Screening and Treatment of Coronary Artery Disease Matthew


 and area (r=0.")


")























![All Cause Mortality in Patients Without Known CAD Relative Risk All Cause Mortality [NDR]](https://slidetodoc.com/presentation_image_h/16ad75634821e6f32084e9a53ef370ff/image-36.jpg "All Cause Mortality in Patients Without Known CAD Relative Risk All Cause Mortality [NDR]")







 CAC Score")










- Slides: 55
Screening and Treatment of Coronary Artery Disease Matthew J. Budoff, MD, FACC Associate Professor of Medicine Division of Cardiology, Harbor-UCLA Medical Center, Torrance, CA DISCLOSURE INFORMATION: The following relationships exist related to this presentation:
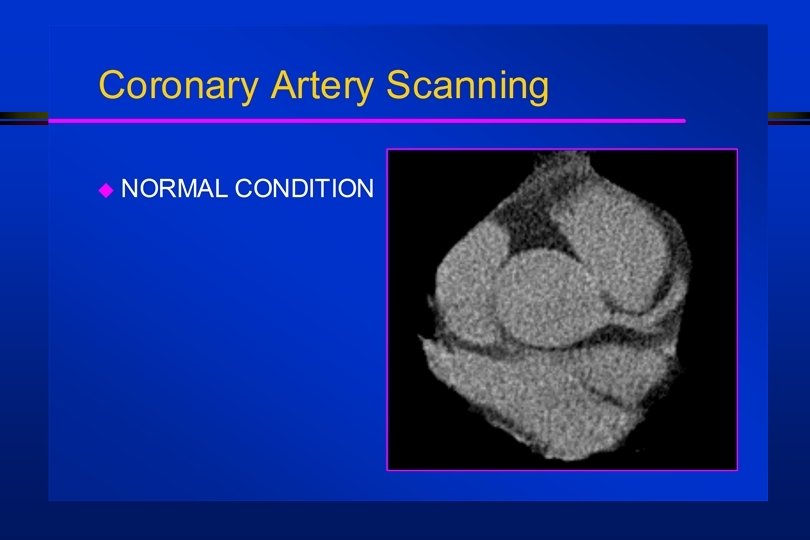
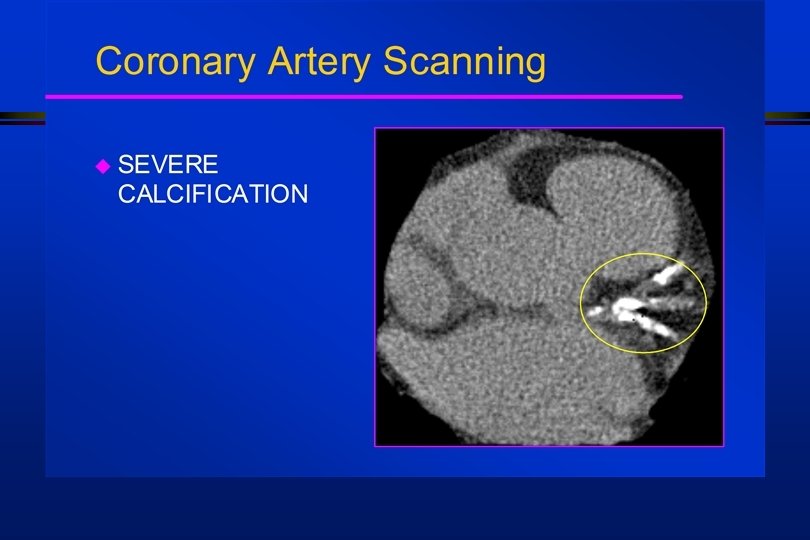
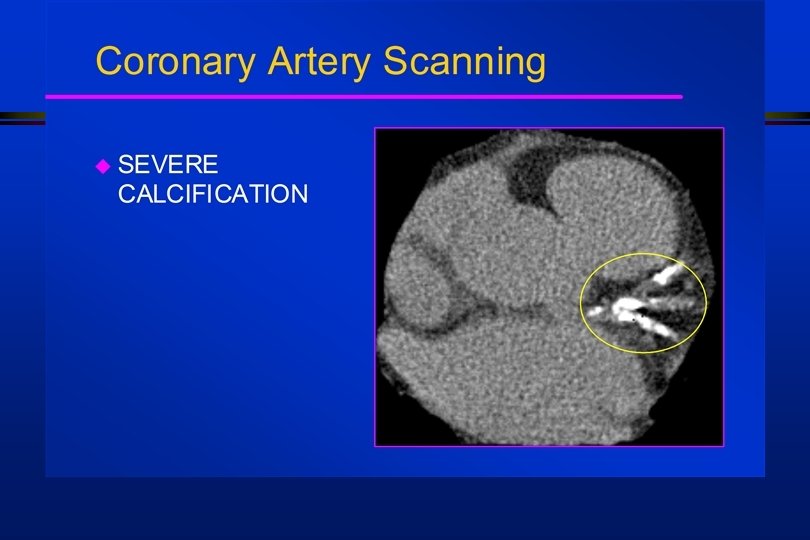
Electron Beam Computerized Tomography Detectors Crystal-photodiodes Preamplifiers Heart 47 cm scan field Radiation shield Patient cross section Source collimator Target ring Vacuum chamber Target rings Vacuum envelope
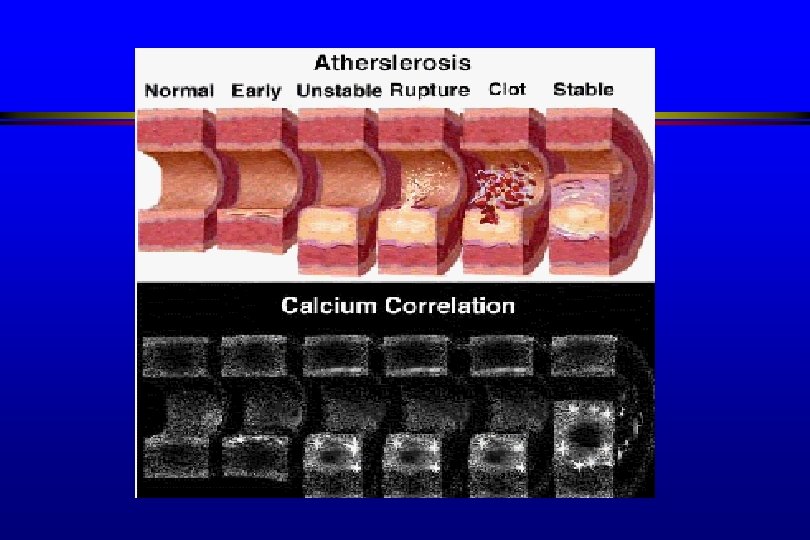
CAC vs HISTOLOGY l l High correlation of score (r=0. 96) and area (r=0. 95) with histomorphometry (p<0. 0001) “. . the amount of coronary calcium increases as the extent of atherosclerosis increases” Mautner GC et al: Radiology 1994; 192: 619 -623
Total Coronary Artery Plaque and EBCT Coronary Calcium 20% Calcified Fibrotic 80% Lipid Rich 20% Plaque Detectable by IVUS, Pathology 80%
Total Coronary Artery Plaque Burden and EBCT Coronary Calcium Score: defining the tip of the atherosclerotic iceberg Mild Plaque Calcium Score Total Plaque Burden Moderate Severe
Framingham Risk in the Young 222 patients with AMI (men < 55, women <65) l Only 25% qualified for pharmacotherapy based on 10 -year risk prior to MI l Only 18% of women met criteria l l Akosah – JACC 2003
Prediction of Cardiac Events in Asymptomatic Patients by EBT Pohle, Heart 2003: 89: 625 -628 l l l 102 patients with AMI, age < 60 years 95. 1% had calcification present Only 5. 8% of controls had calcification present (p<0. 0001) Agatston >50% score – present in 87% By extrapolation, this test may allow identification of 87 -95% of the 650, 000 patients whose first presentation is Myocardial infarction or cardiac death
Refining Framingham Risk Score EBT derived “Arterial Age” a man is as old as his coronaries… Syndenham 1689
EBCT CORONARY CALCIUM SCORES AS FUNCTION OF AGE AND GENDER MALES 1000 900 800 700 600 500 400 300 200 100 0 10 th 25 th 50 th 75 th 90 th 30 -39 40 -49 50 -59 60 -69 70+
EBCT CORONARY CALCIUM SCORES AS FUNCTION OF AGE AND GENDER FEMALES A
Negative Predictive Power of EBT 1764 persons underwent EBT and angiogram l Sensitivity for Obstruction (any calcium) 99. 4% in men, 100% in women l Negative predictive power > 99% l Can be used as a ‘filter’ prior to angiography to help avoid negative angiograms l Haberl et al. JACC Feb 2001
EBCT “Screening” in the Emergency Room: Results in the Mayo Clinic “chest pain unit” 50% women, 98% Caucasian All events occurred in those with CAC Annals of Em Med, 1999 NPV for “Significant” CAD of 100%
CARDIOMYOPATHY l Evaluate Cardiomyopathy of Unknown Etiology using EBT The sensitivity of coronary calcium depicting an ischemic cardiomyopathy was 99% (score >0 = presumed ischemic CM) 1 l Better than echocardiography or stress testing at distinguishing ischemic from dilated CM 2 l 1 Budoff et al. JACC 1999 2 Le T. Clin Card 2000
Sensitivity of Calcium for Future Cardiovascular Events
Rusty Pipe Model of Atherosclerosis
Glagov Hypothesis: Coronary Remodeling Progression Artery can compensate for up to 40% plaque volume (lumen size remains constant) Normal vessel Glagov S et al, N Engl J Med, 1987. Minimal CAD Moderate CAD Artery at maximum expansion: lumen narrows Severe CAD
Glagov Hypothesis: Coronary Remodeling Progression Artery can compensate for up to 40% plaque volume (lumen size remains constant) Normal vessel Glagov S et al, N Engl J Med, 1987. Minimal CAD Moderate CAD Artery at maximum expansion: lumen narrows Severe CAD
Glagov Hypothesis: Coronary Remodeling Progression Artery can compensate for up to 40% plaque volume (lumen size remains constant) Normal vessel Glagov S et al, N Engl J Med, 1987. Minimal CAD Moderate CAD Artery at maximum expansion: lumen narrows Severe CAD
False Negative Coronary Angiography Diffuse Atherosclerosis despite negative angiogram Images supplied by Steven E. Nissen, MD, Cleveland Clinic.
Asymptomatic Persons Nuclear Imaging Hu, Circulation 2000
Historical Development of a Coronary Artery Plaque EBCT “positive” for coronary calcium This process, in various stages of development, can be seen in many areas of the coronary artery system, consistent with the “diffuse” nature of coronary artery disease
The challenge in diagnosis of coronary heart disease “The majority of people destined to die suddenly will not have a positive exercise test. The likely reason that they will die suddenly is that only a mild, non-flow -limiting coronary plaque will have been present before the sudden development of an occlusive thrombus. ” - Stephen Epstein New England Medical Journal 1989
RR of MI/SCD: EBT Score and hs-CRP Park et al. Circ. 2002; 106 -2073 -2077 High hs-CRP Low hs-CRP
CAC by EBT and Cardiac Events n=64 99% 65 Cardiac Events (Cardiac Death, MI, Revasc) 696 pts. 53+11 yrs 50% males 2. 7 year f/u n=1 1% Event Rate: 6%/yr <. 1%/year Raggi et al Circ 2/00
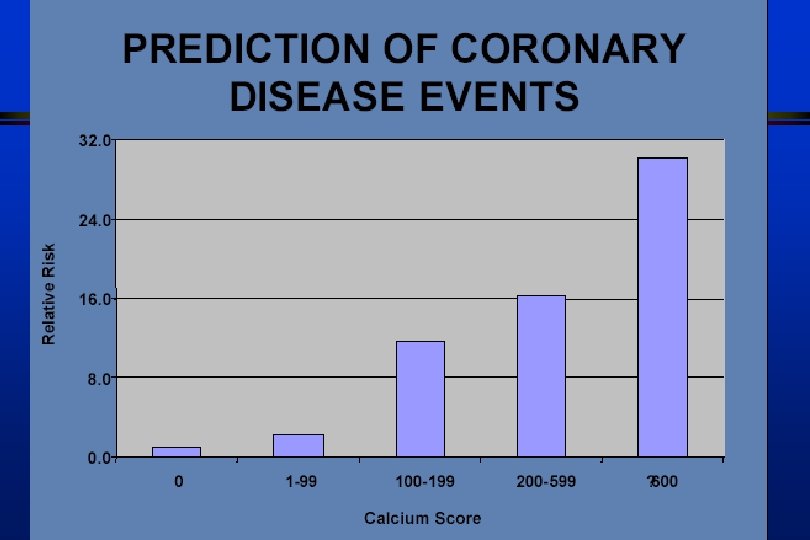
Event Rates Based upon Scores Raggi, AHJ 2001
High Coronary Artery Calcium Scores Pose an Extremely Elevated Risk for Hard Events Figure 1. Probability of survival free of events in 98 consecutive asymptomatic subjects with calcium score >1, 000 on a screening electron beam tomography scan. Wayhs R, Zelinger A, Raggi P, J Am Coll. Card. , Vol 39: pp 225 -230, 2002
Relative Risk Of Future Cardiac Event using EBT Raggi Wong Detrano
Prediction of Cardiac Events in Asymptomatic Patients by EBT Kondos et al, Circulation 2003; 107: 2571 -2176 5635 asymptomatic, low to intermediate risk patients, 37+12 m f/u Cardiac events: MI, SCD, revascularization, age 30 -76, avg 51+9 yrs. 1. 05 0. 87 Age: 1. 04 -1. 07 1. 39 Smoking: 1. 04 -1. 87 Elevated TC: 0. 65 -1. 07 1. 98 Relative Risk 1. 33 DM: 1. 19 -3. 28 HTN: 0. 98 -1. 81 Presence of CAC: 3. 85 -28. 4 0. 75 1. 0 1. 25 1. 50 3. 0 10. 46 30. 0
Prediction of Cardiac Events in Asymptomatic Patients by EBT The St. Francis Heart Study, ACC 2003 10. 7 9. 5 9. 9 Relative Risk Annual Event Rate (%) Calcium Score >100 vs <100 Any Baseline EBT Calcium Event Score Cor. Event MI/ SCD 3 SFHS
All Cause Mortality in Patients Without Known CAD Relative Risk All Cause Mortality [NDR] n = 10, 377 asymptomatic men and women f/u = 5. 0+3. 5 yrs. EBT found to be independent and incremental to risk factors DM Smoke HTN Shaw, Raggi et al In Press, Radiology 2003 <10 10 -100 101 -400 >1000 401 -1000 EBT Coronary Calcium Score
5 Year Mortality
EBT 5 year All-Cause Mortality
Risk Stratification – Shaw et al.
Rationale for Use of CAC in Different Populations Risk Category Population Number Shifted Needed to Scan Low 35% 2% 50 Intermediate 40% 73% 1. 3 High 25% 16% 7
Asymptomatic Patient Algorithm for Intermediate Risk Patients Greenland P, et al. Circulation Oct 9, 2001
NCEP ATP-III : Noninvasive Testing “measurement of coronary calcium is an option for advanced risk assessment. High coronary calcium scores (e. g. , >75 th percentile for age and sex) denotes advanced atherosclerosis and provides rationale for intensified LDL-lowering therapy. ”
Prevention V Guidelines Used a score >80 by EBT to implement aggressive drug treatment in Framingham intermediate risk patients l In patients with a zero score, “one would not be justified to intervene with costly lipid lowering drugs at this time” l
Percent Volume Change vs LDL Treated Untreated Suboptimal Therapy (LDL >120 mg/dl) CAC Score Change +120% 0 – 80% 60 120 LDL (mg/d. L) Callister et al. N Engl J Med. 1998; 339: 1972 -1978. 200
Rates of Progression of CAC n=66 25% 8. 8% P<0. 0001 Before Statin Achenbach S, Circulation, Vol 106: Aug. 27, 2002 After Statin
32 Patients who achieved LDL <100 Mg/d. L n=32 27% -3. 4% P=0. 0001 Before Statin Achenbach S, Circulation, Vol 106: Aug. 27, 2002 After Statin
Annual Event Rate with Progression 13 X Risk Annual CAC Score Change Raggi, Budoff AJC 2003
Progression and Medical Intervention
COMPLIANCE “Willpower lasts about two weeks…. And is usually soluble in alcohol” l Mark Twain/Sam Clemens
Compliance and Lipid-Lowering Therapy l ~50% of patients discontinue lipid-lowering therapy within 1 year. l ~75% of patients discontinue lipid-lowering therapy within 2 years. Roberts, Am. J. Cardiol. 78: 1996: 377 -378.
Percentage of individuals maintaining Statin therapy at 3. 6 years according to various levels of baseline CAC
Odds ratio of maintaining statin therapy with various levels of baseline CAC 28. 9 9. 1 5. 1 2. 4 1. 1 9. 3 4. 2 3. 0 1. 9
5 USES OF EBT l Use a calcium score to screen patients with moderate (intermediate) Framingham risk Positive EBT scans indicate incremental risk n Alters therapeutic goal (LDL, BP, etc) n l l Identify patients who do not need further cardiac evaluation (scores of zero) Consider serial imaging as ongoing management tool (progression) Improve compliance Non-invasive Angiography
EBT Coronary Calcium