Screening for Trauma symptoms or experiences Brooks Keeshin
 Brooks Keeshin, MD Center for Safe and")
Screening for Trauma (symptoms or experiences? ) Brooks Keeshin, MD Center for Safe and Healthy Families University of Utah Department of Pediatrics

I have a problem…

Felitti, et al. 1998

Exposure versus Distress • Which is more important – ACES – Evidence based treatment targets symptoms, not experience • Child Welfare/Justice Dept/Health Care – Population – Goals of individual system • Mental Illness/Family Dynamics – Capability, investment and need

In Practice Application • What is your goal? – Improve trauma reaction/decrease repeated trauma – Decrease emotional distress – Decrease interference with “real” treatment objective • Treating patient versus family versus community • Piece of the overall picture

TRAUMA EXPOSURE

ACEs • The deadly ACEs include: – Physical Abuse – Sexual Abuse – Psychological Abuse – Witnessed Domestic Violence – Family Mental Illness – Family Substance Abuse – Family Incarceration

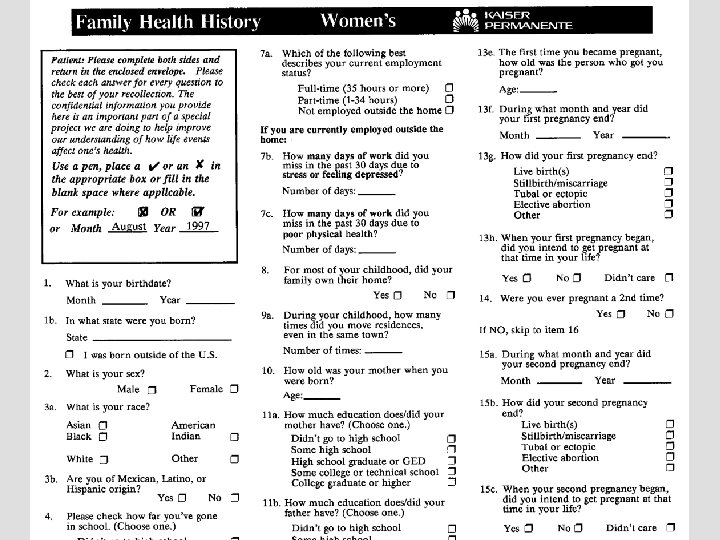
Cross Sectional Studies Study Population Childhood Adult Medical Experience Correlation Felitti >9, 500 et al. , adult 1998 members of Kaiser Health Plan in 19951996 Adverse Childhood Experiences (ACE) Odds Ratios: >3 ACEs Heart dx 2. 2 Cancer 1. 90 Stroke 2. 4 Severe lung disease 3. 9 Obesity 1. 6 Adult Psychiatric Correlation Odds Ratios: >3 ACEs Suicide 12. 2 Depressed 4. 6 Alcoholism 7. 4 Illicit drug use 4. 7 IV drug use 10. 3

Cross Sectional Studies Study Population Childhood Experience Molnar >5800 adults Childhood et al. , in 1990 -1992 Sexual 2001 National Abuse Comorbidity Survey Adult Psychiatric Correlation Green >5600 adults Childhood et al. , in 2001 -2003 Adversity 2010 National Comorbidity Survey Population Attributable Risk Proportions: Odds Ratios: Females Depression 1. 9 PTSD 10. 2 Severe drug dependence 1. 9 Any mental illness 2. 3 Males PTSD 5. 3 Any mental illness 2. 3 Mood 26. 2% Anxiety 32. 4% Substance use 21% Disruptive behavior 41. 2%

Cross Sectional Studies Study Population Childhood Experience Dube et al. , 2010 >5, 300 adults in the Texas Behavioral Risk Factor Surveillance System Survey of 2002 Odds Ratios: Adverse Any Childhood Abuse Childhood Experiences Obesity 1. 5 Fair or poor health 1. 7 (ACE) >18, 00 adults from various countries Childhood Family Adversities Scott et al. , 2011 Adult Medical Correlation Abuse and Household Dysfunction Obesity 1. 3 Fair or poor health 2. 0 Hazard Ratios: >3 adversities Heart Disease 2. 19 Asthma 1. 55 DM 1. 59 OA 1. 44

DEFINITIONS

Definition of Child Abuse • CDC – “Words or overt actions that cause harm, potential harm, or threat of harm to a child” • WHO – “…all forms of physical and/or emotional ill-treatment, sexual abuse, neglect or negligent treatment or commercial or other exploitation, resulting in actual or potential harm to the child’s health, survival, development or dignity in the context of a relationship of responsibility, trust or power. ”

Definition of Child Abuse • Nelson’s – “Child maltreatment encompasses a spectrum of abusive actions, or acts of commission…that result in morbidity or death” • DSM-IV TR – regards both physical and sexual abuse of children and adults as “severe mistreatment of one individual by another…”

Definition of Child Abuse • “Man’s inhumanity to man in its most extreme form – mistreatment and murder of his off-spring – has been well documented throughout each era of recorded history. There has been virtually no conceivable form of inhumanity to children that has not been documented…” – Spitz and Fisher’s Medicolegal Investigation of Death

National Incidence Study

National Incidence Study

Sexual Abuse • Sexual abuse occurs when a child is engaged in sexual activities that – the child cannot comprehend – the child is developmentally unprepared and cannot give consent – and/or that violate the law or social taboos of society.

Age of Consent wikimedia

How about the line between corporal punishment?

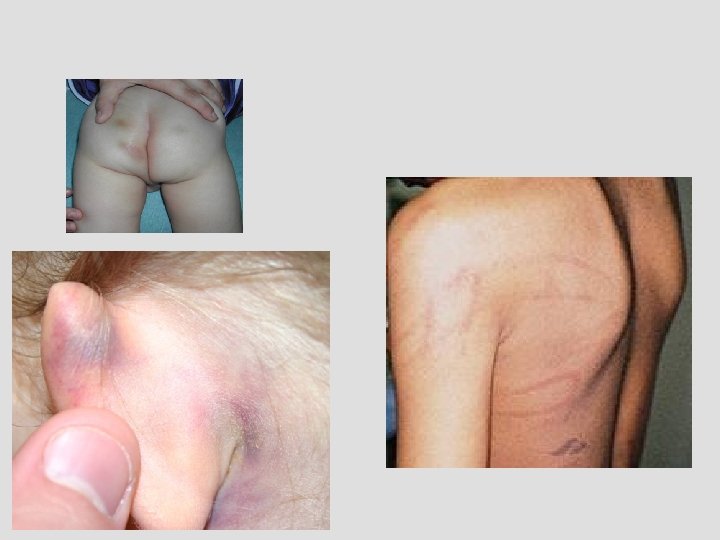
Corporal Punishment vs Physical Abuse

Corporal Punishment vs Physical Abuse

Gershoff, 2008, Report on Physical Punishment in the United States

IT IS ALL HOW YOU ASK THE QUESTION…

Physical Abuse Questions
 Statutory Sexual Abuse")
Sexual Abuse Questions (part 1) Statutory Sexual Abuse

Statutory Sexual Abuse Context Sexual Assault

Lifetime Incidence of Traumatic Events Please circle yes or no to show which things have happened to you. If yes, also fill in the rest of the line. Did this ever happen to him/her How old How much it upset How much it many was s/he him/her then upset him/her times? (first time) now No Yes Been in a car accident None Some Lots No Yes Been hurt in another kind of accident or sick in the hospital None Some Lots No Yes Seen someone else get hurt None Some Lots LITE 2. 1 copyright Greenwald, 1999

Traumatic Events Screening Inventory • 24 Item scale for ages 6 -18 • Wide array of exposure to community, disaster individual and interpersonal violence • Each positive response requests clarifying details – Age, first and last time, most stressful time, how affected • 20 -30 minutes to complete

Childhood Trust Events Survey

Conflict Tactics Scale PC Version • Filled out by parent or guardian regarding interpersonal violence only • Focuses on last 12 months – Once, twice, 3 -5, 6 -11, 12 -20 and >20 times • Includes non-violent, psychologically violent and violent interpersonal acts as well as history of sexual abuse • Can be adapted for interview with older child

TRAUMATIC STRESS

Child Abuse Outcomes • • PTSD Anxiety Disorders Depression Eating Disorders Substance Abuse/Dependence Domestic Violence/Revictimization Parenting Challenges Medical Problems Corwin and Keeshin, Child Adol Psych Clinics of North America, 2011

PTSD and Abuse • Sexual Abuse – 1/3 of foster children have PTSD – 1/3 of victims have PTS symptoms at 3 months • Physical Abuse – Up to 80% have some PTS symptoms, with 30 -50% meeting criteria for PTSD Corwin and Keeshin, Child Adol Psych Clinics of North America, 2011

Criteria A • Threatened death, serious injury or sexual violence • 1. Direct experience • 2. Witnessing in person • 3. Learning event occurred • 4. Experiencing repeated/extreme details of event

Criteria B • Intrusion Symptoms 1. Memories 2. Dreams 3. Flashbacks 4. Psychological distress after exposure to cue 5. Physical distress after exposure to cue

Criteria C • Avoidance 1. Avoidance of memories, thoughts or feelings 2. Avoidance of external reminders

Criteria D • Negative alterations in cognition and mood 1. Poor memory of event 2. Negative beliefs towards self 3. Self blame 4. Persistent negative emotional state 5. Loss of interest 6. Detachment 7. Lack of positive emotions

Criteria E • Increased arousal and reactivity 1. Irritable and angry 2. Reckless and self-destructive behavior 3. Hypervigilance 4. Exaggerated startle 5. Poor concentration 6. Sleep disturbances

Dissociation 1. Depersonalization 2. Derealization

Adult PTSD DSM IV vs. 5 Kilpatrick et al. , J Trauma Stress 2013

Diagnostic Considerations in Youth • Diagnosis is complicated in younger children, especially pre-verbal children – Limitations in abstract thought, emotional processing, language, etc. (Scheeringa et al, 2005/2006/2003) Scheeringa et al. Am J Psychiatry 2006; 163: 644– 651
 examined • the diagnostic requirement")
Diagnostic Considerations in Youth • Carrion and colleagues (2002) examined • the diagnostic requirement of meeting all DSM-IV symptom cluster criteria (i. e. , criteria B, C, and D) in traumatized youth (n = 60) and; • the cumulative importance of the symptom clusters and their relationship to impairment and distress. • 3 groups • children meeting all 3 DSM-IV PTSD symptom cluster criteria • children meeting 2 symptom cluster criteria • children meeting 1 symptom cluster criterion • Traumatized youth with sub-threshold DSM-IV-TR PTSD criteria do not differ significantly from children meeting all three cluster criteria with regard to impairment and distress. • Impairment related to sub-threshold symptoms in children is not due to comorbidity but rather is specific to the posttraumatic symptoms present. Carrion et al. Toward an empirical definition of pediatric PTSD: the phenomenology of PTSD symptoms in youth. JAACAP. 2002

Are alternate diagnosis children symptomatic? Scheeringa et al, 2012, J Trauma Stress

Misclassification of PTSD in children ≤ 6 using DSM-IV-TR Scheeringa et al, 2012, J Trauma Stress

Trauma Symptom Checklist for Children/Young Children • • 54 or 90 item measure Validity Safety Screening Subscales – Depression/Anxiety/Anger – Posttraumatic Stress/Dissociation – Sexual Concerns • Results are adjusted for gender and age
 based")
Child PTSD Symptom Scale • 17 item for child or parent (or both) based on DSM IV criteria • Entry screen for CFTSI (Child Family Traumatic Stress Intervention • Considered positive if at least one symptom is new or worse after a traumatic event with a score of 2 or 3

UCLA PTSD RI • Pros: – Obtain some info of traumatic events as well as assess for symptoms – Child, adolescent and parent versions – Questions assess for Criterion A – D of PTSD – 5 point Likert scale (none of the time to most of the time) is used to rate symptoms • Cons: – Focuses only on PTSD

CAPS CA • Clinician administered tool • Assess for multiple types of traumatic events • Covers complete PTSD diagnostic criteria and independently assesses both frequency and intensity of symptoms • Additional questions for associated features (guilt, shame, attachment behaviors, etc) • 30 minutes to 2 hours to complete

A WORD ABOUT SAFETY
 reported “Wanting to kill myself” at least sometimes")
Suicidal Ideation • 80 teens (33%) reported “Wanting to kill myself” at least sometimes • 29 teens (12 %) reported “Wanting to kill myself” lots of times or almost all of the time (7 patients) • 27 teens (11%) had a “negative” screen but still indicated “Wanting to kill myself” at least sometimes
 reported “Wanting to hurt myself” at least sometimes")
Self Harm • 92 teens (38%) reported “Wanting to hurt myself” at least sometimes • 37 teens (15%) reported “Wanting to hurt myself” lots of times or almost all of the time (12 patients) • 29 teens (12%) had a “negative” screen but still indicated “Wanting to kill myself” at least sometimes

Critical Item Take Home • Teens with suspected abuse are a high risk population for self-inflicted injury and suicidal ideation • 45% of all screens and 30% of all “negative” screens include one positive response about self-harm or suicidal ideation

TASA • Factors associated with suicidal event: – – Self-rated depression Suicidal ideation Higher family income Number of previous suicide attempts – History of sexual abuse • OR 18. 2 (95% CI 2. 5 -130. 6) Brent et al. JAACAP 2009

COMMENTS

Psychotherapeutic Treatment of Pediatric PTSD – Trauma Focused CBT Keeshin and Strawn. Child and Adol Psych Clinics of NA 2014


Latency Age • LONGSCAN analysis – 1300 at risk children • Health problems in abused children at 6 and 12 years of age. • By 6, 67% had experienced at least one adverse event – 1 adverse exposure doubled the risk for overall poor health – 4 or more adverse exposures tripled the likelihood of illness Flaherty et al, 2006, 2009

LONGSCAN • By 12, only 10% had no adverse childhood event • More than 20% experienced 5 or more types of childhood adversity. • At ages 6 and 12, observed correlations with increased adverse experiences – Increased somatic complaints – Overall poor health as reported by the child – Illnesses requiring a doctor’s visit Flaherty et al, 2006, 2009

Longitudinal Study of Low-income Children • Followed >6, 000 children receiving Aid to Families with Dependent Children • Compared children with CPS reports of abuse to matched controls • Used hospitalization for asthma, cardiorespiratory and infection as primary outcome • Children with history of early child maltreatment (prior to age 12) had 75 -100% higher risk of hospitalization Lanier et al. , J Ped Psychology 2009

BMI %ile of Hospitalized Youth Percentage of Patients 70 p = 0. 003 60 50 40 30 20 10 0 0 -20 20 -40 40 -60 60 -80 Body Mass Index Percentile Black – No reported trauma Gray – Reported history of sexual abuse 80 -100

Psychotropic Treatment at Admission 2. 5 2 No Trauma Physical Abuse Sexual Abuse 1. 5 Physical + Sexual Abuse 1 0. 5 0 Number of psychotropics Keeshin, Strawn, Luebbe, et al. 2014 (Child Abuse and Neglect). Total Medications

Length of Stay 9. 5 No Trauma Physical Abuse Sexual Abuse Physical + Sexual Abuse 9 8. 5 8 7. 5 7 6. 5 6 5. 5 5 Length of stay (days) Keeshin, Strawn, Luebbe, et al. 2014 (Child Abuse and Neglect).

Add Health Study Population Physical Assault Hussey et >15, 000 adult Odds Ratios: al. , young adults Poor health 1. 38 2006 who had Overweight 1. 20 previously Depression 1. 75 completed Smoking 1. 22 adolescent Binge drinking 1. 30 surveys Marijuana use 1. 57 Violence 1. 50 Sexual Abuse Odds Ratios: Poor health 1. 65 Smoking 1. 80 Binge drinking 1. 60 Marijuana use 2. 00 Violence 1. 50
 Physical Abuse All No patients Trauma Only (N=1079) (N=694) (N=158) 13.")
Demographics Age (Mean) Physical Abuse All No patients Trauma Only (N=1079) (N=694) (N=158) 13. 6 13. 5 13. 3 Sexual & Abuse Physical Group Only Abuse Difference (N= 172) (N= 55) 14. 20 14. 33 F(3, 1075) = 3. 02* 64. 6 67. 3 56. 3 64. 0 52. 7 28. 6 25. 6 38. 0 28. 5 38. 2 6. 8 7. 1 5. 7 7. 6 9. 1 47. 2 40. 9 40. 5 75. 0 58. 2 Χ 2(3) = 69. 82*** 0. 8 1. 1 1. 4 1. 9 F(3, 1074) = 3. 02* Race (%) White Black Other Sex (% Female) Past Psychiatric 1. 0 Admission Keeshin, Strawn, Luebbe, et al. (in preparation). Χ 2(6) = 13. 22*
 Mood Anxiety (all) PTSD only Disruptive Behavior Substance Use Sexual & Physical")
Diagnosis (%) Mood Anxiety (all) PTSD only Disruptive Behavior Substance Use Sexual & Physical Sexual Abuse Physical All No patients Trauma Only Abuse (N=1079) (N=694) (N=158) (N= 172) (N= 55) Group Difference 51. 2 49. 0 43. 7 54. 1 45. 5 Χ 2(3) = 3. 83, ns 24. 3 10. 1 36. 1 58. 1 63. 6 Χ 2(3) = 241. 59*** 17. 3 1. 0 32. 9 54. 7 61. 8 Χ 2(3) = 399. 00*** 40. 1 39. 5 48. 7 34. 9 40. 0 Χ 2(3) = 6. 96, ns 6. 6 6. 8 4. 4 6. 4 10. 9 Χ 2(3) = 2. 92, ns Keeshin, Strawn, Luebbe, et al. (in preparation).

BMI %ile of Hospitalized Youth Percentage of Patients 70 p = 0. 003 60 50 40 30 20 10 0 0 -20 20 -40 40 -60 60 -80 Body Mass Index Percentile Black – No reported trauma Gray – Reported history of sexual abuse Keeshin, Luebee, Strawn, et al. 2013 J Peds 80 -100

Cross Diagnostic Co-Morbidity • Physical abuse 2 -fold increase in risk • Sexual abuse 3 -fold increase in the likelihood that the patient would have crossdiagnostic comorbidity • No multiplicative risk for crosscategory comorbidity associated with sexual + physical abuse Keeshin, Strawn, Luebbe, et al. 2014 Child Abuse & Neglect

Length of Stay 9. 5 No Trauma 9 Physical Abuse 8. 5 Sexual Abuse 8 7. 5 Physical + Sexual Abuse 7 6. 5 6 5. 5 5 Length of stay (days) Keeshin, Strawn, Luebbe, et al. 2014 Child Abuse & Neglect

Psychotropic Treatment on Admission 2. 5 No Trauma Physical Abuse 2 Sexual Abuse Physical + Sexual Abuse 1. 5 1 0. 5 0 Number of psychotropics Keeshin, Strawn, Luebbe, et al. 2014 Child Abuse & Neglect Total Medications
- Slides: 76