Scrub Circulating Nurse Responsibilities of a Circulating Scrub

Scrub & Circulating Nurse

Responsibilities of a Circulating & Scrub Nurse: • Circulating and scrub nurses are two of the most important healthcare workers in an operating room. Together, they are responsible for anticipating and meeting the needs of the surgeon and patient. During a surgery, each performs her own duties, but they work , together to make the procedure as successful as possible.

Shared Duties: • Both scrub nurses and circulating nurses are responsible for keeping the operating room running smoothly. Each is responsible for patient care; the circulating nurse takes care of the patient before the operation and the scrub nurse monitors the health of the patient during the operation. They also share the task of preparing the room for surgery; the scrub nurse prepares the sterile area while the circulating nurse makes sure back-up supplies are available in case they are

Scrub Nurse:

Scrub Nurse: • A scrub nurse works in the sanitized area of the surgery. He is "scrubbed in, " putting on sterile masks and clothing before approaching the surgical station. The scrub nurse hands the surgical tools and other supplies to the doctor performing the operation. A scrub nurse maintains the sanitation of the operating area, making sure everything stays sterile to reduce the likelihood of contamination. Scrub nurses are also responsible for the care of the surgeon. If her glasses are foggy, or if she is sweating, the scrub nurse is in charge of taking care of those problems, allowing the surgeon to continue her work unhindered. • During the surgery, the scrub nurse is also responsible for monitoring the health of the patient.

A Scrub Nurse Prepares the Surgical Instruments:

A Scrub Nurse Prepares the Surgical Instruments: • The scrub nurse prepares the sterile field, surgical supplies and equipment. During the surgery, the scrub nurse assists the surgeon and the physician assistant by passing instruments, suctioning blood and maintaining the sterile field. A scrub nurse has a degree from a nursing school and at least one

Education of Scrub nurses: • Scrub nurses can complete either a one-year certification program or a two-year associate degree in surgical technology at a community college. Both programs require courses in science, medical terminology, surgical practice and instrumentation. Both paths require a period of practical training. A certifying exam, available upon graduation, is not mandatory.

Duties of Scrub nurses: • Scrub nurses prepare sterile instruments and supplies for a procedure, help the surgeon by passing instruments and keep track of instruments and supplies.

Before an operation: • Ensures that the circulating nurse has checked the equipment • Ensures that theater has been cleaned before the trolley is set • Prepares the instruments and equipment needed in the operation • Uses sterile technique for scrubbing, gowning and gloving • Receives sterile equipment via circulating nurse using sterile technique • Performs initial sponges, instruments and needle count, checks with circulating

SCRUBBING AND GOWNING: • Before each operation, all members of the surgical team – that is, those who will touch the sterile surgical field, surgical instruments or the wound – should scrub their hands and arms to the elbows. Scrubbing cannot completely sterilize the skin, but will decrease the bacterial load and risk of wound contamination from the hands. Every hospital should develop a written procedure for scrubbing that specifies the length and type of scrub to be undertaken. It is usual that the first scrub of the day is longer (minimum 5 minutes) than any

When scrubbing: • Remove all jewellery and trim the nails. • Use soap, a brush (on the nails and finger tips) and running water to clean thoroughly around and underneath the nails. • Scrub your hands and arms up to the elbows. . • After scrubbing, hold up your arms to allow water to drip off your elbows.

When scrubbing:

When scrubbing:

When scrubbing:

When scrubbing:

When scrubbing:

When scrubbing:

Gowning:

After scrubbing your hands: • Dry them with a sterile towel and make sure the towel does not become contaminated. • Hold your hands and forearms away from your body and higher than your elbows until you put on a sterile gown and sterile gloves.

Put a sterile gloves:

Put a sterile gloves:

Put a sterile gloves:

Put a sterile gloves:

Surgical gloves: • Surgical gloves prevent transmission of HIV through contact with blood, but there is always the possibility of accidental injury and of a glove being punctured. Promptly change a glove punctured during an operation and rinse your hand with antiseptic or re-scrub if the glove has leaked during the puncture. Patient safety is of primary concern; do not compromise it. Change your gloves only when it is safe for the patient.

When surgeon arrives after scrubbing: • Perform assisted gowning and gloving to the surgeon and assistant surgeon as soon as they enter the operation suite • Assemble the drapes according to use. Start with towel, towel clips, draw sheet and then lap sheet. Then, assist in draping the patient aseptically according to routine procedure • Place blade on the knife handle using needle holder, assemble suction tip and suction tube • Bring mayo stand back table near the draped patient after draping is completed • Secure suction tube and cautery cord with towel clips or allis • Prepares sutures and needles according to use

During an operation: • Maintain sterility throughout the procedure • Awareness of the patient’s safety • Adhere to the policy regarding sponge/ instruments count/ surgical needles • Arrange the instrument on the mayo table and on the back table

Before the Incision Begins: • Provide 2 sponges on the operative site prior to incision • Passes the 1 st knife for the skin to the surgeon with blade facing downward and a hemostat to the assistant surgeon • Hand the retractor to the assistant surgeon • Watch the field/ procedure and anticipate the surgeon’s needs • Pass the instrument in a decisive and positive manner • Watch out for hand signals to ask for instruments and keep instrument as clean as possible by wiping instrument with moist

Before the Incision Begins: • Always remove charred tissue from the cautery tip • Notify circulating nurse if you need additional instruments as clear as possible • Keep 2 sponges on the field • Save and care for tissue specimen according to the hospital policy • Remove excess instrument from the sterile field • Adhere and maintain sterile technique and watch for any breaks

End of Operation: • Undertake count of sponges and instruments with circulating nurse • Informs the surgeon of count result • Clears away instrument and equipment • After operation: helps to apply dressing • Removes and siposes of drapes • De-gown • Prepares the patient for recovery room

Circulating Nurse:

Circulating Nurse: • A circulating nurse operates as a go-between for the operating room and the rest of the hospital. She is not scrubbed in. A circulating nurse does the initial assessment of the patient as he is wheeled into the operating room and makes sure that the patient is comfortable. The circulating nurse also assists the surgeon and scrub nurse as they clean up and prepare for the surgery. During the surgery, circulating nurses hand packages of supplies to the scrub nurse as necessary. If something is required from outside of the room, or if the surgeon needs a message passed on to another staff or family member, it falls to a circulating nurse. • After the surgery, the circulating nurse counts opened packages and used supplies, to make sure the numbers add up correctly. This is to ensure that

Circulating Nurse:

Circulating Nurse: • The circulating nurse prepares the patient for surgery by setting up the I. V. , attaching the monitoring devices and helping the anesthesiologist. The circulating nurse prepares the operating room for surgery and helps the scrub nurse place the instruments on the table. Education: A circulating nurse has a degree from a nursing school and at

Education of Circulating nurses: • Circulating nurses are required to attend a two-year nursing program that leads to a registered nurse degree. The program includes basic science, nursing and practical courses. Newly graduated nurses must pass a licensing exam in order to practice; an optional operating room

Duties of circulating nurses: • In addition to supervising the room, opening additional supplies for the scrub nurse and taking care of required paperwork, circulating nurses transport the patient to and from the operating room.

Before an operation: • Checks all equipment for proper functioning such as cautery machine, suction machine, OR light and OR table • Make sure theater is clean • Arrange furniture according to use • Place a clean sheet, arm board (arm strap) and a pillow on the OR table • Provide a clean kick bucket and pail • Collect necessary stock and equipment • Turn on aircon unit • Help scrub nurse with setting up theater

During the Induction of Anesthesia: • Turn on OR light • Assist the anesthesiologist in positioning the patient • Assist the patient in assuming the position for anesthesia • Anticipate the anesthesiologist’s needs • If spinal anesthesia is contemplated: Place the patient in quasi fetal position and provide pillow Perform lumbar preparation aseptically

After the patient is anesthetized: • Reposition the patient per anesthesiologist’s instruction • Attached anesthesia screen and place the patient’s arm on the arm boards • Apply restraints on the patient • Expose the area for skin preparation • Catheterize the patient as indicated by the anesthesiologist

During Operation: • Remain in theater throughout operation • Focus the OR light every now and then • Connect diatherapy, suction, etc. • Position kick buckets on the operating side • Replenishes and records sponge/ sutures • Ensure theater door remain closed and patient’ s dignity is

End of Operation: • Assist with final sponge and instruments count • Signs theater register • Ensures specimen are properly labeled and signed

After an Operation: • Hands dressing to the scrub nurse • Helps remove and dispose of drapes • Helps to prepare the patient for the recovery room • Assist the scrub nurse, taking the instrumentations to the service (washroom)

Circulating nurse "flipping" sterile suture material from a suture packet onto the back table:

• i. Sterile areas should be protected from moisture because a moist item may become contaminated. When moisture soaks through a sterile area to an unsterile one, or vice versa, a means of transporting infectious organisms to the sterile area is provided. Therefore, the OR specialist should observe the following rules of practice. • (1) Sterile packages should be laid on dry areas. • (2) If any portion of a sterile package becomes damp or wet, the entire package should be discarded. • (3) If a sterile package falls on the floor, it
 Linen packages from the sterilizer should be permitted to cool before")
• (4) Linen packages from the sterilizer should be permitted to cool before being stored on shelves. This procedure prevents their becoming damp from steam condensation when placed on a cool shelf. • (5) Sterile drapes should be placed on a dry surface. (Thus, time should be allowed for the prep solution used to paint the patient's skin to dry before draping is begun. ) • (6) During surgery, if a solution soaks through a sterile area from an unsterile one or through an unsterile area from a sterile one, the wet area should be

Basic Surgical Techniques:

• One of the major jobs of a Surgical Technologist is to assist the surgeon during an operation. As a sterile team member, the Surgical Technologist may stand directly across from the surgeon in the role of the first assistant or function in the role of the "scrub nurse. " Some of the duties of the assistant are to sponge and suction blood from the operative site, hold retractors and other instruments, and cut suture for the surgeon. An expanded role of a first assistant may include incising and suturing tissue as directed by the surgeon.

• The "scrub nurse" will pass instruments, supplies, and suture to the surgeon during the procedure. The unsterile "circulating nurse" will provide for the safety and comfort of the surgical patient and will be alert to the needs of the other members of the surgical team. For each role, it is vital for the Surgical Technologist to know the various steps the surgeon may take during most surgical procedures. This presentation on "Basic Surgical Techniques" will show the routines for a basic abdominal case, however most of these techniques will apply to any type of surgical procedure.

• By using the surgeon's preference card, the supplies are collected for the surgical case. This may be done in the Operating Room by surgical personnel or in the Central Supply Department and sent to the Operating Room on a

• Prior to opening the first case of the day, flat surfaces and overhead lights are cleaned with a damp cloth moistened with a hospital grade or high level disinfectant.

• Both the scrub nurse and circulating nurse assist with opening the sterile supplies needed for the surgical procedure. Some hospitals have a set routine on where supplies are opened in the room, for example, the suture on the left side of the back table and the linen on the right side. Also unsterile equipment must be obtained. Teamwork is of utmost importance now, and through out the surgical procedure. Supplies and equipment should be obtained at this time because once the patient enters the room, the

• The scrub nurse opens his/her gown and gloves last, preferably on a separate field and proceeds to perform the surgical scrub. Ideally, someone should stay in the room to maintain vigilance over the sterile field.

• Following the surgical scrub, the technologist dries his/her hands using a sterile towel, and dons his/her sterile gown and gloves using the closed gloving method. The Surgical Technologist proceeds to set up the surgical case following that hospital's routine.

• The scrub nurse and circulating nurse perform a sponge, needle, and instrument count before the initial incision is made.

• The circulating nurse obtains the patient's x-rays if necessary and checks on any blood products that may have been ordered.

• The circulating nurse greets the patient who is in the pre-op holding area. The patient's chart is checked for appropriate information. The nurse verifies the patient's identity, the operative procedure and site, doctor, pre-op orders and lab work. An IV may be started at this time by the nurse or a

• When the surgical team is ready, the patient is brought into the operating room and moved to the OR bed. The positioning should be performed by at least two persons, with one standing beside the locked stretcher and the other beside the OR bed. A safety strap is placed 2 -3 inches above the patient's knees and the patient's arms are placed on arm boards. Monitoring devices such as blood pressure cuff, EKG pads, and pulse oxymeter are placed on the

• Following the surgical scrub, the surgeon enters the operating room and is gowned and gloved by the scrub nurse. The surgeon may ask for a moist towel to wipe the powder

• The circulator ties the surgeon's gown in the back.

• The surgeon then preps the patient's skin with an antiseptic solution. If performed on the abdominal area, the umbilicus

• Draping of the patient follows, according to procedure and the surgeon's preference. The scrub nurse should know the draping routine and have all necessary drapes ready in proper order.

• For most basic abdominal draping, four towels are placed around the incision site and held in place with four towel clips. Some surgeons prefer to use a clear plastic drape over the four towels after the skin has been

• A fenestrated drape is applied as the final drape. A laparotomy sheet is used for most surgeries on the anterior

• The surgeon steps into position to operate with the assistant standing across from him/her. The scrub nurse quickly brings up the mayo stand, back table, and ring stand, and places two lap pads at the incision site. A magnetic pad, to prevent instruments from falling from the field, may be placed near the incision site. This pad also contains a "no
 active electrode is secured to the sterile drape followed by")
• The (ESU) active electrode is secured to the sterile drape followed by the suction tip and tubing. An ESU tip cleaner may be placed on the magnetic pad.

• The circulator attaches the distal ends of the active electrode and the grounding pad, applied earlier, to the power unit, and the end of the suction tubing to the suction canister. These units are then

• The circulator then moves the kick bucket into a convenient location.

• When the surgery is ready to begin, the scrub nurse passes the skin knife to the surgeon. The skin knife is usually the #20 knife blade attached to the #4 knife handle. The surgeon and first assistant hold the skin taut as

• Bleeders will be encountered as the incision is made into the subcutaneous layer. The surgeon may elect to coagulate these blood vessels with the ESU or clamp the bleeders with hemostats and tie them off with absorbable suture material. A 3 -0

• The first assistant is responsible for raising the hemostat so the surgeon can get the tie around it and then exposing the point so the knot can be tightened. The hemostat is then removed. Some surgeons prefer for the assistant not to remove the

• After several additional knots are tied, the first assistant will cut the suture. Vicryl is a multifilament suture material and should be cut on the knot. Plain is monofilament and may come untied, so a 3 millimeter tail is

• If the surgeon uses the ESU, the hemostat is held away from the skin edges. The hemostat is touched by the activate electrode and at the surgeon's request is removed by the first assistant. Care must be taken, by the first assistant, to activate the coagulation button on the active

• The surgeon deepens the incision through the subcutaneous layer with the ESU cutting element or the inside knife which is the #10 blade attached to the #3 handle. Whenever the surgeon is cutting, the scrub nurse should be ready to pass a hemostat, in case a blood vessel is encountered.

• The next layer is the fascia. Since the fascia is a tough, white, fibrous layer, the surgeon may use the curved mayo scissors, the inside knife, or the ESU to deepen the incision A Goulet retractor is often used to retract the skin and subcutaneous layer at this time.

• The next layer is the abdominal musculature. If a midline abdominal incision is used, the incision is made between the rectus abdominal muscles. The surgeon may use the handle of the #3 knife for blunt dissection to separate the muscles.

• The next abdominal layer is the peritoneum. It is the thin serous membrane that lines the abdominal cavity. Since the abdominal organs are located directly under the peritoneum, the surgeon must take special precautions to avoid cutting these underlying structures. To enter the peritoneum, many surgeons grasp it with two hemostats and elevate

Electronic-Surgery: System «The Da Vinci» automatic

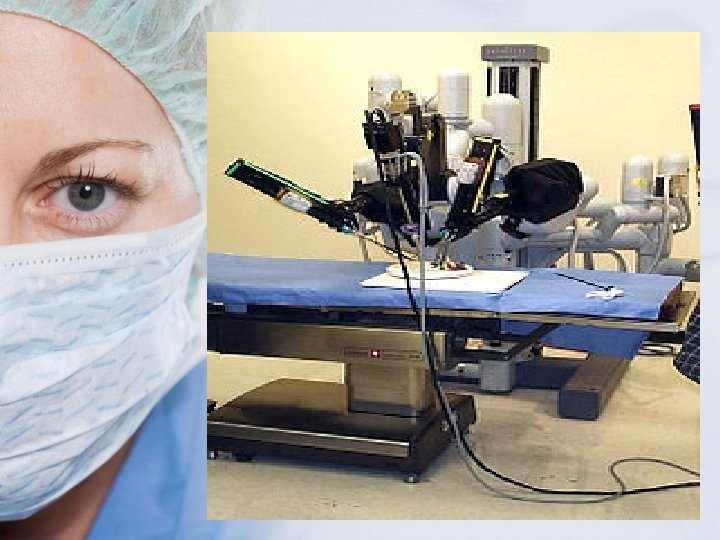
System «The Da Vinci» automatic: • The da Vinci system from the latest systems used in the surgical procedure, which depends on the robot in its procedures. This system, which is the first of its kind that gets the applause and approval by the Food and Drug Administration (FDA) in order to use the latest medical technology and computers. This allows a lot of surgical operations delicate and difficult much easier.

System «The Da Vinci» automatic: • On the other hand comes this system offers a lot of solutions and an end to many of the problems was featured in the surgical system the normal old, for example, to use it speeds up the process of wound healing and ease after the surgery where they do not have a doctor to open a large part of the skin over the place process.

System «The Da Vinci» automatic:

Safety and accuracy: • The use of this system reduces the rate of blood lost during surgery and therefore does not need a doctor for a blood transfusion to the patient during the process, the issue is inevitable in almost all types of operations in the traditional manner. Not to mention reducing the sense of patient discomfort and pain after the operation and dispensing to stay longer in hospital after the operation, and not to mention that the use of robots in this system means to reduce the incidence of contamination of the wound or something like that where not included in

Safety and accuracy: • Of the advantages of the system also can run it after the command, which opens up the way for a surgical procedure on or after the so-called PAL Telesurgry. Jderbalzkr that this system has become in effect in many countries of the developed world such as America, Japan, Germany, France and Australia in addition to the United Kingdom.

Photo: This picture shows hardware da Vinci

: This unit provides")
three basic components, namely: • Unit stereoscopic vision (In. Site Vesion): This unit provides the surgeon with a precise vision of an expanded and multi-dimensional image of the area subject to surgery. The system works by three cameras to capture threedimensional images of the wound from the inside, where this is the only system in the world that has this potential in terms of image and follow-up steps in this process clarity and Holograms.
: • And lined with these three cameras on")
Unit stereoscopic vision (In. Site Vesion): • And lined with these three cameras on an axis to control the evidence according to the status of the patient and the circumstances of the wound, and not the cameras only for vision but there is also the possibility of registration of the video material is seen by a doctor through the cameras and this is what makes the system is also useful to know all the steps carried out by a doctor during the process, which enhances side mode and the possibility of follow-up studying for his doctor's records.
: • It is a set of tools mobile controlled")
Unit labor Animation (Endo. Wrist): • It is a set of tools mobile controlled by the doctor through a special device to replace the human hand perfectly, so that these tools are collectively designed to replace the surgeon's hand from the hand wrist to the fingers and emulated perfectly, and while comes hand automatic imitation of hand, human found surpass them in their ability to move quickly and with more flexibility than regular hand. In addition, they allow a hard skin and dissecting the area of operation and suture the wound after the operation more accurately as well as tissue
: • Contains the organs of control of public order,")
Console General Surgeon (Surgeon Console): • Contains the organs of control of public order, especially in the hand machines, as well as containing the unity of the threedimensional video monitor the process.

Photo: wrist traction device that moves the human wrist and also be more accurate

How the system works: • Surgeon sits in front of the console away from the patient and place of the process and consideration of the wound through the vision system which is similar to my eyes the telescope or microscope to follow up the wound and place of the process. While the control holding the ends of hand tools in front of him and guided to move wherever he wants to hand over the patient's body or inside it.

How the system works: • These endings allow the doctor to carry out movements smartest and more accurate than use it to his regular, in addition to the possibility of work of a doctor for hours without having to wrestle with his hands work on the injured patient, which may lead to an error during the process, those errors that occur, especially in the processes that take a lot time and continuous work. If this system has been tested in the field of cardio-thoracic surgery, it is expected to prove its worth also in the field of surgery of the reproductive system and urinary systems are also effective, particularly for the eradication of the prostate. Will this

Faculty Of Nursing Prepare Student: Karolin El-Sayyed The supervision of Dr. Ahmed abu- Rahma
- Slides: 93