SECONDARY LOBULE l Normal lung histology l Inflammatory

SECONDARY LOBULE
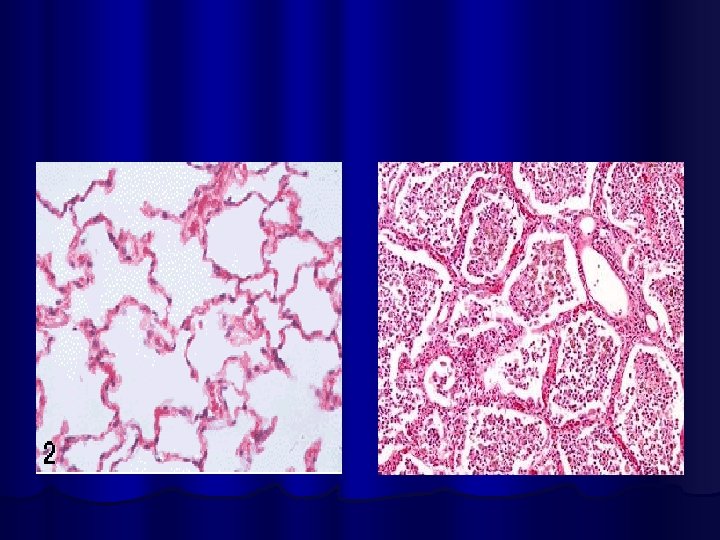

l Normal lung histology l Inflammatory Cells ls. Pneumonia

WHAT IS PNEUMONIA ?

Pneumonia: Definition l Syndrome l caused by acute infection, usually bacterial (may be non bacterial) l Involving lung parenchyma distal to terminal bronchioles l Characterized by clinical and/or radiographic signs of consolidation of a part or parts of one or both lungs.

What are symptoms of Pneumonia ?

Symptoms in Pneumonia l Cough l Fever l Shortness of Breath l Rapid Breathing l Confusion l Restlessness

What are signs of Pneumonia l General Inspection l Respiratory Inspection l Palpation l Percussion l Auscultation

Clinical Signs in Pneumonia l l l Fever Tachycardia Rapid Respiratory Cyanosis in Severe cases Signs of consolidation Reduced movement l Dull Percussion sound l Bronchial Breathing and Crackles l l My be signs of Pleurisy/ Pleural Effusion

Radiological Signs of Pneumonia What is the Hall Mark ?

Radiological Signs of Pneumonia What is the Hall Mark ? CONSOLIDATION AIRBRONCHOGRAM

What is this ?

Pneumonia of RUL

Classification of Pneumonias ? ? ?

Classification of Pneumonia l According to Etiology l According to anatomical site l According to Clinical Settings

Classification of Pneumonia l According to Etiological agent

Classification of Pneumonia l According to Aetiological agent Bacterial Pneumonia l Viral Pneumonia l Bacteria like & Ricketsial Pneumonia l Fungal Pneumonias l Parasitic Pneumonia l Chemical Pneumonia (lipoid pneumonia) l Physical Pneumonia (ionizing radiation) l

Classification of Pneumonia l According to anatomical site Lobar l Segmental l Sub-segmental l Lobular/ Bronchopneumonia/ Diffuse Pneumonia l

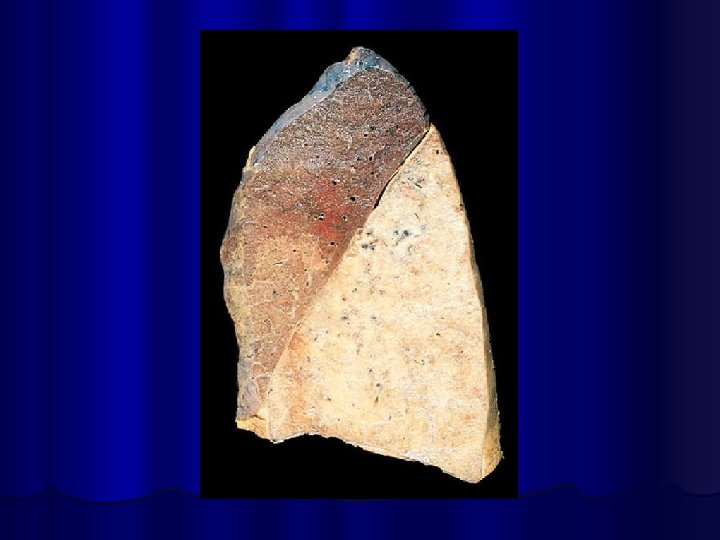
Lobar Pneumonia of RUL

Segmental Pneumonia Right Upper lobe


Bronchopneumonia/ Diffuse Pneumonia
 l")
Classification of Pneumonia l According to Clinical Setting Community acquired Pneumonia ( CAP) l Hospital acquired/Health care associated Pneumonia l Ventilator Associated Pneumonia (VAP) l Aspiration Pneumonia l Hypostatic Pneumonia l Pneumonia in immunocompromised host l

“Community Acquired Pneumonia” Can U define ?
 Pneumonia that begins outside hospital or is diagnosed within 48")
Community Acquired Pneumonia (CAP) Pneumonia that begins outside hospital or is diagnosed within 48 hours of admission in hospital in a patient who has not been hospitalized or residing in a long- term care facility for 14 days or more before the onset of symptoms

AETIOLOGY l l No cause found in 40 -60% of cases In more than 20% cases, more than one organism Bacteria are more commonly identified than viruses Commonest Organisms Strept pneumonaie l Mycoplasma l H influenza l Chlamydophilla pneumonaie l MRSA l Respiratory Viruses l

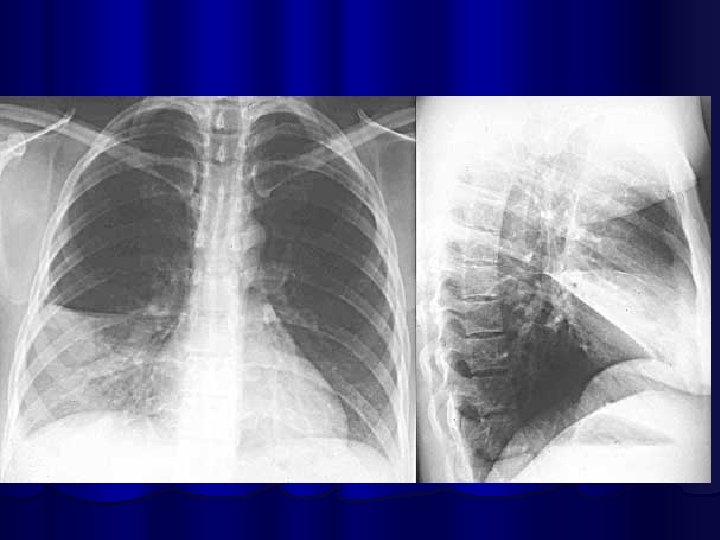
Which lobe is involved l What is the organism l

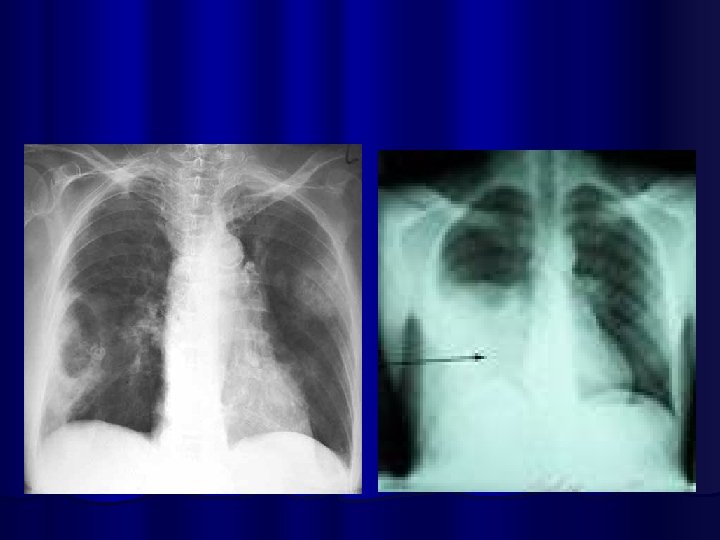
l 60 years old woman is brought to hospital in confusional state. She is febrile and short of breath. On auscultation there are few crackles in the mid zone bilaterally. She is anaemic. WBC count is 6 X 109. l Her chest x-ray is :

What is the diagnosis ?
")
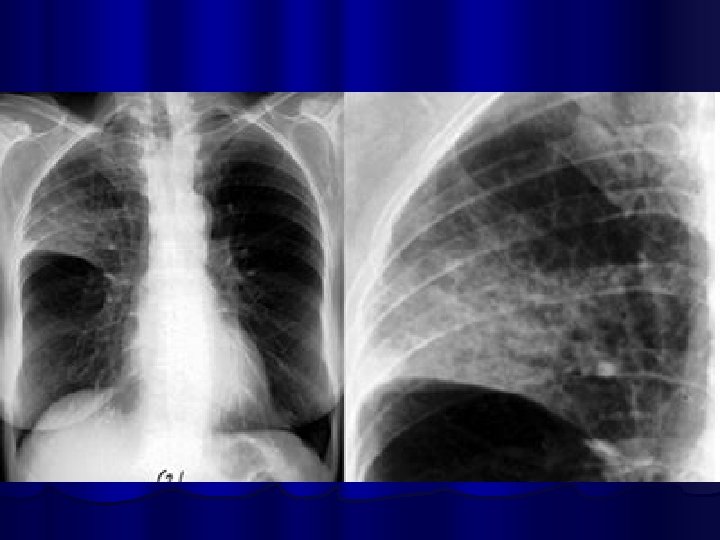
Mycoplasma Pneumonia)

Legionella Pneumonia

RISK FACTORS FOR PNEUMONIA

RISK FACTORS FOR PNEUMONIA l l l l l COPD Pulmonary Oedema Altered consciousness Recent Viral respiratory tract infection Cigarette smoking Alcohol Bronchiectasis Bronchial obstruction Immunosupression Intravenous drug abuse

How the organism reaches Lung ? l Inhalation of micro-organism l Aspiration of gastric content l Spread from contagious site l Hematological spread from distant site

Aspiration

What investigations will you carry out ?

INVESTIGATIONS l l l l l Blood Complete picture Chest X Ray Sputum Gram stain ? Sputum Culture Blood cultures Urea, creatinine, electrolytes Serological studies Arterial blood gases (ABGs) in severe cases Thoracocentesis if effusion is present
")
Serological tests l Pneumococcal antigen l l Mycoplasma antibodies (Ig. M & Ig. G) l l Latex test on urine, sputum & serum Cold agglutinin in 50% cases Legionella antibodies l Immunoflorescence test

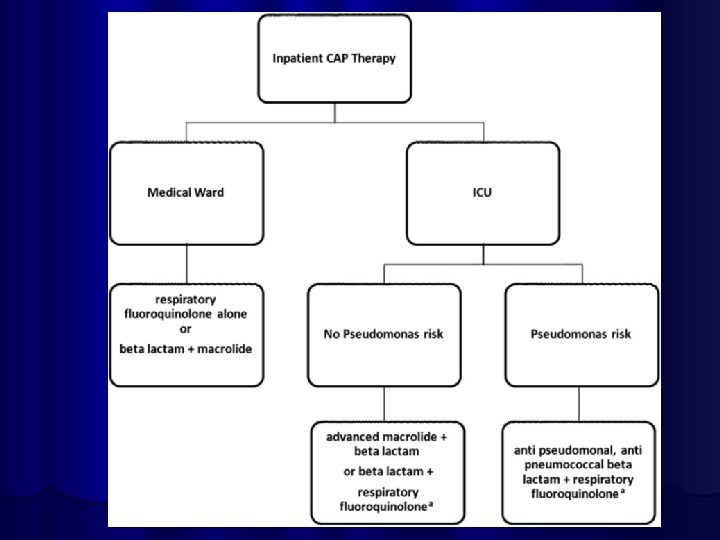
MANAGEMENT OF PNEUMONIA Doctor should assess severity of the Pneumonia and should decide whether patient can be treated at home or in hospital

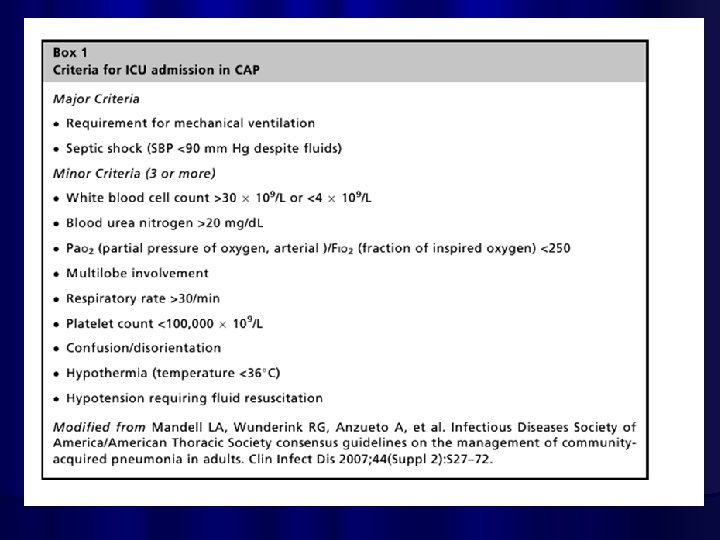
When to admit ? Age > 65 y l Comorbid condition l Abnormal vital signs l RR >30 l BP < 90/60 l Temp > 101 l Altered mental status l Sepsis/ multiorgan dysfunction l Abnormal Lab findings l TLC < 4000 or > 30000 l Po 2 , 60 PCO 2 > 50 l Multi-lobe involvement or pleural effusion l
 Respiratory rate (>30 b/m) Blood")
l l l l Confusion Urea level (>19 mmol/L) Respiratory rate (>30 b/m) Blood Pressure SBP<90 mm. Hg or DBP <60 mm. Hg Age >65 yrs Excellent indicator for mortality

General Measures l Care of mouth and skin l Fluids l Cough Suppressants l Analgesics for pain l Antipyretics for fever l Oxygen


DURATION OF TREATMENT l Influnced by severity of illness, the agent, responsible, and other medical problems l For Strept Pneumonia: treat for 72 hours after the patient is afebrile l For S aureus and Psudomonas, klebsiella, anaerobes, mycoplasma, legionella: two weeks at least

Lung Abcess Empyema

COMPLICATIONS OF PNEUMONIA l Parapneumonic effusion l Empyema l Sepsis l ARDS l Lung abcess l Focal Bronchiectasis

PREVENTION OF PNEUMONIA Polyvalent pneumococcal vaccine l Influenza vaccine l Smoking Cessation l Alcohol cassation l

Thanks

AETIOLOGY BACTERIAL l Streptococcus Pneumoniae l 2/3 rd of case > 30% l Haemophilus influenzae l Klebsiella Pneumoniae l Staphylococcus aureus l Moraxella catarrhalis l Atypical Bacterial l Mycoplasma pneumoniae (9%) l Chlamydia pneumoniae (10%) l Legionella Pneumoniae l Coxeilla burneti l

AETIOLOGY l BACTERIAL l Streptococcus Pneumoniae l 2/3 rd of case Haemophilus influenzae l Klebsiella Pneumoniae l Staphylococcus aureus l Moraxella catarhalis l l Atypical Bacterial l l Mycoplasma pneumoniae Chlamydia pneumoniae Legionella Pneumoniae Coxeilla burneti l Viral l l Influenza A & B Adenovirus Varicella Respiratry syncytial virus Measles Parainfluenza Virus CMV Corona Virus Coxsackie virus Rhino virus

Hospital Acquired Pneumonia Two days after hospital admission l Etiology l Gram negative bacteria l Staphylococcal aureus l Anaerobic organisms l Lobar pneumonia causing organisms l

Staphylococcal

Pneumonia in immunocompromised host Ø Aetiological agents • Pneumocystis carinii • Pseudomonas aeroginosa • Aspergillus fumigatus • Cytomegalovirus • Herpesviruses • Mycobacterium tuberculosis
- Slides: 63