Seizures Endocrine Emergencies Dr Colin Begg Consultant Paediatric

Seizures & Endocrine Emergencies Dr Colin Begg Consultant Paediatric Intensivist Royal Hospital for Children, Glasgow

Aims • Seizures —diagnosis & treatment in the PICU — 2017 ILAE re-classification • Encocrine Emergencies —overview —common PICU presentations

Childhood Epilepsy Incidence • Is falling. Cohort study: — 1% of children born between 1994 -1996 had either • repeat prescription for anti-epilepsy drugs • clinical diagnosis • had symptoms of epilepsy by five years of age — This fell to 0. 53% for children born 2003 – 2005 • decline of 47% • 33% over the same period, if only repeat AED Rx were considered. Meeraus WH, Petersen I, Chin RF, et al. Childhood epilepsy recorded in primary care in the UK. Archives of Disease in Childhood. Published online January 23 2013

Childhood Epilepsy Incidence • Reasons unclear — improved diagnostic accuracy — changes in treatment practices • milder forms of epilepsy are no longer treated — 15 year reduction in TBI — ? Men C & pneumococcal vaccine Meeraus WH, Petersen I, Chin RF, et al. Childhood epilepsy recorded in primary care in the UK. Archives of Disease in Childhood. Published online January 23 2013

Seizures in Children • Febrile convulsions very common • Incidence — 2% - 5% US & Western Europe — 6% - 9% Japan — 14% India & Guam — background prevalence risk 1 in 30 • rises to 1 in 5 where one sibling is affected • 1 in 3 if both parents & a previous child have had febrile seizures. • Mutations in STX 1 B, encoding a presynaptic protein, cause fever-associated epilepsy Maybe associated with polymorphisms in STX 1 B channel syndromes Julian Schubert, Aleksandra Siekierska, Holger Lerche Nature Genetics volume 46, pages 1327– 1332 (2014) Febrile seizures Patel Nikhil, Ram Dipak, Swiderska Nina, Mewasingh Leena D, Newton Richard W, Offringa Martin et al. BMJ 2015; 351 : h 4240

Febrile Convulsions • “a seizure occurring in childhood after one month of age associated with a febrile illness not caused by an infection of the central nervous system, without previous neonatal seizures or a previous unprovoked seizure, and not meeting the criteria for other acute symptomatic seizures. ” — ILAE 1993

Simple vs. Complex Febrile Convulsions • https: //www. bmj. com/content/351/bmj. h 4240

Risk factors for recurrent febrile seizures • Age at onset under 18 months • History of febrile seizure in a first degree relative • Relatively low grade of fever associated with seizure (<39°C) • Shorter duration of fever before seizure (<1 hour) • Multiple seizures during the same febrile illness • Day nursery attendance

Red flags for meningitis • History of irritability, decreased feeding, or lethargy • Complex febrile seizures • Any physical signs of meningitis or encephalitis (bulging fontanelle, neck stiffness, photophobia, focal neurological signs) • Prolonged postictal altered consciousness or neurological deficit (>1 hour) • Drowsiness with limited response to social cues (lasting >1 hour) • Recent or current treatment with antibiotics • Incomplete immunisation in children aged 6 -18 months against Haemophilus influenzae b and. Streptococcus pneumoniae • In children <2 years old, symptoms and signs of meningeal irritation such as meningism and photophobia may be absent in meningitis and further assessment by a senior paediatrician (or general practitioner with suitable training, depending on the setting) may be required. If there is genuine uncertainty, a lumbar puncture should be performed but postponed if there is reduced consciousness

Management

Refractory seizures • Check Phenytoin and/or Phenobarbitone levels • Consider cause — Encephalitis — ADEM — FIRES • Urgent neurology consultation & EEG — Steroids? Plasmapheresis? Ketogenic diet — Anakinra or other novel AED • Commence propofol or thiopentone infusion — no difference either way • Prabhakar H, Kalaivani M. Propofol versus thiopental sodium for the treatment of refractory status epilepticus. Cochrane Database of Systematic Reviews 2017, Issue 2. Art. No. : CD 009202

Monitoring modalities • Gold standard — Continuous v. EEG with neurology review telemetry • NIRS can be useful • a. EEG/CFM – sceptics & believers. Evidence limited

The 2017 ILAE Classification of Seizures • In 2017, the International League Against Epilepsy released a new classification of seizure types, largely based upon the existing classification formulated in 1981. • Main differences: 1. Specific listing of certain new focal seizure types that may previously only have been in the generalized category 2. Use of awareness as a surrogate for consciousness 3. Emphasis on classifying focal seizures by first clinical manifestation (except for altered awareness) 4. A few new generalizedseizure types 5. Ability to classify some seizures when onset is unknown 6. Renaming of certain terms to improve clarity of meaning. Fisher et al. Instruction manual for the ILAE 2017 operational classification of seizure types. Epilepsia doi: 10. 1111/epi. 13671.

The Reason “Words, words, I’m so sick of words!” Eliza Doolittle, My Fair Lady

ILAE 2017 Classification of Seizure Types Basic Version 1 Focal Onset Aware Impaired Awareness Motor Non-Motor Generalised Onset Motor Tonic-clonic Other motor Non-Motor (Absence) focal to bilateral tonic-clonic Unknown Onset Motor Tonic-clonic Other motor Non-Motor Unclassified 2 1 Definitions, other seizure types and descriptors are listed in the accompanying paper & glossary of terms 2 Due to inadequate information or inability to place in other categories From Fisher et al. Instruction manual for the ILAE 2017 operational classification of seizure types. Epilepsia doi: 10. 1111/epi. 13671

ILAE 2017 Classification of Seizure Types Expanded Version 1 Focal Onset Aware Impaired Awareness Motor Onset automatisms atonic 2 clonic epileptic spasms 2 hyperkinetic myoclonic tonic Non-Motor Onset autonomic behavior arrest cognitive emotional sensory focal to bilateral tonic-clonic Generalized Onset Unknown Onset Motor tonic-clonic tonic myoclonic-tonic-clonic myoclonic-atonic epileptic spasms 2 Motor tonic-clonic epileptic spasms Non-Motor behavior arrest Non-Motor (absence) typical atypical myoclonic eyelid myoclonia Unclassified 3 1 Definitions, other seizure types and descriptors are listed in the accompanying paper and glossary of terms. 2 These could be focal or generalized, with or without alteration of awareness 3 Due to inadequate information or inability to place in other categories From Fisher et al. Instruction manual for the ILAE 2017 operational classification of seizure types. Epilepsia doi: 10. 1111/epi. 13671
 Simple (no loss")
International classification of Seizures 1981 Partial Seizures (start in one place) Simple (no loss of consciousness of memory) Sensory Motor Sensory-Motor Psychic (abnormal thoughts or perceptions) Autonomic (heat, nausea, flushing, etc. ) Complex (consciousness or memory impaired) With or without aura (warning) With or without automatisms Secondarily generalized Generalized Seizures (apparent start over wide areas of brain) Absence (petit mal) Dreifuss et al. Proposal for revised Tonic-clonic (grand mal) clinical and electroencephalographic classification of epileptic seizures. Atonic (drop seizures) From the Commission on Myoclonic Classification and Terminology of the International League Against Epilepsy. Other Epilepsia. 1981; 22: 489 -501. Unclassifiable seizures

Motivation for Revision • Some seizure types, for example tonic seizures or epileptic spasms, can have either a focal or generalized onset. • Lack of knowledge about the onset makes a seizure unclassifiable and difficult to discuss with the 1981 system. • Retrospective seizure descriptions often do not specify a level of consciousness, and altered consciousness, while central to many seizures, is a confusing concept. • Some terms in current use do not have high levels of community acceptance or public understanding, such as “psychic, ” “partial, ” “simple partial, ” “complex partial”, and “dyscognitive. ” • Some important seizure types are not included.

Possible Seizure Classifications could be Based On: Pathophysiology Anatomy Networks Practical, by: Modify Existing But this is currently impossible with our limited understanding Temporal Frontal Parietal Occipital Diencephalic Brainstem Neocortical Limbic Thalamo-Cortical Brainstem AED response Surgical target Disabling EEG pattern Many others 1981 ILAE System 2010 ILAE update • In the absence of fundamental knowledge, ILAE chose to extend the existing classification • The is an operational (practical) system, not a true scientific classification • Others might devise special operational classifications for specific use, e. g. , neonatal, ICU • This classification is predominantly for clinicians
 •")
How Do Clinicians Classify Seizures? • Elicit symptoms and signs of event (semiology) • Look for familiar patterns in symptoms and signs • Sometimes use ancillary data, e. g. , EEG, MRI, genes, antibodies, etc. one-to many Symptoms + Signs Seizure Type many-to-one examples automatisms focal impaired awareness seizure absence seizure automatisms autonomic focal impaired awareness seizure

Key Seizure Signs and Symptoms? Symptoms Medical Term automatic behaviors automatisms emotions or appearance of emotions extension or flexion postures tonic flushing/sweating/piloerection autonomic jerking arrhythmically myoclonus jerking rhythmically clonus language or thinking problems, deja vu cognitive lid jerks eyelid myoclonia limp atonic numb/tingling, sounds, smells, tastes visions, sensations vertigo pausing, freezing, activity arrest behavior arrest thrashing/pedaling hyperkinetic trunk flexion spasm

The 2017 Changes • Allow some seizures to be either focal or generalized onset • Classify seizures of unknown onset • Clarify “impairment of consciousness” • Include a few previously unclassified types • Update word usage for greater public clarity • Validate use of supportive information, e. g. EEG • Conform with ICD 11 and 12 • Update the 2001 glossary of seizure terms • Standardize common descriptors to describe seizures • Map old to new terms

The 2017 Changes • Allow some seizures to be either focal or generalized onset • Classify seizures of unknown onset • Clarify “impairment of consciousness” • Include a few previously unclassified types • Update word usage for greater public clarity • Validate use of supportive information, e. g. EEG • Conform with ICD 11 and 12 • Update the 2001 glossary of seizure terms • Standardize common descriptors to describe seizures • Map old to new terms

Some Seizure Onsets can be Focal or Generalized Focal Onset Generalized Onset atonic clonic epileptic spasms myoclonic tonic-clonic

The 2017 Changes • Allow some seizures to be either focal or generalized onset • Classify seizures of unknown onset • Clarify “impairment of consciousness” • Include a few previously unclassified types • Update word usage for greater public clarity • Validate use of supportive information, e. g. EEG • Conform with ICD 11 and 12 • Update the 2001 glossary of seizure terms • Standardize common descriptors to describe seizures • Map old to new terms

Seizures of Unknown Onset Hypothetical case: You hear a noise and enter the video. EEG room to find the patient in bed, grunting, eyes rolled up, all limbs stiff, then rhythmically jerking for a minute. He was off-camera at the start. What seizure type is this? Some seizure types are worth describing even if onset is unknown: • • • tonic-clonic epileptic spasms behaviour arrest

The 2017 Changes • Allow some seizures to be either focal or generalized onset • Classify seizures of unknown onset • Clarify “impairment of consciousness” • Include a few previously unclassified types • Update word usage for greater public clarity • Validate use of supportive information, e. g. EEG • Conform with ICD 11 and 12 • Update the 2001 glossary of seizure terms • Standardize common descriptors to describe seizures • Map old to new terms

Key Role of Impaired Consciousness Among many possible behaviors during a seizure, impairment of consciousness has always had a key role in classifying the seizure, because of practical importance for: • • Driving Safety during seizures Employability Interference with schooling and learning
 of Consciousness Two types of seizures with loss of consciousness: How")
Loss (or Impairment) of Consciousness Two types of seizures with loss of consciousness: How well does the public understand LOC during a complex partial seizure?
 of Consciousness Elements of consciousness • • Awareness of ongoing activities")
Loss (or Impairment) of Consciousness Elements of consciousness • • Awareness of ongoing activities Memory for time during the event Responsiveness to verbal or nonverbal stimuli Sense of self as being distinct from others Which would be the best surrogate marker ? • The 2017 Classification chooses awareness • Consciousness remains in the classification but “awareness” is in the seizure name • In several languages, these words are the same • Awareness is not used to classify generalized onset seizures

The 2017 Changes • Allow some seizures to be either focal or generalized onset • Classify seizures of unknown onset • Clarify “impairment of consciousness” • Include a few previously unclassified types • Update word usage for greater public clarity • Validate use of supportive information, e. g. EEG • Conform with ICD 11 and 12 • Update the 2001 glossary of seizure terms • Standardize common descriptors to describe seizures • Map old to new terms
 clonic")
New Seizure Types New Focal Seizures Motor Non-Motor behavior atonic arrest automatisms (autonomic) clonic epileptic spasms(cognitive) emotional hyperkinetic (sensory) myoclonic tonic New generalized seizures • absence with eyelid myoclonia • epileptic spasms (infantile spasms) • myoclonic-atonic (e. g. , Doose) • myoclonic-tonic-clonic (e. g. , JME) New combined seizures (focal to bilateral tonic-clonic) (parentheses) indicates prior existence, but renaming

The 2017 Changes • Allow some seizures to be either focal or generalized onset • Classify seizures of unknown onset • Clarify “impairment of consciousness” • Include a few previously unclassified types • Update word usage for greater public clarity • Validate use of supportive information, e. g. EEG • Conform with ICD 11 and 12 • Update the 2001 glossary of seizure terms • Standardize common descriptors to describe seizures • Map old to new terms
 Impaired awareness")
Wording Changes OLD TERM NEW TERM Unconscious (still used, not in name) Impaired awareness (surrogate) Partial Focal Simple partial Focal aware Complex partial Focal impaired awareness Dyscognitive (word discontinued) Focal impaired awareness Psychic Cognitive Secondarily generalized tonic-clonic Focal to bilateral tonic-clonic Arrest, freeze, pause, interruption Behavior arrest

The Elements of Change • Allow some seizures to be either focal or generalized onset • Classify seizures of unknown onset • Clarify “impairment of consciousness” • Include a few previously unclassified types • Update word usage for greater public clarity • Validate use of supportive information, e. g. EEG • Conform with ICD 11 and 12 • Update the 2001 glossary of seizure terms • Standardize common descriptors to describe seizures • Map old to new terms

The 2017 Changes • Allow some seizures to be either focal or generalized onset • Classify seizures of unknown onset • Clarify “impairment of consciousness” • Include a few previously unclassified types • Update word usage for greater public clarity • Validate use of supportive information, e. g. EEG • Conform with ICD 11 and 12 • Update the 2001 glossary of seizure terms • Standardize common descriptors to describe seizures • Map old to new terms

Supportive Information Seizures are usually classified by symptoms and signs But supportive information may be helpful, when available: • • • Videos brought in by family EEG patterns Lesions detected by neuroimaging Laboratory results such as detection of anti-neuronal antibodies Gene mutations Diagnosis of an epilepsy syndrome diagnosis

The 2017 Changes • Allow some seizures to be either focal or generalized onset • Classify seizures of unknown onset • Clarify “impairment of consciousness” • Include a few previously unclassified types • Update word usage for greater public clarity • Validate use of supportive information, e. g. EEG • Conform with ICD 11 and 12 • Update the 2001 glossary of seizure terms • Standardize common descriptors to describe seizures • Map old to new terms

ICD 9, 10, 11, 12 • ICD 9 & 10 are in use now with old terminology: petit mal, grand mal • ICD 11 does not name seizure types, but ILAE syndromes & aetiologies • ICD 12 should conform to the new ILAE seizure type classification

The 2017 Changes • Allow some seizures to be either focal or generalized onset • Classify seizures of unknown onset • Clarify “impairment of consciousness” • Include a few previously unclassified types • Update word usage for greater public clarity • Validate use of supportive information, e. g. EEG • Conform with ICD 11 and 12 • Update the 2001 glossary of seizure terms • Standardize common descriptors to describe seizures • Map old to new terms

Glossary: Full list in Epilepsia Paper WORD DEFINITION SOURCE a sudden onset, interruption of ongoing activities, a blank stare, possibly a brief up- ward deviation of the eyes. Usually the patient will be unresponsive when spoken to. Duration is a few seconds to half a minute with very rapid recovery. Although not always available, an EEG would show generalized epileptiform discharges during the event. An absence seizure is by definition a seizure of generalized onset. The word is not synonymous with a blank stare, which also can be encountered with focal onset seizures. Adapted from 11 absence, atypical an absence seizure with changes in tone that are more pronounced Adapted from Dreifuss 1 arrest atonic see behavioral arrest automatism a more or less coordinated motor activity usually occurring when cognition is impaired and for which the subject is usually (but not always) amnesic afterward. This often resembles a voluntary movement and may consist of an inappropriate continuation of preictal motor activity. absence, typical than in typical absence or the onset and/or cessation is not abrupt, often associated with slow, irregular, generalized spike-wave activity sudden loss or diminution of muscle tone without apparent preceding myoclonic or tonic event lasting ~1 to 2 s, involving head, trunk, jaw, or limb musculature. new 11 11

The 2017 Changes • Allow some seizures to be either focal or generalized onset • Classify seizures of unknown onset • Clarify “impairment of consciousness” • Include a few previously unclassified types • Update word usage for greater public clarity • Validate use of supportive information, e. g. EEG • Conform with ICD 11 and 12 • Update the 2001 glossary of seizure terms • Standardize common descriptors to describe seizures • Map old to new terms

Common Descriptors of other symptoms and signs during seizures. These are not seizure types, just suggested descriptive words. A free text description is also highly encouraged.

The 2017 Changes • Allow some seizures to be either focal or generalized onset • Classify seizures of unknown onset • Clarify “impairment of consciousness” • Include a few previously unclassified types • Update word usage for greater public clarity • Validate use of supportive information, e. g. EEG • Conform with ICD 11 and 12 • Update the 2001 glossary of seizure terms • Standardize common descriptors to describe seizures • Map old to new terms

Examples of Mapping Old to New Terms Full List in Epilepsia paper
 Onset: Decide whether seizure onset is focal")
Rules for Classifying Seizures (1 of 2) Onset: Decide whether seizure onset is focal or generalized, using an 80% confidence level. Awareness: For focal seizures, decide whether to classify by degree of awareness or to omit awareness as a classifier. Impaired awareness at any point: A focal seizure is a focal impaired awareness seizure if awareness is impaired at any point during the seizure. Onset predominates: Classify a focal seizure by its first prominent sign or symptom. Do not count transient behavior arrest. Behavior arrest: A focal behavior arrest seizure shows arrest of behavior as the prominent feature of the entire seizure. Motor/Non-motor: A focal aware or impaired awareness seizure maybe further sub-classified by motor or non-motor characteristics. Alternatively, a focal seizure can be characterized by motor or non-motor characteristics, without specifying level of awareness. Example, a focal tonic seizure.
 Optional terms: Terms such as motor or")
Rules for Classifying Seizures (2 of 2) Optional terms: Terms such as motor or non-motor may be omitted when the seizure type is otherwise unambiguous. Additional descriptors: It is encouraged to add descriptions of other signs and symptoms, suggested descriptors or free text. These do not alter the seizure type. Example: focal emotional seizure with tonic right arm activity and hyperventilation. Bilateral vs. generalized: Use the term “bilateral” for tonicclonic seizures that propagate to both hemispheres and “generalized” for seizures that apparently originate simultaneously in both. Atypical absence: Absence is atypical if it has slow onset or offset, marked changes in tone or EEG spikewaves at less than 3 per second. Clonic vs. myoclonic: Clonic refers to sustain rhythmical jerking and myoclonic to a regular unsustained jerking. Eyelid myoclonia: Absence with eyelid myoclonia refers to forced upward jerking of the eyelids during an absence seizure.

The Net Effect The net effect of updating the Classification of Seizures should be the following: 1. Render the choice of a seizure type easier for seizures that did not fit into any prior categories; 2. Clarify what is meant when a seizure is said to be of a particular type; 3. Provide more transparency of terminology to the nonmedical community (and non-Neurologists!)

Examples 1. A woman awakens to find her husband having a seizure in bed. The onset is not witnessed, but she is able to describe bilateral stiffening followed by bilateral shaking. EEG and MRI are normal.

Examples Old = unclassified New = unknown onset tonic-clonic 1. A woman awakens to find her husband having a seizure in bed. The onset is not witnessed, but she is able to describe bilateral stiffening followed by bilateral shaking. EEG and MRI are normal. This seizure is classified as onset unknown tonic-clonic. There is no supplementary information to determine if the onset was focal or generalized. In the old classification, this seizure would have been unclassifiable.

Examples 2. In an alternate scenario of case #1, the EEG shows a clear right parietal slow wave focus. The MRI shows a right parietal region of cortical dysplasia.

Examples Old = partial onset, secondarily generalized seizure New = focal to bilateral tonic-clonic seizure 2. In an alternate scenario of case #1, the EEG shows a clear right parietal slow wave focus. The MRI shows a right parietal region of cortical dysplasia. In this circumstance, the seizure can be classified as focal to bilateral tonic-clonic, despite the lack of an observed onset, because a focal etiology has been identified, and the overwhelming likelihood is that the seizure had a focal onset. The old classification would have classified this seizure as partial onset, secondarily generalized seizure.

Examples 3. A child is diagnosed with Lennox-Gastaut syndrome of unknown etiology. EEG shows runs of slow spike-wave. Seizure types include absence and others.

Examples Old = atypical absence seizures New = atypical absence seizures 3. A child is diagnosed with Lennox-Gastaut syndrome of unknown etiology. EEG shows runs of slow spike-wave. Seizure types with this child include absence, tonic, and focal motor seizures. In this case, the absence seizures are classified as atypical absence (the word “generalized” may be assumed) due to the EEG pattern and underlying syndrome. The absence seizures would have had the same classification in the old system.

Examples 4. The same child as in #3 has seizures with stiffening of the right arm and leg, during which responsiveness and awareness are retained.

Examples Old = tonic seizures New = focal aware tonic seizures 4. The same child as in #3 has seizures with stiffening of the right arm and leg, during which responsiveness and awareness are retained. This seizure is a focal aware tonic seizures (the word “motor” can be assumed). In the old system, the seizures would have been called tonic seizures, with a perhaps incorrect assumption of generalized onset.

Examples 5: A 25 year old woman describes seizures beginning with 30 seconds of an intense feeling that “familiar music is playing. ” She can hear other people talking, but afterwards realizes that she could not determine what they were saying. After an episode, she is mildly confused, and has to “reorient herself. ”

Examples Old = complex partial seizures New = focal seizures with impaired awareness 5: A 25 year old woman describes seizures beginning with 30 seconds of an intense feeling that “familiar music is playing. ” She can hear other people talking, but afterwards realizes that she could not determine what they were saying. After an episode, she is mildly confused, and has to “reorient herself. ” The seizures would be classified as focal seizures with impaired awareness. Even though the patient is able to interact with her environment, she cannot interpret her environment, and is mildly confused.

Examples 6. A 22 year-old man has seizures during which he remains fully aware, with the “hair on my arms standing on edge” and a feeling of being flushed.

Examples Old = simple partial autonomic seizures New = focal aware autonomic seizures 6. A 22 year-old man has seizures during which he remains fully aware, with the “hair on my arms standing on edge” and a feeling of being flushed. These are classified as focal aware non-motor autonomic, or more succinctly focal aware autonomic. The old classification would have called them simple partial autonomic seizures.
 has seizures with")
Examples 7. A 4 year-old boy with myoclonic-atonic epilepsy (Doose syndrome) has seizures with a few arm jerks, then a limp drop to the ground.

Examples Old = myoclonic astatic seizures New = myoclonic-atonic seizures 7. A 4 year-old boy with myoclonic-atonic epilepsy (Doose syndrome) has seizures with a few arm jerks, then a limp drop to the ground. These are now classified as myoclonic-atonic seizures (the word “generalized” may be assumed). The old classification would have called these unclassified or unofficially, myoclonic-astatic seizures.

Examples 8. A 35 year-old man with juvenile myoclonic epilepsy has seizures beginning with a few bilateral arm jerks, followed by stiffening of all limbs and then rhythmic jerking of all limbs.

Examples Old = myoclonic seizures followed by a tonic-clonic seizure New = myoclonic-tonic-clonic seizures 8. A 35 year-old man with juvenile myoclonic epilepsy has seizures beginning with a few regularly-spaced jerks, followed by stiffening of all limbs and then rhythmic jerking of all limbs. This would be classified as generalized myoclonic-tonic-clonic seizures. No corresponding single seizure type existed in the old classification, but they might have been called myoclonic seizures followed by a tonic-clonic seizure.

Examples 9. A 14 -month old girl has sudden flexion of both arms with head flexing forward for about 2 seconds. These seizures repeat in clusters. EEG shows hypsarrhythmia with bilateral spikes, most prominent over the left parietal region. MRI shows a left parietal dysplasia.
 New = focal epileptic spasms 9.")
Examples Old = infantile spasms (focality not specified) New = focal epileptic spasms 9. A 14 -month old girl has sudden flexion of both arms with head flexing forward for about 2 seconds. These seizures repeat in clusters. EEG shows hypsarrhythmia with bilateral spikes, most prominent over the left parietal region. MRI shows a left parietal dysplasia. Because of the ancillary information, the seizure type would be considered to be focal epileptic spasms (the term “motor” can be assumed). The previous classification would have called them infantile spasms, with information on focality not included.

Examples 10. A 75 year-old man reports an internal sense of body trembling. No other information is available.

Endocrine Emergencies C Begg

Aims • Review anatomy/physiology of endocrine system • Recognise and manage common endocrine emergencies • Be aware of common pitfalls • Gain an understanding of the controversies of endocrine management in PICU

Common issues • Hypoglycaemia • Diabetic Ketoacidosis • Adrenal Insufficiency • Thyroid function and ICU

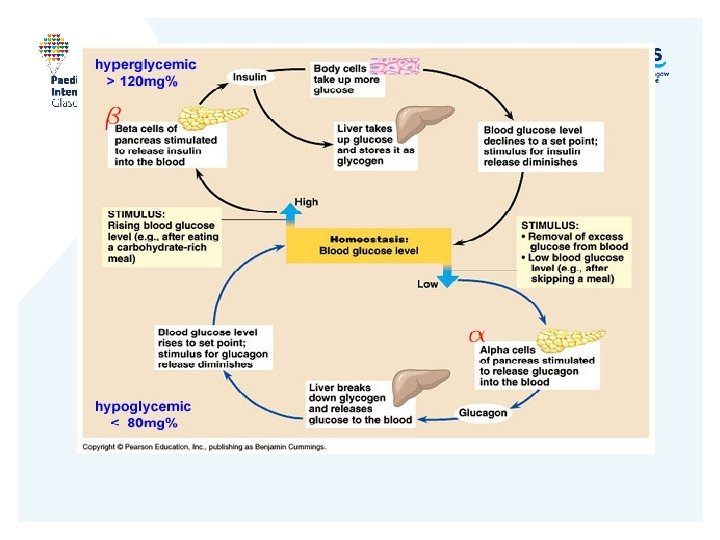
Glucose homeostasis Eat – increased blood glucose. Pancreas secretes insulin. Insulin switches off gluconeogenesis /glycogenolysis and encourages uptake glucose to peripheral cells. Also encourages protein and fat uptake and storage. Glucagon secretion reduced Counteregulatory hormones (GH, glucagon, cortisol, catecholamines)
 Neonates limited glycogen/fat. Delayed")
Hypoglycaemia • Definition: Child <3. 5 Neonate <2. 6 (controversial) Neonates limited glycogen/fat. Delayed maturation hepatic enzymes Poor intake Worry if symptomatic

• Most babes – occasional low sugar normal • Concern – low sugar, recurrent, difficulty correcting, older Rule of thumb: Low sugars – not good for you! Act fast • Symptomatic and convulsions –poor prognosis . Kovisto 1972 - Dev Med Child • <2. 6 on 5 consecutive days –CP Lucas BMJ 1988; 297: 1304 -1308 • <2. 5 symptomatic -39% MRI changes –normal development at 9 months Kinnala Paediatrics 1999

Treatment • Feed if able • Glucose – 2 -5 ml/kg of 10% dextrose • Try and avoid recurrent boluses – just get rebound • Recheck BM regularly – ensure improves and avoid further hypoglycaemic episodes • Provide sufficient dextrose – 10%, 12. 5%, 15% as necessary (PIC line may be required)

Differential • Decrease in glucose availability (Fasting, diarrhoea, glycogen storage disease, ketotic hypoglycaemia, liver disease) • Increase in glucose utilisation (Hyperinsulinism, neisidoblastosis, Beckwith-Wiedeman, ethanol, sepsis, adrenal insufficiency)

Hypoglycaemia Investigations Blood • Insulin • C-peptide • Growth Hormone • Cortisol • TFT • FFA • Bhydroxybutyrate Urine • Reducing substances • Ketones • Organic Acids

Too much insulin • Macrosomia • Persistent and severe non-ketotic hypoglycaemia • High insulin levels • High glucose infusion(8 mg/kg min +) ? ? Greater neurologic injury – no ketones or glucose 2. 5% mortality 52% severe neuro disability Diazoxide/octreotide +/- near-total pancreatectomy

Metabolic disorders causing hypo • Fatty acid disorders Non-ketotic hypoglycaemia and high FFA • Glycogen Storage Disorders Hepatosplenomegaly, typical facies • Galactosaemia Jaundice, hypoglycaemic, G-ve sepsis. +ve reducing substances, Gal-1 -put

Ketotic Hypoglycaemia • Typically age 1 - 5 • Recurrent low glucose when ill • Ketonuria, ketonemia, low insulin • Hypoalinaemia, low lean muscle mass • ? extreme response to fasting • Improves as gets older

Diabetes • Insulinopenic • Glucose load – not taken up by tissues • Glucagon not switched off so leads to glycogenolysis, lipolysis, ketogenesis • Fat oxidation primary energy source

Diabetic Ketoacidosis • Mortality • Children with IDDM 3 x more likely to die in childhood than general population. Death - Cerebral Oedema – unpredictable - Hypokalaemia - Aspiration

Insulin Deficiency Glucose uptake Lipolysis Proteolysis Glycerol Free Fatty Acids Amino Acids Hyperglycemia Osmotic diuresis Gluconeogenesis Glycogenolysis Ketogenesis Dehydration Acidosis

Definition • Glucose > 11 mmol/l • p. H <7. 3 • Bicarbonate < 15 mmol/l • Metabolic acidosis – Increased anion gap • Glucose and ketones in urine • Blood ketone usually over 3. 0 mmol/l (most ketone tests don’t measure B-hydroxybutyrate - underestimate)

Cerebral Oedema • CT scan – all have some oedema -? clinical relevance • Who? • Young • New IDDM • Long history of symptoms – severity of dehydration • 4 -12 hours 25% mortality Low p. CO 2 , high Na, high urea Bicarbonate therapy

Guidelines • Frequent reassessment key to management • Same person • Shift system – clear documentation

• Restore metabolic haemostasis • Minimise risks of complications

Variation in the Management of Pediatric Diabetic Ketoacidosis by Specialty Training NS Glaser et al Archives Pediatric Adolescent Medicine 1997 151 1125 Conclusions: Substantial differences exist in the management of pediatric DKA among physicians. These obscure our ability to evaluate treatment, and highlight the need for further studies comparing the outcome of different treatment strategies.
 • B – 100% Oxygen •")
Emergency Management • A – reduced consciousness/vomiting (NG) • B – 100% Oxygen • C – IV access – ECG monitoring (avoid CVC if possible) • If shocked 10 ml/kg 0. 9% saline • Reassess (BPSED suggest max 30 ml/kg) Local 20 ml/kg
 3% - only just clinically")
Clinical assessment • Assess degree of dehydration (BSPED 2009) 3% - only just clinically detectable 5% - dry mucous membranes, reduced skin turgor 8% - poor perfusion/ thready pulse Over-estimation is dangerous. If available use recent clinic weight

Conscious level • Hourly GCS – even if fully awake initially. • Coma – HDU/PICU • Cerebral oedema management • Detecting oedema- bradycardia/ hypertension, pupils, headache, irritability • Increased lethargy in face of biochemical improvement.

Criteria for PICU/HDU admission • p. H <7. 1 with marked hyperventilation • Severe dehydration • Coma • Young <2

Observations • Fluid balance – urine output • Blood glucose – hourly • Blood ketones – 1 -2 hourly • BP and obs • Twice daily weight • Headache, slow pulse, change in behaviour/ sleepy • 2 hourly UE then 4 hourly
")
Fluid Management • Requirement = Maintenance + Deficit – resus fluid. • Deficit (litres) = % dehydration x body weight (kg) • Give fluids over 48 hours

• 0. 9% saline + 20 mmol KCL per 500 ml initially ( 6 hours local guidelines/ 12 hours BSPED) • <14 mmol/l add glucose to the above • After 12 hours if stable 0. 45%saline/ 5%dextrose • If Na falls stick with 0. 9% saline

Fluid controversy • Maintenance and deficit • Hypertonic dehydration and electrolyte disorder Prolonged and cautious replacement

Mechanisms in DKA • Hyperglycaemia leads to glycosuria and osmotic diuresis. • Kidney has low threshold for ketones therefore excreted with a cation • Relative acute dehydration with large Na loss – intravascularly dry. • If occurs more slowly –wide variation in fluid and electrolyte deficiencies.
")
Sodium • Hyponatraemia — Osmolar shift water ICF ECF (osmotic effect of high glucose) — Natriuresis — Hyperlipidaemia — Ketone salt loss in urine — ADH • Hypernatraemia (if Na high with high glucose assume reasonable amount of dehydration) • Normal

Corrected Na Levels - Controversial • ? Marker for oedema • Serum sodium should rise as blood glucose falls. • Low coma score and Corrected Na not rising assume – oedema • Corrected Na = Plasma Na + 0. 4(glucose - 5. 5) • Increase in Corr Na >5 mmol in 4 -8 hrs = too much fluid loss = increase rate by 25% • Decrease in corr Na by 5 mmol in 4 -8 hrs = too much fluid in = decrease rate by 25%

Potassium • Give unless anuric • KCL deficient – vomit/diuresis • Acidosis K+ leaves cells • Renal impairment • K > 6 • Correction of acidosis and admin of insulin will lead to rapid fall. • If KCL very low –think about holding off insulin 30% at presentation

Insulin • ? Early start -leads to oedema • Start after an hour • Continous low dose IV infusion • 50 units actrapid in 50 ml • Run at 0. 1 units/kg/hr (0. 05) • Aim to switch off ketogenesis (measure blood ketones or anion gap) • If glucose falls <4 give 2 ml/kg 10% dextrose • Increase glucose

• BG falls up to 25% 1 st hour-fluids alone dilution, CRH, GFR • Better perfusion, counterregulatory hormones (not too much insulin) • If BG falls>5 mmol/l/hr add dextrose — consider bolus — maintain insulin to switch off ketogenesis
-(CL-HC 03) • Clasically high anion gap acidosis • Normal value")
Anion Gap = (Na+K)-(CL-HC 03) • Clasically high anion gap acidosis • Normal value varies amongst centres • Lactate contributes • Anion gap can be normal —Maintained hydration —Loss of ketones in urine —Net Cl gain

Acidosis • Ketoacidosis — HC 03 buffered Anion gap acidosis • Lactic acidosis — Anaerobic glycolysis in tissues • Hyperchloraemia (Cl: Na>80%) — replacement fluid (supra physiological chloride) — Renal loss of bicarbonate precursors (Ac. Ac 3 HB) Acidifying effect of hyperchloraemia can mask resolution of ketoacidosis

• p. H >7. 3, glucose <14 and glucose containing fluid started – reduce insulin to 0. 05 units/kg/hr • If glucose still rising despite above – ? medication error,

• Bicarbonate - ? Associated with cerebral oedema. p. CO 2 low, • Phosphate – replace? • Anticoagulant prophylaxis?

Acidosis not improving • Too little insulin • Inadequate resuscitation • Sepsis • Hyperchloraemic acidosis • Salicylate/ Poison

Cerebral Oedema • Ensure not hypoglycaemic • Mannitol 5 ml/kg 20% • Or 3% saline (5 ml/kg) • Replace deficit over 72 hours – ½ maintenance • CT (bleed/infarction/ venous thrombosis)
 EO : Na,")
Regulation Cell volume Effective Osmolality = 2 x (Na + Glucose) EO : Na, Glucose, or both Rapid fluid administration, bolus insulin Insulin+ Na/H ion exchanger ICF Na

Effective Osmolality DKA Once serum glucose falls below renal threshold and glycosuria decreases there is potential for desalination to cause rapid decreases in plasma sodium

Against Osmolar Theory • Asymptomatic cerebral oedema present pre treatment • Deaths from cerebral oedema pre treatment • Inconsistent association in studies between oedema and management —Cerebral Oedema in Childhood Diabetic Ketoacidosis: Is Treatment a Factor? T B Brown Emerg Med J 2004; 21: 141– 144 Based on the current state of the literature, the idea that treatment for DKA results in CO must be considered an unsubstantiated myth

Blood result- nuggets • Transaminitis not uncommon -25 -50% • CK elevated in 25 -40% • Amylase/Lipase raised in 15 -25% - 12 -24 hrs • WCC – Elevated, Left shift Mechanism unclear —? Catecholamines —Proinflammatoty cytokines (ketones) Don’t presume infective in origin CRP raised in DKA independent of infection

Complications DKA • Cerebral oedema • Cerebral thrombosis • Cerebral haemorrhage • Large vessel thromboses • Pancreatitis • Renal failure • Cardiac arrhythmias

Ketone Detection Nitroprusside Test • Urine —Nitroprusside reacts with acetoacetate not 3 OHB —Unrepresentative of current status —Semi quantitative-does not measure exact levels —Detectable in urine after blood levels normal —Renal reabsorption unpredictable (recovery) —Poor correlation with acidosis (remain positive) —Lactate- false improvement • Blood —Rise before urine levels rise —Real time POINT OF CARE TESTING FOR 3 HB Earlier end point for iv insulin KJ Noyes et al Pedaitric Diabetes 2007 8 150

Nuggetts • Capillary gas unreliable if poor peripheral perfusion • Shock with haemodynamic compromise rare • Hamatocrit implies degree of dehydration • Fluid depletion ICF and ECF • Failure of sodium to rise, falling sodium concerning —Consider increasing Na • Fluid resuscitation will decrease glucose • Insulin needed to switch off ketogenesis, acidosis

Nuggetts • Insulin 1/24 after starting Rx • Max 0. 1 u- avoid decreasing add glucose if necessary (young children may be very sensitive) • Cont until p. H>7. 3 HCO 3 > 15 • Add glucose once 14 -17 sooner if precipitous ie >5 mmol/l/hr- as necessary ie 12. 5%, 15%

Role of Insulin in ICU
 • Insulin resistance •")
Tight glycaemic control? • Stress – high sugars (catecholamines/ cytokines) • Insulin resistance • Adult surgical patients – reduced mortality and morbidity, less ARF, immunoprotective Van den Berghe et al NEJM 2001; 345: 1357 -1367 Flurry of activity – CHIP trial

• Insulin is an effective inotrope • Increases c. AMP and ATP production • ? Any effect on mortality/morbidity? ?

Adrenal Insufficiency

Adrenal
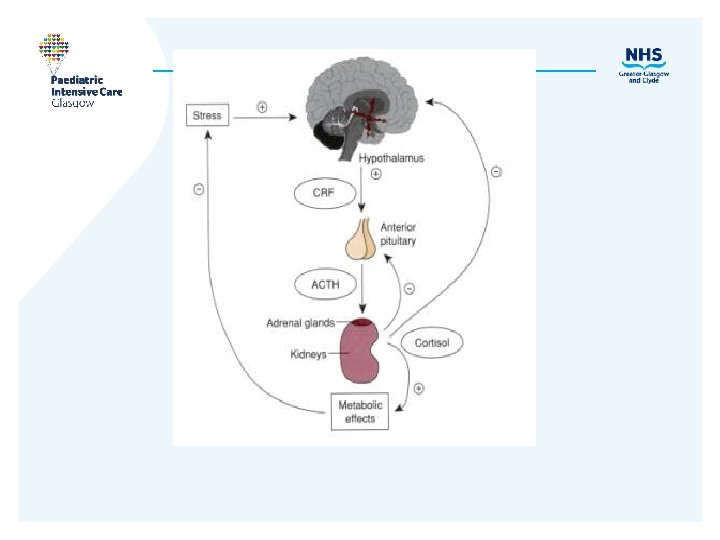
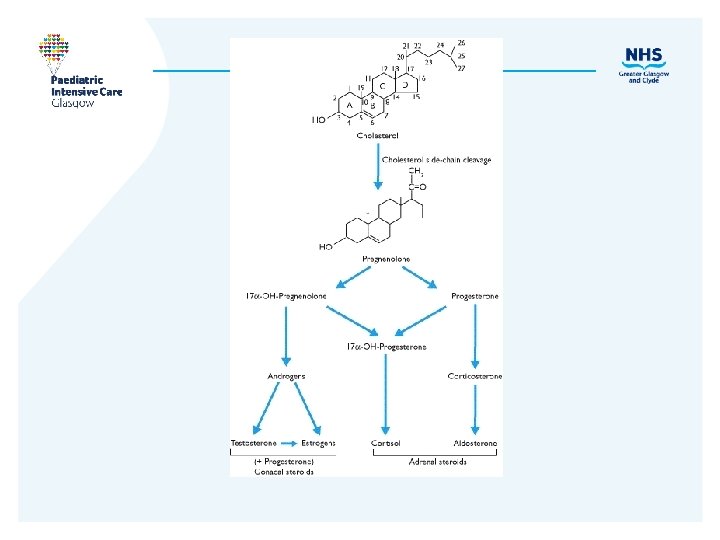

Mechanism of action • Glucocorticoids Increase hepatic gluconeogenesis, glycolysis, proteolysis, lipolysis Inhibit peripheral glucose uptake, immune function, +ve inotrope, Enhance effect noradren/adrenaline, aldosterone. Increase excretion of renal Ca Regulated by ACTH • Mineralocorticoids Maintain intravascular volume. Na retention- lose K+ and H+ Mostly R-A-A pathway.

Steroid deficiency Glucocorticoid Mineralocorticoid Androgen Fasting hypoglycaemia Nausea/ vomiting Weight loss Decreased pubic/ axillary hair Nausea/ vomiting Hyperpigmenta tion Salt craving Fatigue/ muscle Hypotension. wasting High K+, low Na

• • Hyperglycaemia Side effects of Steroids Hypertension Infection Myopathy

Neonate • Congenital adrenal hyperplasia • Steroid synthesis defects – 21 hydroxylase deficiency • Salt wasting – shock and collapse • Virilization of females

Acquired Deficiency • Autoimmune • Fatigue, pain, wt loss, GI • TB symptoms • Adrenoleukody • Hyperpigmenta strophy tion • Waterson. Friedrichsen • Low sugars, • Adrenal low Na, ketosis, haemorrhage high K(late) • High urea, low cortisol • High Ca - Addisons

Treatment • Fluid resuscitate • Give steroid • Stress dose initially ( 2 - 4 x normal) • Avoid hypoglycaemia

• Rise in serum cortisol Adrenal Function in Critical Illness • Changes in circadian rhythm • Decrease in binding proteins • Changes in number and sensitivity of receptors

Stress and cytokines CNS system disease, corticosteroids _ + _ Hypothalamus _ CRH ++ _ Reduced feedback Pituitary Corticotropin ++ _ Pituitary apoplexy, corticosteroids Corticotropin + Cytokines, anaesthetics, antiinfective agents, steroid, haemorrhage, infection Adrenal Increased cortisol and decreased cortisol binding globulin + Tissues Cytokines, local glucocorticoid activation _ Adrenal Decreased cortisol and decreased cortisol binding globulin Tissues _ Cytokines, glucocorticoid resistance
 • Make more glucocorticoid")
Stress and beyond • Initially cortisol high (ACTH, aldosterone low) • Make more glucocorticoid – not driven by ACTH • If remains high too long…. Secondary infections, poor wound healing, myopathy

Relative adrenal insufficiency • To treat or not to treat? • Some people appear not to have an appropriate stress response • Acquired adrenal failure in chronic illness?

To treat or not to treat? The evidence • Meningococcus – rise in cortisol not high enough! • Catecholamine resistant shock • 1995 –Cronin et al – Metanalysis –Crit Care Med – worse outcome • 2001 – Annane – Support – physiologic doses (ACTH stimulation test) • 2005 - Carcillo – Absolute and relative -paediatric
 Hydrocortisone 1. 0 100 Prednisolone 4")
Which steroid? Anti-inflammatory Mineralocorticoid Plasma ½ life (mins) Hydrocortisone 1. 0 100 Prednisolone 4 0. 8 120 -300 Methylprednisolone 5 0. 5 Dexamethasone 30 none Fludrocortisone 200 150 -300

Adrenal Medulla

Phaeochromacytoma • • • Think of diagnosis! Hypertension Urinary catecholamines Sympathetic system Alpha blockers Post-op

Thyroid and ICU

Hypothyroidism • Think about hypothyroidism • Treat early! • Trisomy 21, midline lesions
 •")
Sick Euthyroid • Decrease T 3, increased r. T 3 (occurs if fasting) • Normal T 4 (severe fall) • TSH (low/normal) • Loss of circadian rhythm • Hypothalamic effect? • Later GH, ACTH fall

To treat or not to treat? Controversial ? Energy-saving neuroendocrine adaptation ? Loss of essential hormones –need replaced ?

Drugs and Thyroid Function • Decrease TSH production Dopamine, steroids, octreotide • Decrease thyroid hormone secretion Amiodarone • Increase thyroid hormone metabolism Phenobarbitone, phenytoin, rifampicin

Cardiac function and Thyroxine • Inotropic agent • By-pass give – T 3 –improved cardiac function – Kemperer et al NEJM 1995 • Cochrane Review 2004 –insufficient evidence infants

Thyroid Storm • Precipitants: Thyroid surgery Cessation of medication LIFE THREATENING 20 -30% mortality Trauma /Infection /DKA • Presentation: RARE Fever, Tachycardia, CNS GI Myxoedema coma even more rare in paediatrics

Summary • Reviewed basic anatomy and physiology of endocrine system • Able to manage common endocrine emergencies (hypoglycaemia, DKA, adrenal insufficiency) • Aware of common pitfalls • Awareness of the controversies of endocrine management in PICU
- Slides: 145