Screening Tests for Cognitive Impairment and Dementia Letitia

 Screening? • Screening: identifying apparently healthy, asymptomatic people who may have")

 • CONSENSUS (1987), SOLVD (1991) • USCHFS (1996), COPERNICUS (2001)")


 • Published 1975, after initial study n=206 • Comprised")














 • Mini-Cog • Mo.")

 4 -6 2 -5 2")










- Slides: 39
Screening Tests for Cognitive Impairment and Dementia Letitia Kinloch, MD
What is (Cognitive) Screening? • Screening: identifying apparently healthy, asymptomatic people who may have or be at risk for a disease • Ideally, there is a next step – Hepatitis C antibody testing as part of the new patient labs at the VA – PSA for prostate cancer screening • Screening for problems with cognition
Why bother? We can’t cure dementia Treating the underlying disease or health condition Managing comorbid conditions more effectively Averting or addressing potential safety issues Allowing the patient to create or update advance directives and plan long-term care • Ensuring the patient has a caregiver or someone to help with medical, legal, and financial concerns • Ensuring the caregiver receives appropriate information and referrals • • https: //www. nia. nih. gov/health/assessing-cognitive-impairment-older-patients#why
• VHEFT (1986) • CONSENSUS (1987), SOLVD (1991) • USCHFS (1996), COPERNICUS (2001) • Val. He. FT (2001) • RALES (1999), EMPHASIS (2011) • SCD-He. FT (2005)
Whom Should We Screen? • • Anybody who is concerned about themselves Anybody whose family is concerned about them Anybody over 80 Barnes Dementia Screening Indicator: – Age – BMI – Hx CVA – Hx Type II DM – Educational level – Need for assistance with medications or money – Current use of antidepressants OR report that “everything was an effort” > 3 days per week Barnes DE et al, Development and validation of a brief dementia screening indicator for primary care, Alzheimers Dement, 2014.
Caveats • Dementia ≠≠≠ Delirium • Don’t test someone who is severely acutely anxious, severely tired, etc. • Keep in mind processes other than dementia which can affect cognition
Folstein Mini-Mental State Examination (MMSE) • Published 1975, after initial study n=206 • Comprised items available at the time, or similar to those available for more extensive testing • Intended to – Screen for cognitive impairment/dementia, differentiate vs. psychiatric disease – Monitor for change over time • NOT to be confused with the Mental Status Examination (MSE) – Appearance, attitude, behavior, mood and affect, speech, thought process, thought content
MMSE • 30 items, max score 30 • Range – No cognitive impairment 24 -30 – Mild cognitive impairment 18 -23 – Severe cognitive impairment 0 -17 • Education – <8 th grade – <12 th grade – college <21 abnormal <24 abnormal <25 abnormal
“Medical Test Taken Down By Copyright Claim” • Forbes/Tech, December 31, 2011 Sweet-16 removed from internet accessibility after legal action by PAR • Newman JC. NEJM, December 29, 2011 “For clinicians, the risk of infringement is real. Photocopying or downloading the MMSE probably constitutes infringement; those who publish the MMSE on a Web site or pocket card could incur more severe penalties for distribution. Even more chilling is the “takedown” of the Sweet 16, apparently under threat of legal action from PAR”
Greenburg, J J
Mo. CA • “The Montreal Cognitive Assessment Mo. CA is a brief cognitive screening tool for Mild Cognitive Impairment” • 1996, Dr. Ziad Nasreddine (neurologist in Montreal, affiliated with Mc. Gill), but didn’t appear in literature until Journal Am Geriatric Society, April 2005 • n = 94, compared to gold standard neuropsychological testing • 30 points: – 18 -26 mild cognitive impairment – 10 -17 moderate cognitive impairment – <10 severe cognitive impairment +1 point for education <12 years • www. mocatest. org
Since then: • Translated to >50 languages • Used in >100 countries • Found to have little/no learning effect and has multiple versions available • Used to screen for cognitive impairment or follow changes in cognitive impairment in : stroke, endarterectomy, complicated grief, mydriatic solutions, atrial fibrillation, picture book reading
“CLINICAL USE: Universities/Foundations/Health Professionals/Hospitals/Clinics/Public Health Institutes: Mo. CA© may be used, reproduced, and distributed WITHOUT permission. The test should be made available free of charge to patients. ” http: //www. mocatest. org/permission/
REGISTER OR LOGIN TO ACCESS
SLUMS • Dr. Syed Tariq, director Division of Geriatrics, St. Louis University • Am Journal Geri Psychiatry, November 2006 • n = 702, compared with DSMIV criteria diagnosis • 30 points – 27 -30 normal, <12 years school 25 -30 – 21 -26 MNCD, <12 years school 20 -24 – 1 -20 dementia, <12 years school 1 -19 • Google “SLUMS test” or “SLUMS VA, ” first thing listed is the test
Mo. CA vs. SLUMS • Psyc. INFO database SLUMS: 10 entries Mo. CA: 334 entries • Mo. CA has been validated in other cultures and >50 other languages • Both correlate with the MMSE • Both have greater range, less “ceiling” than MMSE
Mo. CA vs. SLUMS continued • Cummings-Vaughn LA, Journal Am Geriatrics Society, July 2014 • Compared Mo. CA, SLUMS and Short Test of Mental Status • N = 136 veterans > 60 • Took all 3 tests in random order, neuropsych testing comparison (separate session!) • AUC of ROC’s for MCI and dementia equivalent • Sensitivity, specificity, PPV and NPV all equivalent • Conclusion: similar validity
Why is the VA using SLUMS? • Karansagar D, “A Systematic Evidence Review of the Signs and Symptoms of Dementia and Brief Cognitive Tests Available in VA” Department of Veterans Affairs, April 2010. • VA Evidence Based Synthesis Program Center, Portland, OR (OHSU) • Study is the end result of a VA working group established 2007 set to identify possible MMSE alternatives
• KEY QUESTION #1. What signs and symptoms should prompt VA providers to assess cognitive function as part of an initial diagnostic workup for dementia? • KEY QUESTION #2. Which measures of cognitive function provide the optimal sensitivity, specificity, and time to completion among the measures available to VA providers? • KEY QUESTION #3. What are adverse consequences of using these measures?
6 Screening Tools • BOMC (Blessed Orientation-Memory – concentration Test) • Mini-Cog • Mo. CA • GPCOG (General Practitioner Assessment of cognition) • SLUMS • STMS (Short Test of Mental Status)
Cognitive Domain BOMC GPCOG MC Mo. CA SLUMS STS Orientation/Time + + - + + + Registration/Recall + + + Remote memory - - + - Praxis, Visuospatial - + + + Aphasia, Verbal Fluency - - - + Attention + - - + + + Executive Function - + + +
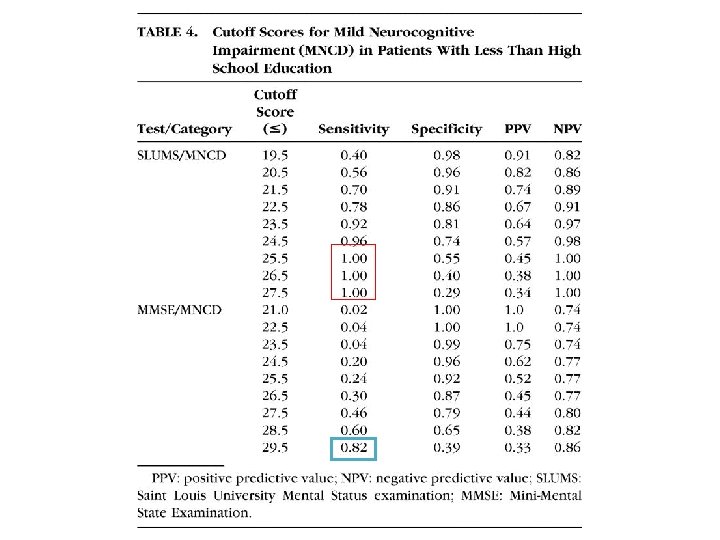
BOMC GPCOG MC Mo. CA SLUMS STS Duration (minutes) 4 -6 2 -5 2 -4 Education Bias + - Sensitivity 0. 83 0. 82 0. 76 Specificity 0. 77 0. 70 0. 89 - 10 -15 + 7 5 - + 0. 94 0. 98 <HS 1. 0 0. 50 1. 0 <HS 0. 98 0. 86 0. 94
SLUMS in the VA • • Validated in veterans Good sensitivity/specificity Shorter Trainees can do it Remaining Questions • ? Learning effect • Other populations
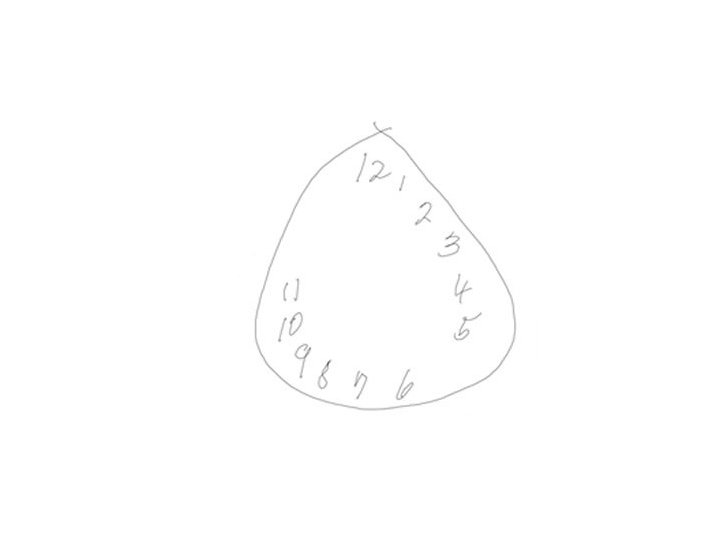
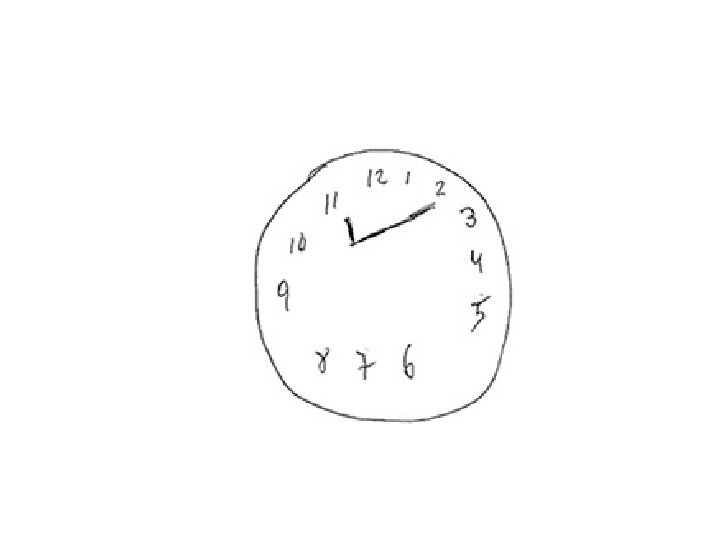
Mini-Cog • 3 -word registration and recall – 3 attempts at registration • Clock drawing – Directions given first to draw the face, when this is done to add the time – 10 minutes after 11 or 20 after 8 – Numbers in correct sequence, none missing or duplicate, roughly right place, 12/3/6/9 in anchors – No points off for hand length – Scoring is all or nothing (2 points) • Score 3 -5 normal, <3 dementia
In Summary, for Screening Purposes: • Don’t use the MMSE • Consider – MOCA • long administration time, low specificity • good sensitivity, validated in MANY different populations) – SLUMS • good specificity and sensitivity in veterans • not yet validated in other populations – Mini-Cog • very short administration time, high specificity, has been evaluated for inter-rater reliability • not as sensitive
Other Purposes • Follow for changes over time • Demonstrate impairment to 3 rd party • As part of assessing decisional capacity
Downside of Screening? • Barriers to doing anything extra during an appointment • False positives • Anxiety and fear associated with diagnosis
Case 1 Ms H is a 94 year old woman with a history of hypertension and coronary artery disease, who recently moved in with her daughter A, after living with a different daughter S in another state for years, after S was in a car accident. Her daughter A is concerned about her memory and that she is not adapting well to her new home. MOCA is 13. What can you tell her daughter?
Case 2 Mr M is an 80 year old with >50 years of heavy alcohol use, admitted with severe alcohol withdrawal. He has now been out of the MICU for a 4 days, vitals and electrolytes are consistently within normal limits, he is no longer on benzodiazepines, and SLUMS is 10. What can you say about him?
Case 3 Mr H is a 65 year old with a history of schizophrenia. He has no family and lives alone with intensive VA case management. His case manager, who has known him for 2 years, is concerned that he is not remembering things as well as he used to. Labs are normal, his psychotic symptoms have not increased, and he feels fine. SLUMS is 14. What should you do?
Case 4 Ms B is an 85 year old former college professor with a medical history of hypothyroidism only. Her husband is concerned because she does not seem as interested in things they used to like to do together, such as walks, crosswords and discussing the news. Ms B says she feels fine. MOCA is 26. What should you do?