Secondary immunodeficiency Acquired Immunodeficiencies Secondary or Acquired Immunodeficiencies
")

")




, greatly")
")


 infection is characterized by infection of memory CD 4+ T cells")















 CELLS Early: Normal reactivity Late: Reduction but not elimination of")
 – detects viral load �")


- Slides: 32
Secondary immunodeficiency (Acquired Immunodeficiencies)
Secondary or Acquired Immunodeficiencies � Agent-induced immunodeficiency: e. g. infections including HIV � Metabolic disorders and trauma � Splenectomy � Drugs such as corticosteroids, cyclosporin A, radiation and chemotherapy � Aging
Human Immunodeficiency Virus � Discovered in 1983 by Luc Montagnier (Lymphadenopathy virus; Nobel Prize) and Robert Gallo (HTLV-III) � Is a member of genus retrovirus (RNA virus) belonging to Lentiviridae � Characterized by long incubation period and slow course of disease � HIV-1 (Common in US) and HIV-2 (in Africa) � AIDS patients have low CD 4+ T cells � Virus prevalent in homosexual, promiscuous heterosexual, i. v. drug users, transfusion, infants born to infected mothers (prenatally, during birth and lactation) � Opportunistic infections with Candida albicans, Pnuemocystis carinii, Mycobacterium avium, Toxoplasma, Cytomegalovirus (CMV), etc. � Patients with HIV have high incidence of cancers such as Kaposi sarcoma and lymphomas
� Viruses that cause infections, called R 5 viruses, usually use CCR 5 coreceptor, found on effector memory T cells, macrophages, and dendritic cells common in mucosal epithelia. These R 5 viruses are the major virus type through much of early infection period. � As the infection progresses, R 5 viruses may mutate to preferring the CXCR 4 coreceptor, enabling them to infect naïve as well as central memory T cell. These X 4 viruses contribute to the later significant decline in numbers of CD 4+ T cells.
CXCR 4 and CCR 5 serve as coreceptors for HIV infection of different cell types X 4 virus (T-Tropic) Naïve and central memory T cells R 5 virus (MTropic) Macrophages, DCs and effector memory
� Certain chemokines, such as RANTES, had a negative effect on virus replication. CCR 5 and CXCR 4 cannot bind simultaneously to HIV-1 and to their natural chemokine ligands. Competition for the receptor between the virus and the natural chemokine ligand can thus block viral entry into the host cell. � Individuals with deletion mutation in CCR 5 gene making them resistant to viral variants that require this coreceptors.
� Patients with AIDS generally die from tuberculosis, pneumonia, severe wasting diarrhea, or various malignancies. The time between acquisition of the virus and death from the immunodeficiency averages nine to twelve years. � A rise in the level of circulating HIV-1 (viral load) in the plasma and concomitant drop in the number of CD 4 T cells generally previews this first appearance of symptoms.
� Evidence for infection with HIV-1 (presence of antibodies or virus in blood), greatly diminished numbers of CD 4 - T cells (200 cells/mm 3), impaired or absent delayed-hypersensitivity reactions, and the occurrence of opportunistic infections.
Oral Candidiasis (Thrush)
KAPOSI SARCOMA
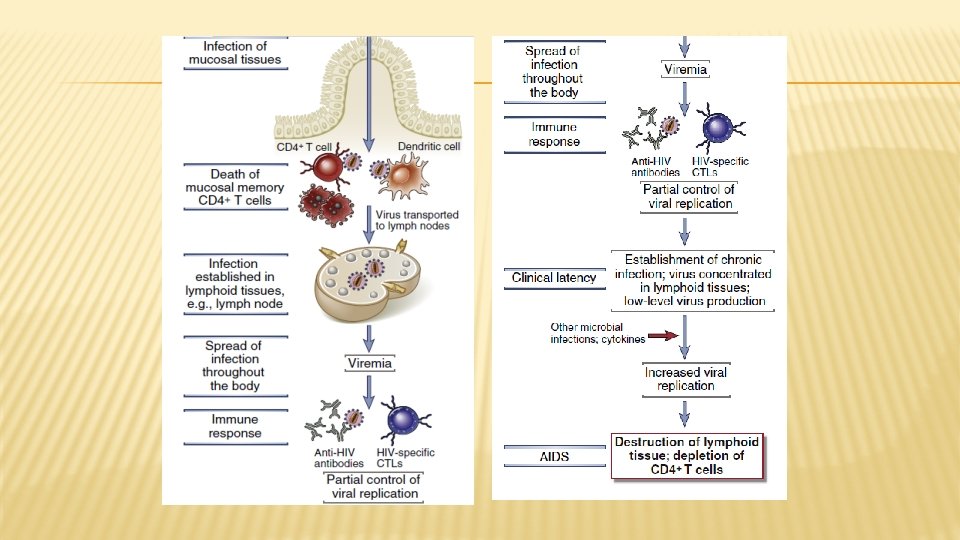
PATHOGENESIS OF HIV INFECTION AND AIDS � HIV disease begins with acute infection, which is only partly controlled by the host immune response, and advances to chronic progressive infection of peripheral lymphoid tissues. � The virus typically enters through mucosal epithelia. The subsequent events in the infection can be divided into several phases.
� Acute (early) infection is characterized by infection of memory CD 4+ T cells in mucosal lymphoid tissues and death of many infected cells. � The transition from the acute phase to the chronic phase of infection is accompanied by dissemination of the virus, viremia, and the development of host immune responses.
� During the acute phase, HIV infection is spreading rapidly among CCR 5 - expressing T cells, and the viral load in the blood as well as in other body fluids can be quite high, elevating the risk of infecting others. � Dendritic cells in epithelia at sites of virus entry capture the virus and then migrate into the lymph nodes. � And may pass HIV on to CD 4+ T cells through direct cell-cell contact.
Within days after the first exposure to HIV, viral replication can be detected in the lymph nodes. This replication leads to viremia, during which large numbers of HIV particles are present in the patient’s blood, accompanied by an acute HIV syndrome that includes a variety of nonspecific signs and symptoms typical of many viral infections � The viremia allows the virus to disseminate throughout the body and to infect CCR 5 helper T cells, macrophages, and dendritic cells in peripheral lymphoid tissues. � Adaptive immune system mounts both humoral and cell-mediated immune responses directed at viral antigens control the infection and viral production, and such control is reflected by a drop in viremia to low but � detectable levels by approximately 12 weeks after the primary exposure. �
� The initial appearance of Ab against HIV Ag seroconversion usually occurs 1 to 3 months after infection. � The most commonly used test for HIV-specific Ab is an ELISA to detect the presence of Ab directed against HIV proteins. � Because of the delay in seroconversion, some HIV ELISA tests also look for HIV Ag in the blood, which may be detectable 2 to 6 weeks after infection. � Positive ELISA results are confirmed using either the more specific Western blot technique, which detect the presence of Ab against several HIV proteins, or PCR assays for HIV RNA.
Soon after infection, viral RNA is detectable in the serum. However, HIV infection is most commonly detected by the presence of anti-HIV antibodies after seroconversion, which normally occurs within two months of infection. � The viral set point refers to the level of virus in the blood at the time of rebound, when the immune response begins to control virus levels. � Clinical symptoms indicative of AIDS generally do not appear for 1 to 20 years after infection, but this interval is variable, and extended by antiretroviral therapy is used. � The onset of clinical AIDS is usually signaled by a decrease in T-cell numbers to below 200/ ml and a sharp increase in viral load. � Patients become very susceptible to opportunistic infections and other health problems. �
viral set point
� This stage is followed by an asymptomatic period during which there is a gradual decline in CD 4+ T cells but usually no outward symptoms of disease. � This is driven by an immune response involving both antibody and cytotoxic CD 8+ T lymphocytes that keeps viral replication in check and drives down the viral load. � Ab provide protection through neutralization, opsonization of virus, and binding to gp 120 on the surface of infected cells, leading to their elimination by ADCC and phagocytosis. � Ab loses effectiveness as the virus mutates due to unrepaired replication errors made by reverse transcriptase.
� The length of this asymptomatic window varies greatly and is likely due to a combination of host and viral factors. � viral replication continues, CD 4+cell levels gradually fall, and viral load in the circulation can be measured by PCR assays for viral RNA. These measurements of viral load have assumed a major role in the determination of the patient’s status and prognosis. � Even when the level of virus in the circulation is stable, large amounts of virus are produced in infected CD 4+ T cells; as many as 109 virions are released every day and continually infect and destroy additional host T cells.
� During this time HIV is mutating, and viruses whose antigens changes to escape recognition by CTLs will survive. � The rapidly evolving virus presents challenges both for the immune system to keep up with these virus escape variants and for the development of drugs and vaccines to treat or prevent progression of the disease.
� � a dramatic depletion of lymphoid tissue and specifically CD 4+ T cells from the GI tract during HIV infection, starting as early as the acute stages of infection. The association between the GI tract and HIV suggeste that TH 17 cells, which express both the CCR 5 and CXCR 4 coreceptors, are the primary targets of infection and destruction. These TH 17 cells are thought to play an important role in homeostatic regulation of the innate and adaptive responses to microbial flora in the gut. Destruction of these cells and disruption of the integrity of the mucosal barrier in the GI tract may allow for the translocation of microbial products across the epithelial lining, explaining some of the rampant immune stimulation that is characteristic of HIV infection. In a deadly feedback loop, this immune stimulation generates yet more activated CD 4+ cells, the favored targets for HIV infection and replication.
The severe decrease in CD 4+ T cells is a clinical hallmark of AIDS � Several explanations have been advanced for the death of uninfected as well as infected CD 4+Tcells. � Lysis of cells actively replicating HIV, abortive HIV infection of resting Tcells (production of viral c. DNA without release of viral particles) cell death WHY? � CD 4+ depletion include � the killing of virus-infected cells by CTLs � Killing of anti-gp 120 antibody-coated cells by phagocytosis, Complement-mediated lysis, NK cell-mediated ADCC. � Cell fusion mediated by binding of an infected cell's gp 120 to an uninfected cell's CD 4 protein � Apoptosis due to induction of Fas. L � Reduced generation of T cells by the thymus
Depletion in CD 4 T cells is the primary cause of immunodeficiency in HIV-infected individuals � Memory T-cells responses such as to influenza virus decline early in the disease progression � Loss of TH 1 decrease or absence of DTH to intracellular pathogen increased susceptibility to TB � Effect both innate and adaptive function AIDS � Chronic exposure to HIV & other intestinal pathogens entering through damaged epithelium systemic inflammation inflammatory mediators cell death & damage to lymphoid organs � Invading gut microbes induce polyclonal B-cell activation (decline in TH) reduce in Ig. G and Ig. A(reduce in T cell dependent Ag)
COURSE OF AIDS Dissemination of virus; Seeding of lymphoid organs Anti-HIV Ab/CTL ACUTE PHASE CHRONIC PHASE AIDS (<200 cells/mm 3)
Death Opportunistic infections <200 CD 4+ T cells/mm 3
Immunological abnormalities associated with HIV infection in different stages 1. Innate and inflammatory response: Early: infection of dendritic cells and transport of HIV to draning LN; some disruction of DCs and ILCs; inflammatory responses induced by HIV, microbes, and their products entering through damaged mucosal barriers, dead cells, and proinflammatory cytokines. Late: on going systemic inflammation; inflammatory cytokine TNF-α and IL-1β can cause cell death ; chronic cell activation contributes to tissue damage; infection of microgilia in brain can result in neurological disorders 2. T HELPER (TH) CELLS: Early: T helper (T) cells Depletion of CD 4 T cells, especially memory T cells in the gut, where TH 17 cells are targeted Late: Further decrease in CD 4 T cell numbers and corresponding TH activities shift from THl to TH 2 responses
Antibody production Early: Enhanced nonspecific Ig. G and Ig. A production Late: Reduced memory and marginal zone B cells. Reduced responses to antigens. Few broadly neutralizing anti-Hl. V antibodies. Decreased class switching, and therefore reduced lg. G and lg. A. 4. Delayed-type hypersensitivity Early: Highly significant reduction in proliferative capacity of. TH 1 cells; shift from TH 1 cells (which mediate DTH responses) to TH 2 cells and reduction in skin-test reactivity Late: Elimination of DTH response; complete absence of skin-test reactivity 3.
5. T CYTOTOXIC (TC) CELLS Early: Normal reactivity Late: Reduction but not elimination of CTL activity due to impaired ability to generate CTLs from. Tc cells resulting from reduced numbers of. TH 1 cells and increased TREG cells, and reduced thymus function.
DIAGNOSIS � RT-PCR (Reverse transcriptase – Polymerase Chain reaction) – detects viral load � ELISA (Enzyme linked immunosorbent assay) � Abs against HIV proteins (sensitive and specific) � Western � Ab Blot detection Infected individuals who have developed Abs (2 wks-6 months after infection) Positive
Treatment of ID: A. Isolation from exposure to any microorganism. B. Replacement of missing protein as Ig, IFNγ, …. etc. C. Replacement of missing cell type by B. M. transplant. D. Replacement of defective gene as IL-2 Rγ chain gene.
References : v Immunology , Kuby, seventh edition 2013 v Immunology , Kuby, eighth edition 2019 v Cellular and Molecular Immunology, Abul K. Abbas, 8 th edition.