higher power and an aversion to adopt a powerlessness identity. One participant reported: “I am not a 12 stepper and I don't believe that a “higher power” has any utility for me. If there is a God, it does not intervene in human affairs. Admitting that you are powerless against addiction, and need divine intervention to overcome that addiction is not a constructive mindset”
Attending both 12 step and SMART meetings § Twelve participants (18. 8%) maintained membership in both SMART Recovery and traditional 12 -step communities § One participant reported that he/she is, “Currently doing both. With a ‘home group’ for SMART recovery and a separate one for [Alcoholics Anonymous]” § Another participant reported, “I haven’t switched. I find different perspectives valuable”
SMART Recovery facilitators’ ranking of the top three program goals that help members with their recovery
Rank ordering of recovery goals findings: Overview Top 3 recovery goals for facilitators: • Abstinence • Correcting irrational beliefs/behaviors • Learning to cope with urges Top 3 recovery goals for members: • Changing thoughts and behaviors • Feeling better about self • Connecting past events to current use/abuse
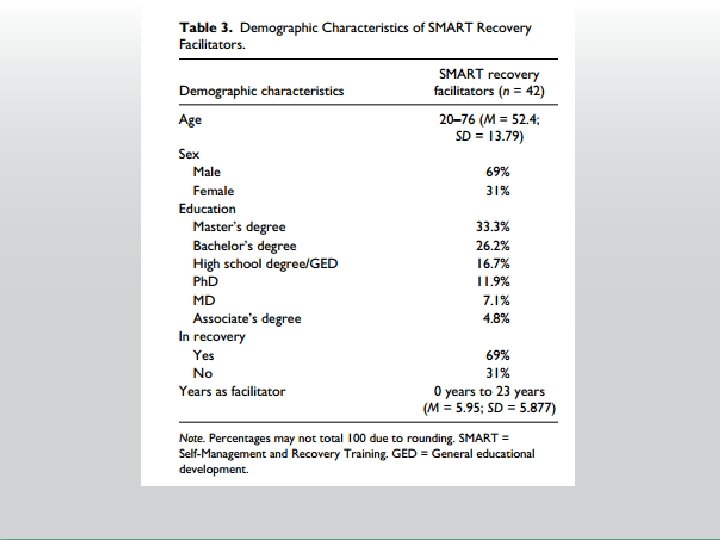
Reasons for becoming a facilitator § Four overarching categories emerged from analyzing the participants’ (n = 38) responses regarding reasons for becoming a SMART Recovery facilitator. § To give back by helping others § Personal benefit for their own recovery § Accidental Facilitator § To provide an alternative recovery group
Facilitator Preparation § 3 overarching categories emerged from analyzing the participants’ (n = 35) responses to what prepared them to be a SMART Recovery facilitator § SMART Recovery training materials and resources § Additional resources outside of SMART Recovery materials § Formal training and education
Refusal Self Efficacy • Strong and reliable predictor of long-term recovery outcomes – – reduced drinking/using more days abstinent longer affiliation with peer support groups transition to stable recovery • Research supports Self Efficacy as a reliable construct that is significantly related to changing health related behaviors including drinking/drug use • SMART Recovery asked that we not explicitly inquire about abstinence; RSE is a known predictor of abstinence • We didn’t want participants to be prompted to feel guilty if lapsed, or if they were taking prescribed pain or mood altering medications due to injury/disability, or psychiatric conditions
Instrument and Variables § Brief Situational Confidence Questionnaire § 10 items rate from 0 to 100 § Respond to emotional and situation triggers, such as feeling depressed, wanting to celebrate with friends, etc. § Strong psychometrics § BSCQ has a cut off score: 45+ indicates lower risk for relapse § New (affiliated < 3 months) vs Established membership (affiliated for 3 months or more) § Low, (less than moderate, frequent attenders)
Results § Established members reported significantly higher refusal self efficacy compared to new members § Established (M = 57. 58) New (M = 39. 20), p =. 006 § New members reported BSCQ scores that are indicative of relapse vulnerability § Frequent attenders reported significantly higher refusal self efficacy compared to infrequent attenders § 10+ meetings/month (M = 83. 2) Fewer than 4 meetings/month (M = 70. 58), p =. 03 § No differences among moderate attenders and other groups, but medium effects indicating meaningfully higher scores as meeting attendance increases
Discussion § Longer affiliation and more frequent attendance improves refusal self efficacy § Essential for those in early recovery § Encourage clients to affiliate with appropriate peer support group for at least 3 months, and attend meetings frequently § Online meetings can supplement in-person meetings (accessibility) § Facilitators can help clients to find other supports as well (counseling, other forms of treatment, role models)
Early Recovery Middle Recovery Late Recovery • Initiation of abstinence – 3 mos (2 -3 years) 7, 8 • Heavy focus on abstinence; highest risk for relapse, instability • 3 months- several years (for some indefinite) • More stability, confidence related to abstinence, reduced focus on abstinence more focus on relapse prevention and reprioritizing work and relationships. Relapse less likely but still possible • Several years • Less emphasis on abstinence and relapse prevention, more attention on individual growth. Focus on work and relationships, individual growth, meaning.
Recovery Capital § Supports which promote recovery over time § Social support, self-efficacy, self-esteem, peer support affiliation, professional treatment, adaptive coping strategies are significantly related to recovery 8, 9, 10 § Recovery capital has been shown to increase quality of life by 22% for those in recovery § Essential to understand the supports and interventions appropriate and necessary at each stage § Presumably, more “recovery capital” translates into higher quality of life, which should result in a reduced risk for relapse § progression to more advanced stages of recovery
Instruments and Variables § Flourishing Scale 11 § self perceived life success and satisfaction on several domains including relationships, daily activities, and optimism about the future. § Strong psychometrics (α =. 85) § BSCQ § Self-Stigma and Mental Illness Scale 12 § Internalized stigma from public stereotypes of having mental illness (substance dependence) § Strong psychometrics (α =. 94) § Relapse history (number of prior relapses) § No prior relapses, few (1 -4), multiple (5+) § Participation (n = 80) in peer support meetings
Findings • Quality of life was significantly correlated with self-concept and abstinence self-efficacy • Significant negative correlation was detected between abstinence self-efficacy and self-stigma (r = -. 34, p <. 01) • Significant positive correlation was detected between abstinence self-efficacy and quality of life (r =. 44, p <. 01). • Significant negative correlation between self-stigma and quality of life (r = -. 52, p <. 01). • Full model with relapse history (step one), abstinence selfefficacy, and self-stigma (step 2) significantly explained variance in quality of life – p <. 001, R 2 =. 363, R 2 adj =. 337. Abstinence self-efficacy and self stigma explained an additional 28. 7% to 31. 3% of the variance in quality of life.
Discussion § Abstinence self-efficacy and self-concept are significantly related to quality of life in expected directions. § Negative significant relationship between self-stigma and abstinence selfefficacy § more internalized negative self-concept is related to a low refusal efficacy § Focus on self-stigma and self-concept is recommended for enhancement of refusal self-efficacy which translates to reduced relapses, better trajectory through the recovery stages • Enhancing self-efficacy is an explicit goal of SMART Recovery prior research shows that affiliation and frequency of meeting attendance increases self-efficacy, this is also the case in other programs • Enhancing self-concept and reducing self stigma are important in recovery as people learn to disavow the public’s perception of someone who struggles with addiction, and adopt a positive self-image • Peer support meetings are not known to focus on self-stigma as a primary meeting goal but perhaps a more deliberate inclusion in meetings would enhance progress through the recovery stages. • Relapse history did explain a small amount of quality of life when entered alone (5%)
Selected References 1 U. S. Department of Health and Human Services Substance Abuse and Mental Health Services Administration (2014). Substance Use and Mental Health Estimates from the 2013 National Survey on Drug Use and Health. www. samhsa. gov 2 National Institute on Drug Abuse (2013). Relapse rates for drug addiction are similar to those of other well-characterized chronic illnesses. Retrieved from https: //www. drugabuse. gov/publications/media-guide/science-drug-abuse-addiction-basics 3 Bond, J. , Kaskutas, L. , & Weisner, C. (2003). The persistent influence of social networks and alcoholics anonymous on abstinence. Journal of Studies on Alcohol, 62, 579 -588 4 Gossop, M. , Stewart, D. , & Marsden, J. (2008). Attendance at Narcotics Anonymous and Alcoholics Anonymous meetings, frequency of attendance and substance use outcomes after residential treatment for drug dependence: A 5 -year follow-up study. Addiction, 103, 119 -125. 5 O’Sullivan, Blum, Watts, Bates (2015) SMART Recovery: Continuing care considerations for rehabilitation counselors. Rehabilitation Counseling Bulletin, 58(4) 6 National Association of Addiction Professionals (2016). Recovery to practice definitions. Retrieved from: http: //www. naadac. org/recovery-definitions 7 National Institute on Drug Abuse. (2012). Principles of drug addiction treatment: A research-based guide (3 rd ed. ). Retrieved from http: //www. drugabuse. gov/publications/principles-drug-addiction-treatment-research-based-guide-third-edition/principles-effective-treatment 8 Laudet, A. , Morgen, K. , White, W. (2006). The role of social supports, spirituality, religiousness, life meaning and affiliation with 12 -step fellowships in quality of life satisfaction among individuals in recovery from alcohol and drug use. Alcoholism Treatment Quarterly, 24(1&2): 33– 74. 9 Kelly, J. F. , Magill, M. , & Stout, R. L. (2009). How do people recover from alcohol dependence? A systematic review of the research on mechanisms of behavior change in Alcoholics Anonymous. Addiction Research & Theory, 17, 236 -259. 10 Fiorentine, R. , Anglin, M. D. (1996). More is better: counseling participation and the effectiveness of outpatient drug treatment. The Journal of Substance Abuse Treatment, 13, 341– 348. 11 Diener, E. , Wirtz, D. , Tov, W. , Kim-Prieto, C. , Choi, D. , Oishi, S. , & Biswas-Diener, R. (2010). New well-being measures: Short scales to assess quality of life and positive and negative feelings. Social Indicators Research, 97(2), 143 -156. 12 Corrigan, P. W. , Watson, A. C. , & Barr, L. (2006). The self-stigma of mental illness: Implications for self-esteem and self-efficacy. Journal of Social and Clinical Psychology, 25(8), 875 -884.
Thank You. Justin R. Watts Ph. D. NCC Justin. watts@unt. edu