SECOND STAGE OF LABOUR SECOND STAGE OF LABOUR

SECOND STAGE OF LABOUR

SECOND STAGE OF LABOUR Ø Begins with complete dilatation of the cervix Ø Ends with expulsion of the fetus POSITIVE SIGNS Ø No cervix felt on vaginal examination

PROBABLE SIGNS Ø Expulsive uterine contractions Ø Trickling of blood Ø Rupture of forewaters Ø Dialation and gaping of the anus Ø Tenseness between coccyx and anus Ø Congestion of the vulva Ø Presenting part appearing Ø Bulging of the perineum

PHYSIOLOGY OF SECOND STAGE q UTERINE ACTION q SOFT TISSUE DISPLACEMENT

PHYSIOLOGY OF SECOND STAGE Ú UTERINE ACTION ü Contractions are stronger and longer but less frequent ü Membranes rupture spontaneously ü Fetal axis pressure increases the flexion of the head ü Contractions become expulsive ü Fergusons reflex increases

PHYSIOLOGY OF SECOND STAGE – Contd…. . Ú SOFT TISSUE DISPLACEMENT ü Anteriorly the bladder is pushed upward into the abdomen ü Posteriorly rectum becomes flattened into the sacral curve ü Levator ani muscles dialate, thin out and displace laterally ü Perineal body is flattened stretched and thinned ü Fetal head visible at the vulva, advancing with contraction and receding with relaxation ü Crowning ü The shoulder and body follow with next contraction accompanied by a gush of amniotic fluid

MECHANISM OF LABOUR LOA

DEFINITION As the fetus descends, soft tissues and bony structure exert pressures which force him to negotiate through the birth canal by a series of passive movements. Collectively these movements are called as mechanism of labour.

PRINCIPLES Ú Descend takes place throughout Ú Whichever part leads and meets the resistance of the pelvic floor will rotate forwards until it comes under the symphysis pubis Ú Whatever emerges from the pelvis will pivot around the pubic bone

The fetus normally situated can be described as…. Ú Lie – Longitudinal Ú Presentation – Cephalic Ú Position – Left occipitoanterior Ú Attitude – Good flexion Ú Denominator – Occiput Ú Presenting part – Posterior part of anterior parital bone

LOA
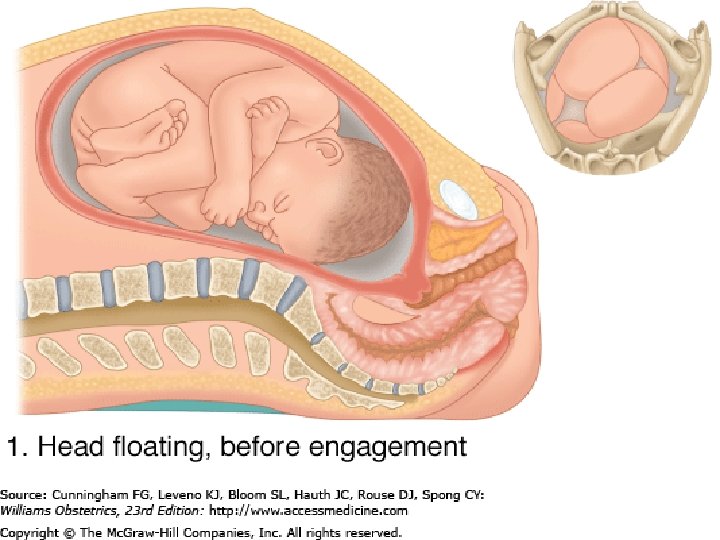

The cardinal movements of mechanism of labour q DESCEND ü Descend takes place throughout the labour ü In a primigravid women it occurs 2 -3 weeks before the onset of labour ü But in multigravida it occurs with the onset of labour ü Uterine contraction and retraction helps in the process ü Rupture of forewater and maternal efforts speed up the process

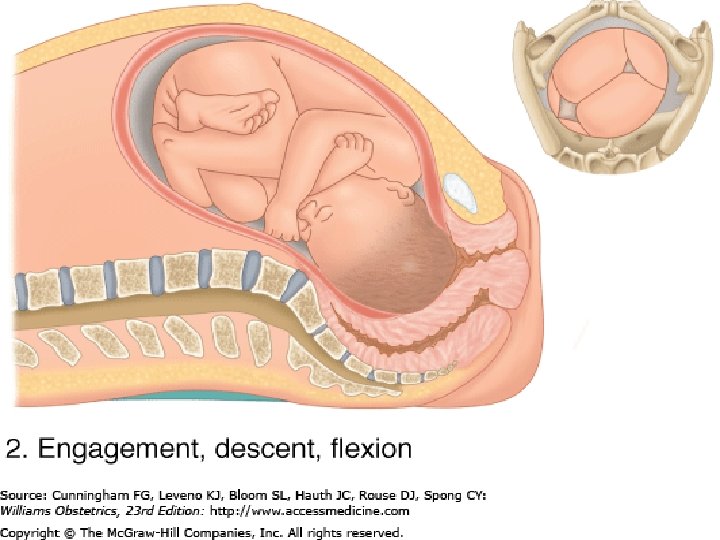
Contd… q FLEXION ü Flexion increases throughout the labour ü At the onset of labour SOF diameter 10 cm presents with increased flexion SOB presents ü And occiput becomes the leading part

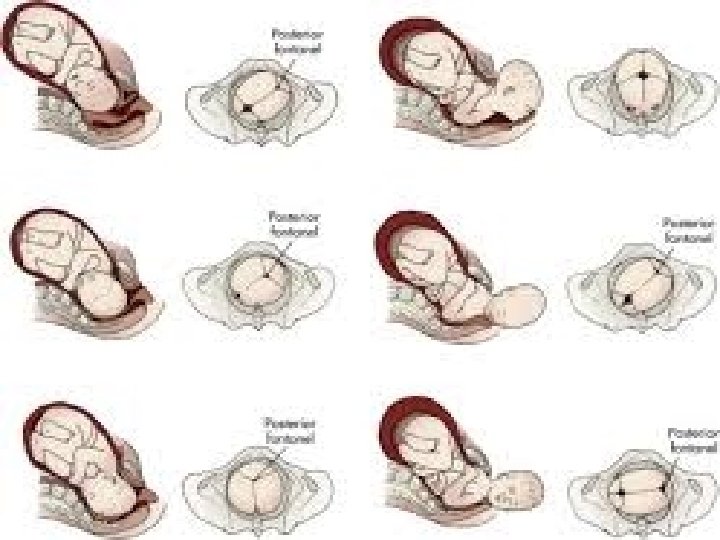
Different types of flexion A. Flexion poor B. Flexion moderate C. Flexion advanced D. Flexion complete

FLEXION

Contd… q INTERNAL ROTATION OF THE HEAD ü In a well flexed vertex presentation occiput leads and meet the resistance of the pelvic floor first and rotate anteriorly 1/8 of the circle to come under the symphysis pubis ü This causes a twist in the neck of the fetus ü Head no longer in alignment with the shoulders

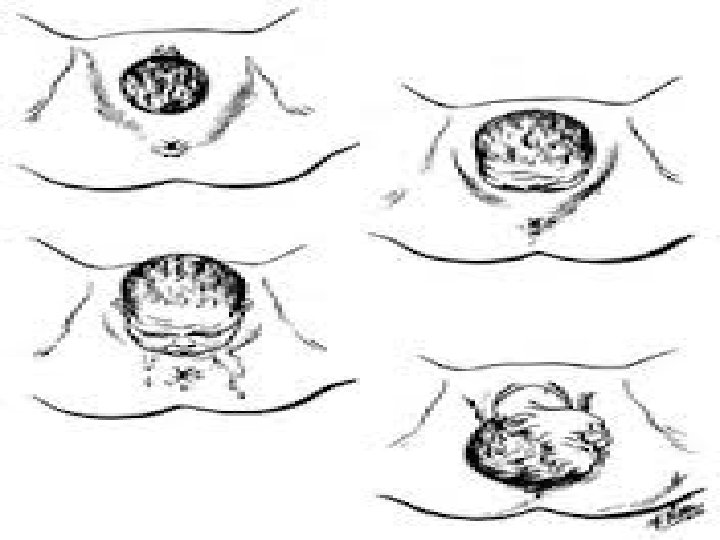
Contd…. q CROWNING ü Occiput slips beneath sub pubic arch ü Widest biparietal diameter is born ü Head no longer recedes between contraction

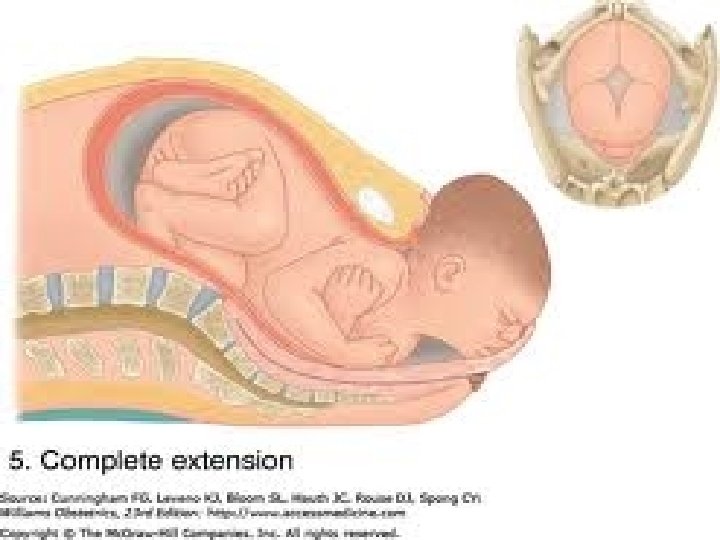
Contd…. q EXTENSION ü Sinciput, face and chin sweep the perineum and head is born by a movement of extension

Contd…. q RESTITUTION ü Twist is corrected by slight untwisting movement ü Head move towards the side from which it started
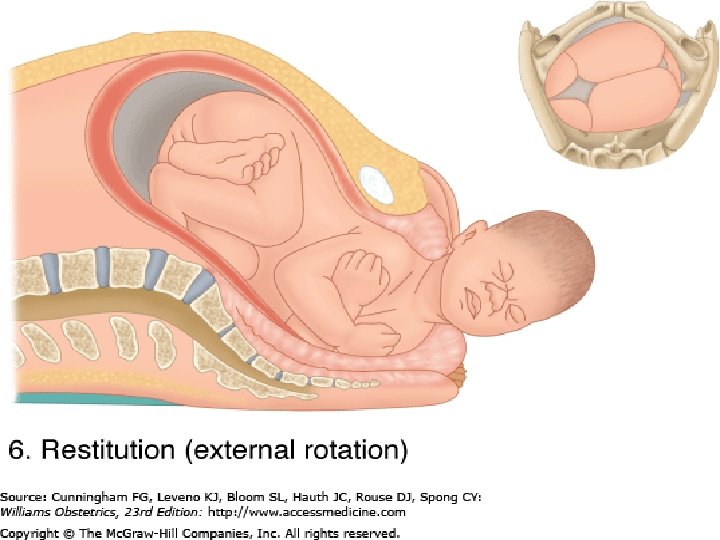

Contd…. q INTERNAL ROTATION OF THE SHOULDER ü Anterior shoulder come and meet the resistance of the pelvic floor first rotates anteriorly to come under the symphysis pubis ü At the same time external rotation of the head also takes place

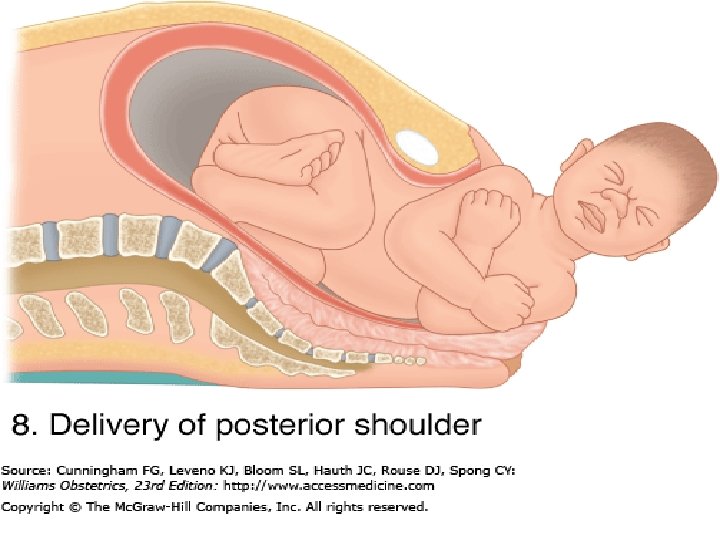
Contd…. q LATERAL FLEXION ü Anterior shoulder slips beneath the sub pubic arch and posterior shoulder sweeps the perineum ü Baby is born by a movement of lateral flexion

MANAGEMENT OF SECOND STAGE q Responsibilities related to first stage of labor q Preparation for deliver q Management of delivery.

EVALUATION OF MATERNAL WELL BEING q Vital signs q Bladder care q Hydration and general condition q Maternal pushing effort q Analgesia and anaesthesia q Perineal integrity ü Ironing out ü Perineal support ü Episiotomy

EVALUATION OF THE FETAL WELL BEING q Normally of the fetal lie, presentation, attitude and position q Fetal adaptation to the pelvis q FHR pattern q The normalcy of progress being made in the mechanism of labor

EVALUATION OF THE PROGRESS Progress of the second stage is based on the following a. Contraction pain b. Length of second stage c. Descend and station d. Progress through the mechanism of labor

Detection of progressive descend includes Ø Progressively lower location of back pain due to pressure from the fetal head. Ø Progressively lower location in the woman’s abdomen of the maximum point of intensity of the fetal heart tones Ø Increasing desire of the woman to push. Ø Change in station of the presenting part noted during vaginal examination Ø Rectal and perineal bulging Ø Appearance of the presenting part at the vaginal orifice

BODILY AND SUPPORTIVE CARE OF THE WOMAN q Breathing 1. Deep breath in and out 2. Controlled breathing 3. Panting q Pushing (help her to make her effort as affective as possible)

PREPARATION FOR DELIVERY Ú Location of the delivery Ú Positions for the delivery

The positions used for delivery are - Lithotomy or dorsal - Left lateral - Supported sitting, semisitting - Squatting - Kneeling - Standing - Knee chest

Left lateral a. Knee chest

a. Squatting a. Standing

GENERAL PREPARATION Ø The room should be warm Ø Adequate light (spot light should be available) Ø A clean area should be prepared to receive the baby Ø A sterile delivery pack Ø Oxytocic agents keep ready Ø Keep ready a radiant warmer / incubater for the baby Ø Arrange and keep ready the neonatal resuscitation equipments

Contd…. Ø A cap and a mask must be worn in the delivery room prior to opening the sterile packs Ø A surgical hand scrub is done as soon as the head becomes visible Ø After hand scrub the midwife must prepare her sterile articles on the instrument table. This include antiseptic solution, cotton wool and pads Ø Practice strict aseptic technique during the delivery

CONDUCTING THE DELIVERY Management of the delivery includes the q Hand manoeuvres used to assist the baby’s birth q The immediate care of the newborn q The following management decisions

Delivery of the baby’s head q Perineum needs to be swabbed q Drape with sterile linen and a pad used to cover the anus q Ritgen’s manoeuvre – it is the technique used to control the delivery of the head.

1. Place the pads of your finger tips on the portion of the Vertex. Spread the fingers over the vertex of the baby’s head with the finger tips pointing towards the as yet unseen face and your elbow pointing upward towards the mother. 2. Allow the head to gradually extend beneath your hand by exerting control, but not prohibitive, pressure with your hand. Use the length of your fingers in doing this and not just the finger tips. Proper control of the head in this manner will prevent expulsive crowing and preserve the perineum

3. An additional manoeuvre of supporting the perineum may also be used. For this cover the hand not being used on the baby’s head with a towel. Place thumb in the crease of the groin midway on oneside of the perinueum. Place the middle finger in the crease of the groin midway on the otherside of the perineum. Apply pressure with the thumb and finger downward and then in ward toward each other across the perineal body

4. While doing this combination of head control and perineal support, observe the perineum in the space between he thumb and middle finger. As the perineum distends, the decision is made as to whether an episiotomy is required 5. Infiltrate the perineum, cut a medio lateral episiotomy and secure hemostasis of required. 6. Watch the perineum, while the head born by extension

7. As soon as the head is born (during the resting phase before the next contraction) place the fingertips of one hand on the occiput and then slide them down the curve of the baby’s head at the level of the top of the shoulders and sweep them in both directions, feeling for the umbilical cord (nuchal cord)

Management of a nuchal cord a. If the cord is loose, slip it over the baby’s head b. If the cord is too tight to slip over the baby’s head but not tight around the neck, slip it back over the shoulders as the baby’s body is born
 and cut")
a. If the cord is tight, immediately clamp about (3 cm apart) and cut the cord at the neck before the baby’s body is born. Tell the mother to pant while you are clamping, cutting, and unwinding the cord.

8. Wipe the baby’s face and head and wipe off fluid from the nose and mouth with a soft absorbent cloth 9. Suction the nasal and oral passages of the bay with a soft, rubber bulb syringe or mucus sucker.

10. Delivery of the shoulders ; wait for a contraction and watch the head return to anatomical alignment with the body (restitution) and extended rotation. External rotation shows that he shoulders are rotating into the shows that the shoulder are rotating into t he anteroposterior diameter of the pelvic outlet, which is the largest space. 11. A hand is placed on each side of the baby’s head over the ears and downward traction is applied. This allows the anterior shoulder to slip beneath the symphysis pubis while the posterior shoulder remain in the vagina.


12. When the axillary crease is seen the head and trunk are guided in an upward curve to allow the posterior shoulder to escape over the perineum. The baby is then grasped around the chest to and the birth of the trunk and lift the baby towards. The mother’s abdomen. This allows the mother immediate sighting of the baby and provides close skin contact the time of birth is noted

E. Clamping and cutting the umbilical cord Clamping the umbilical cord is done by placing two instrument clamps on the cord about 8 -10 cm from the umbilicus

F. Immediate care of the newborn -Patency of air way -Apgar scoring - Themoregulation -Attention to cord and examination of arteries and veins -Bonding

EPISIOTOMY Surgically planned incision of the perineum and the posterior vaginal wall during the second stage of labour

EPISIOTOMY- Objectives q To enlarge the vaginal introitus q To minimise overstretching and rupture of perineal muscles and facia q To reduce stress and strain on the fetal head

EPISIOTOMY- Indications Ø Large size baby Ø Pre term or small for gestational age Ø An uncontrolled woman who is unable to respond to instructions Ø Fetal malpresentation and malposition Ø Rigid perineum (elderly primi) Ø Instrumental delivery Ø To speed up delivery if there is fetal distress

EPISIOTOMY- Types q Medio lateral q Median q Lateral q J shaped

Types of episiotomy 1. Medio-lateral 2. Median 3. Lateral 4. J shaped

EPISIOTOMY- Principles q The presenting part of the fetus is protected from injury q A single cut in any direction is preferable to repeated snipping q The episiotomy should be large enough to meet the purpose. q The timing of the cut. It should not be too late or too early. Ideal time – bulging and gaping of the vaginal orifice, crowing

Anatomy of the pelvic floor

Step I • Cleaning of the perineum • Draping • Local anaesthesia

Step II Incision Structures cut are • Posterior vaginal wall • Superficial and deep transverse (bulbospongiosus and part of levator ani) perineal muscles • Fascia covering those muscles • Transverse perineal branches of pudendal vessels and nerves • Subcutaneous tissue • Skin

Step III Repair • Vagina mucosa and submucosal tissues • Perineal muscles • Skin and subcutaneous tissue

Requirements for episiotomy • Good light source • Linen and dressing • Instruments • Sutures and needles

COMPLICATIONS Immediate: v Extension of the incision v Vulval haematoma v Infection v Wound dehiscence Remote: v Dyspareunia

Post operative care v Dressing v Comfort v Ambulate v Removal of stitches

PERINEAL TEAR CAUSES ü Over stretching of the perineum ü Rapid stretching of the perineum ü Inelastic perineum

PERINEAL TEAR - Types Ú ANTERIOR LABIAL TEAR Ú POSTERIOR PERINEAL TEAR

PERINEAL TEAR Classification Ú First degree Involves the fourchette only Ú Second degree Involves the fourchette and the superficial perineal muscles(bulbocavernosus, transverse perineal muscles and pubococcygeous) Ú Third degree Injury to above structures along with anal spincture Ú Fourth degree Trauma extended to rectal mucosa

PERINEAL TEAR Management OBSERVATION Ú Check for anal spincter control Ú Infection Ú Analgesic and Antibiotic NURSING CARE Ø Cold application first 24 hours Ø After that warm application Ø Liquid diet 24 hours Ø Semisolid soft diet from 2 nd day

Nursing diagnosis 1. Anxiety related to outcome of labor 2. Risk for infection 3. Pain related to physiological response to labor 4. Fatigue 5. Impaired skin in integrity 6. Ineffective individual coping 7. Situational low self esteem

Nursing diagnosis related to newborn 1. Ineffective airway clearance related to airway obstruction with mucus and amniotic fluid. 2. Ineffective thermo regulation related to environmental factors. 3. Risk for altered health maintenance related to congenital disorders.
- Slides: 73