Section of Spinal cord Clinical correlation March 10








: PAIN TEMPERATURE CRUDE TOUCH Cross immediately (or sometimes first travels")




, C 2")












")








 and")
 • Spinal muscular atrophy • Friedreich’s ataxia")












 due to N 2 O neurotoxicity Acta Neurologica")









 RBCs in")


- Slides: 72
Section of Spinal cord Clinical correlation 三總神經科部 宋岳峰醫師 March 10, 2014
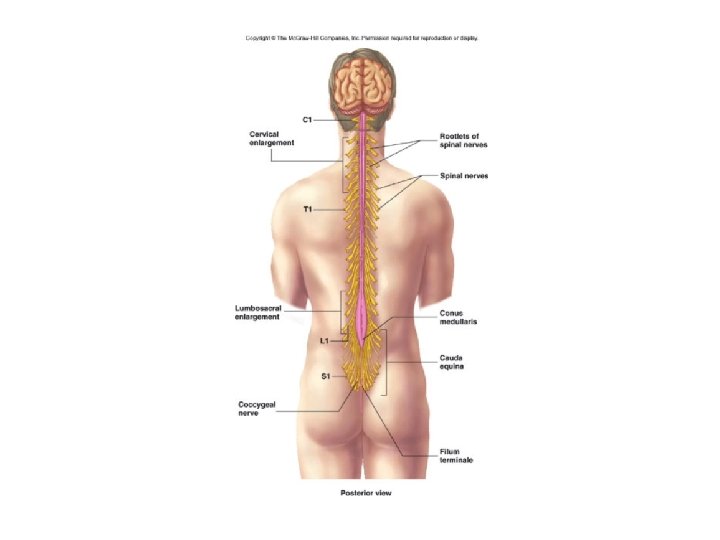
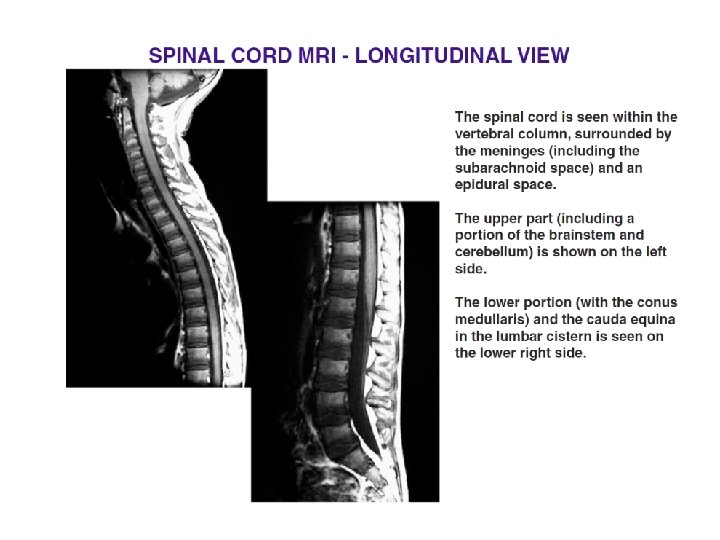
Introduction • Extends from the foramen magnum where it is continuous with the medulla to the level of the first or second lumbar vertebrae • 40 to 50 cm long and 1 cm to 1. 5 cm in diameter • Two consecutive rows of nerve roots emerge on each of its sides. These nerve roots join distally to form 31 pairs of spinal nerves
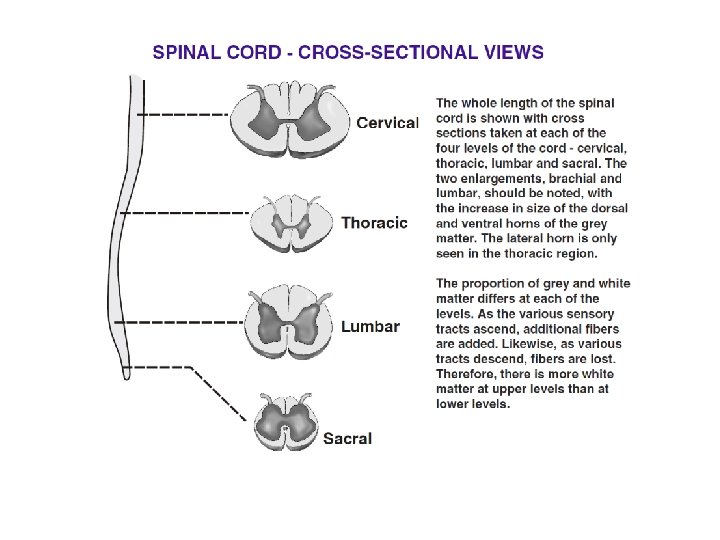
There are 31 segments, defined by 31 pairs of nerves exiting the cord 8 cervical 12 thoracic 5 lumbar 5 sacral 1 coccygeal nerve Coccygeal Dorsal and ventral roots enter and leave the vertebral column respectively through intervertebral foramen at the vertebral segments corresponding to the spinal segment
Intervertebral foramen
Dorsal and ventral roots
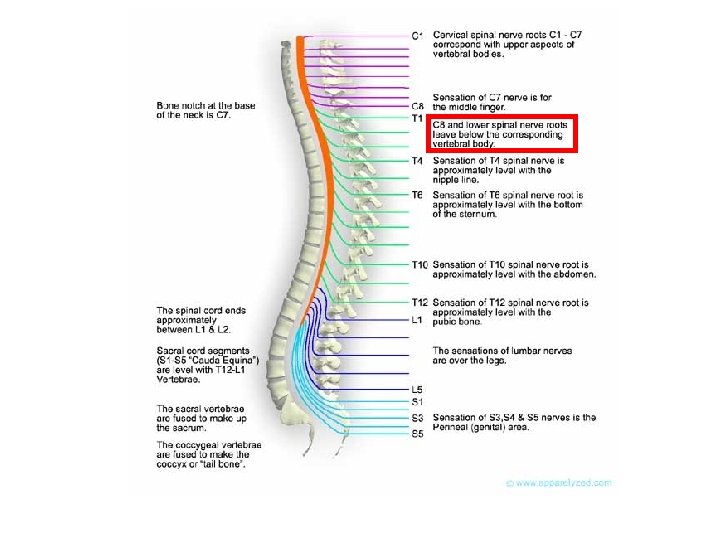
Dermatome
General Features • Carry sensory information from the body and some from the head to the central nervous system (CNS) via afferent fibers • Motor neurons in the ventral horn project their axons into the periphery to innervate skeletal and smooth muscles • Mediate autonomic control for most of the visceral functions
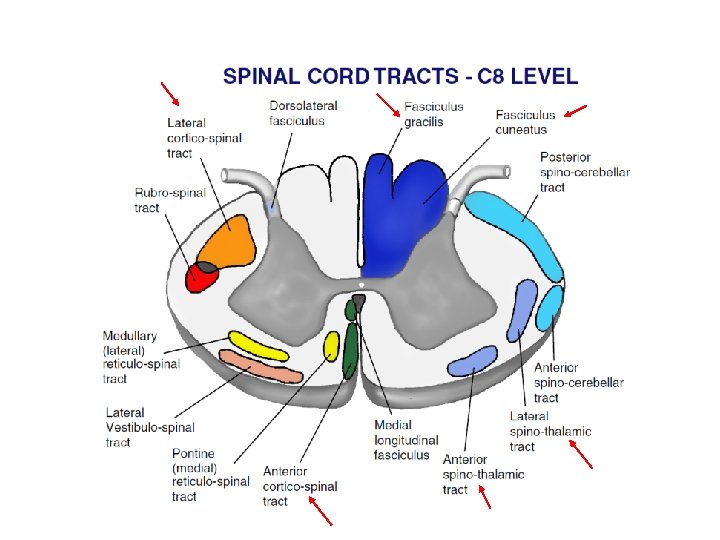
C 8 Level
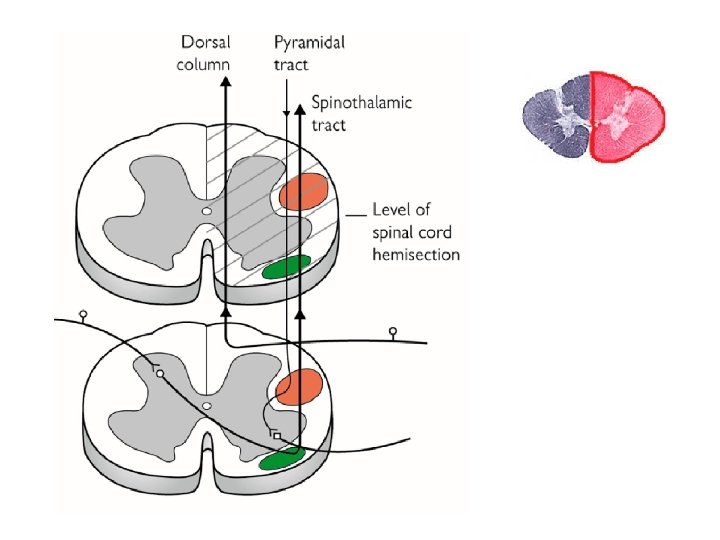
ANTEROLATERAL SYSTEM (spinothalamic tract): PAIN TEMPERATURE CRUDE TOUCH Cross immediately (or sometimes first travels up one or two segments in the cord); therefore contralateral
DORSAL COLUMN - MEDIAL LEMNISCUS PATHWAY : DISCRIMINATIVE TOUCH JOINT POSITION VIBRATION Travels ipsilaterally in the cord and crosses in the medulla
Corticospinal Tract: Carries motor commands from the brain 80% decussate to lateral corticospinal tract 20% continue ipsilaterally as the medial corticospinal tract
Clinical Practice
Longitudinal Localization
High C-spine • Usually associated with trauma - Atlas ring burst (diving), C 2 pedicle fracture with subluxation - Involves quadriparesis and respiratory failure (phrenic nerve: C 3, C 4, C 5)
Low C-spine • Biceps weakness: C 5, C 6 • Triceps, wrist extensors, and pronator weakness: C 7 • Hand weakness: C 8, T 1 • Sensory loss over arms
Thoracic spine • High thoracic spine and low C-spine have sympathetic nervous system involvement (hypotension, bradycardia, Horner’s syndrome) • Sensory level found along the trunk • Some degree of weakness in the leg
Horner’s syndrome • Miosis • Ptosis • Anhydrosis
Lumbar spine • Weakness in the legs • Sensory changes in the legs and saddle area • Conus medullaris: bowel/bladder involvement
Cauda equina • Lower motor signs of flaccidity, areflexia and weakness but with bowel/bladder involvement and sensory level in saddle up to L 1
Patterns of Sensory Loss
Patterns of Sensory Loss Vibration sense Posterior column spinal cord syndrome: B 12 deficiency, Friedrich’s ataxia
Cape Anesthesia Patterns of Sensory Loss Pain and temperature Central spinal cord syndrome: Syringomyelia, Intrinsic spinal cord tumor
Patterns of Sensory Loss Pain and temperature, contralateral to lesion Position, vibration sense, ipsilateral to lesion All modalities, at lesion Brown-Sequard Syndrome: Extrinsic spinal cord tumor
Patterns of Sensory Loss All modalities Complete spinal cord transection: trauma, transverse myelitis
Spinal cord abnormalities
Spinal cord abnormalities Demyelinating disease Tumor Vascular disease Inflammatory disease Infection
Demyelinating diseases • Multiple Sclerosis • Transverse Myelitis (TM)
Tumor • Astrocytoma: slowly progressive • Ependymoma, hemangioblastoma • Metastases to the cord are very uncommon
Vascular disease • Distant vascular occlusion or aortic disease with thrombosis, dissection, or surgical clamping • Sometimes with microscopic fragments of herniated nucleus pulposus • Arteriovenous malformations (AVM) may cause ischemia
Vascular disease
Anterior cord syndrome • Involve the spinothalamic and corticospinal tracts, giving paresis and loss of pain below the level • Usually associated with cord compression, but also can be seen with infarction of the anterior spinal artery
Infarction of the anterior spinal artery
Cord compression
Inflammatory • Vasculitis
Infection • Herpes zoster: radicular pain with dermatomal eruption
• Poliomyelitis: destroys anterior horn cells • Retroviruses HTLV-1 (Tropical spastic paraparesis) and HIV-1 • Neurosyphilis: tabes dorsalis-lancinating pains, dorsal column loss, slapping gait
Degenerative diseases • Amyotrophic lateral sclerosis (ALS) • Spinal muscular atrophy • Friedreich’s ataxia Stephen Hawking suffers from amyotrophic lateral sclerosis
Metabolic diseases • Subacute combined degeneration - Vitamin B 12 deficiency leading to demyelination of the posterior columns and spreading secondarily to the corticospinal tract - Some peripheral nerve involvement - Symptoms including paresthesias, loss of vibratory and position sensation, weakness and spasticity of the legs
Case Discussion
Case 1 • A 38 -year-old woman • Sudden onset of sharp pain at the back of her neck on waking in the morning • Progressive numbness and weakness in her four limbs a few minutes later • Difficulty breathing and urinary retention when she was taken to the ER
• No history of trauma, neck pain, fever, skin rash, or recent illness • Medical history is unremarkable • Denied smoking, drinking and use of illicit drugs • No any significant family history
• BP 110/80 mm. Hg, HR of 82 beats/minute, RR 16 breaths/min and BT 37. 4 o. C • NE: • Normal cranial nerves • Flaccid quadriplegia (MP: Grade 0) • DTR: • Sensation: diminished sensitivity to light touch, temperature and pinprick below the C 2 dermatome. Proprioception and vibration sensations were relatively preserved. • Anal tone: -
Location ?
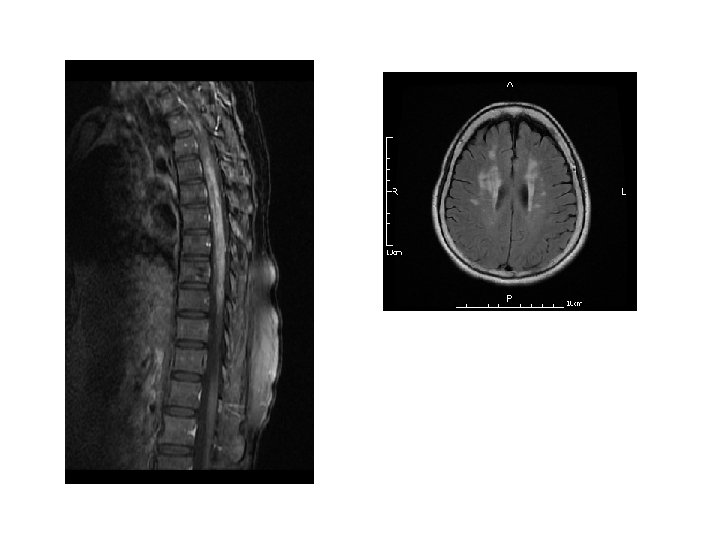
DWI Lt Rt ADC Maps T 2 -Weighted MRI
Diagnosis • Acute cervical spinal cord infarction, extending from C 2 to C 5
Case 2 • A 26 -year-old woman • Weakness and numbness of both lower limbs for 2 days • Previously healthy and denied history of abuse of toxic substances or illegal drugs Acta Neurologica Taiwanica Vol 16 No 2 June 2007
Neurological examination • Mental status, speech, and cranial nerves: normal • MP: 3, lower limbs; 4, upper limbs • DTR: absent, bil. • Sensation: paresthesia in the hands and feet with markedly decreased vibratory sensation in her feet and legs following a distalaccentuating pattern Acta Neurologica Taiwanica Vol 16 No 2 June 2007
Lab Result • NCV/EMG study: sensory-motor demyelinating polyneuropathy • Blood tests: higher MCV (101. 8 f. L), lower B 12 level (187 pg/ml, normal value ≥ 211 pg/ml) Acta Neurologica Taiwanica Vol 16 No 2 June 2007
Diagnosis • Subacute combined degeneration (SCD) due to N 2 O neurotoxicity Acta Neurologica Taiwanica Vol 16 No 2 June 2007
Case 3 • A 35 -year-old man • Good past health • Generalized soreness and sore throat for one day • Difficulty in urination and weakness of lower limbs developed later • Complete paralysis and loss of sensation of lower limbs were noted when he was sent to the Emergency Department
• BP 124/78 mm. Hg, HR of 90 beats/minute, RR 20 breaths/min and BT 38. 5 o. C • NE: • Normal cranial nerves • MP: Grade 5, upper limbs; Grade 0, lower limbs • DTR: ++, upper limbs; -, lower limbs • Babinski’s sign: present, bil. • Sensation: hypoesthesia to all modalities of sensations below the T 6 dermatome
Location ?
Lab result • CSF analysis: pleocytosis, ↑protein, normal glucose, ↑Ig. G Ab to EBV viral capsid antigen (VCA) (1: 1280) and EBV DNA • Nerve conduction study revealed no pick-up of F waves on peroneal and tibial nerves
Diagnosis • Epstein-Barr virus related thoracic transverse myelitis
Case 4 • A 61 year-old woman • Progressive, symmetric weakness and numbness of lower limbs with difficulty urination for 4 days prior to admission • Blindness of both eyes at 7 years old • Paraplegia and paresthesia at 17 years old and got remission after 3 months
Neurological examination • blindness, ou • MP: Grade 5, upper limbs; Grade 3, lower limbs • DTR: ++, upper limbs; +++, lower limbs • Sensory: hypoesthesia over bilateral T 10 dermatome region with impaired vibration and temperature sensation
Location ?
Lab result • • • WBCs in CSF = 98/ul (PMN=84%; MN=16%) RBCs in CSF = 7/ul Protein in CSF = 224 mg/dl CSF virus/bacteria/fungus: negative Blood Aquaporin 4 antibody (AQP 4 Ab): positive
Diagnosis • Optic neuropathy and recurrent transverse myelitis, favor the diagnosis of neuromyelitis optica
Questions?