Scleroderma and the Kidney David Shure July 14








")


 Blobe G et")










- Slides: 24
Scleroderma and the Kidney David Shure July 14, 2009
DD: Renal Failure • ATN • Renal Scleroderma Crisis
Epidemiology • Prevalence: 19 -75 cases per 100, 000 • Susceptibility – Age: peak occurrence 35 -65 – F: M 7 -12: 1 – Environmental Factors: infection – Occupational exposure: silica dust – Usually occurs w/in 4 -5 yrs of SSc onset
Local vs Systemic Disease
Classification – dc. SSC: diffuse cutaneous SSc – lc. SSc: limited cutaneous SSC – SSc sine scleroderma – internal organ involvement – Environmentally induced scleroderma – Overlap syndrome: ie MCTD
• • • Calcinosis cutis Raynaud Phenomenon Esophageal dysmotility Sclerodactyly Telangiectasia
Pathogenesis • Complex and poorly understood • Immune activation • Inflammatory response • Vascular damage • Excessive synthesis EC matrix and collagen deposition • Hypothesis: interplay between early immunological events and vascular changes leading to generation of a pop of activated fibrogenic fibroblasts believed to be effector cells in disease
Vascular and Endothelial Changes • Appear to precede other features of SSc • Vasoconstriction – ET-1: significantly elevated in SSc and assoc with pulm htn, may initiate fibrosis – Superoxide anions: released from endothelium neutralize NO – Defective vasculogenesis: fewer circulating endothelial ell precursors ie CD 34+, CD 133+ and VEGF type 2 – Pts with SSc have incr in endothelial cell surface expression of adhesion molecules and elevation in circulating levels of their soluble forms. Cytokine induced upregulation of adhesion molecules ie ICAM-1, VCAM-1, ELAM-1
Autoantibodies • 75% pts with SSc have circulating autoantibodies – Topoisomerase I (anti-scl 70) • anti-topoisomerase antibodies highly specific for SSc, and correlate with greater risk for ILD and more extensive skin involvement – Centromere antigens (12 -44%) • Anticentromere antibodies assoc with limited cutaneous involvement
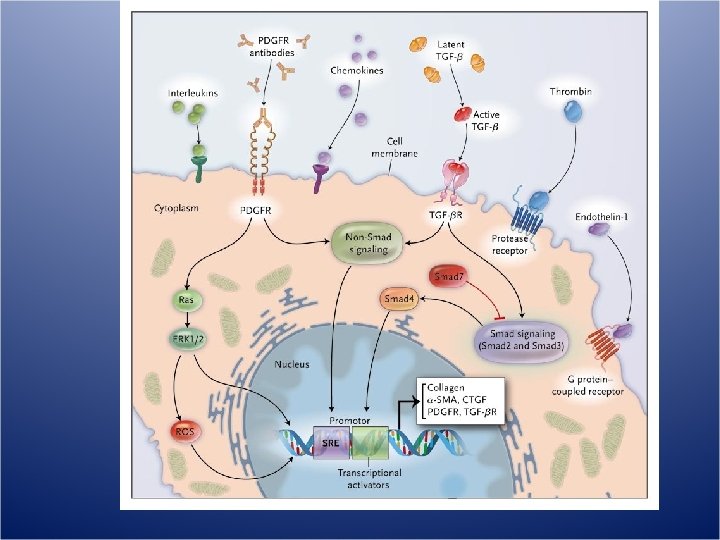
Fibrosis • Fibrosis gradually replaces vascular inflammatory phase and ultimately disrupts architecture of affected tissue 1. TGF-b 2. CTGF 3. PDGF
TGF b • Main Cell Source: macrophages, fibroblasts, T/B cells, platelets, endothelial cells • Pathogenic relevance: – Induces proliferation fibroblasts and production CTGF and endothirlin-1 – Stimulates synthesis collagen, fibronectin – Inhibits EC matrix degradation by reduced synthesis of MMP and induction of TIMP-1 • Effect in SCL – Increased levels in skin – Elevated expression/ phosphorylation of smad 2, 3 effectors of TGF b signaling pathway
Mechanism of Signal Transduction Mediated by Transforming Growth Factor {beta} (TGF-{beta}) Blobe G et al. N Engl J Med 2000; 342: 1350 -1358
CTGF • Cell source: fibroblasts, endothelial cells, smooth muscle cells • Pathogenic relevance: – induced by TGFb, IL-4, and VEGF – Induces proliferation and chemotaxis of fibroblasts and stimulates production of EC matrix • Effect in SCL – Elevated levels in serum – Incr gene expression in skin and in fibroblasts
PDGF • Cell source: platelets, macrophages, endothelial cells, fibroblasts • Pathogenic Relevance: – Mitogen and chemoattractant for fibroblasts – Induces syntehsis of collagen, fibronectin, proteoglycans, – Stimulates secretion of TGF b type I, MCP-1, IL-6 • Effect in SCL – Elevated expression PDGN in skin – Incr levels in BAL
Selective Up-Regulation of PDGFR by Fibroblasts in Scleroderma Tan F. N Engl J Med 2006; 354: 2709 -2711
SRC: Diagnosis • New/abrupt onset BP >150/85 • Progressive/sudden rise in creat • Additional findings – MAHA and thrombocytopenia – Acute retinal changes of malignant HTN – New onset proteinuria/ hematuria – Urine sediment is bland with limited but incr protein – MAHA/TMA – Characteristic changes on renal bx
Renal Biopsy Subintimal Fibrin Deposition – Interlobular artery Muscular Renal Artery – Onion Skin thickening with complete obliteration of vascular lumen
Fibrin Deposition
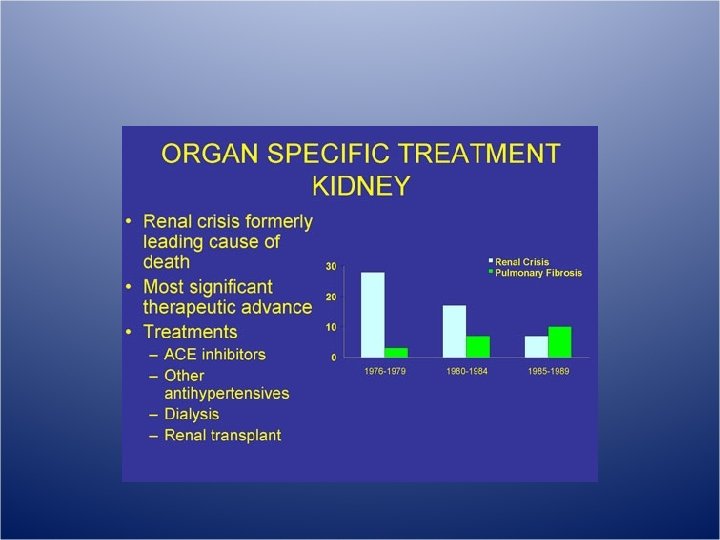
Prevention/Treatment • Prevention: avoidance glucocorticoids • If left untreated, SRC can progress to ESRD over 1 -2 months and death usually within 1 yr • Treatment: – Mainstay prompt control HTN, return to baseline bp in 72 hrs – Optimal anti-HTN is ACE-I ie captopril – Captopril? Advantage = rapid onset and short DOA allowing for more frequent titration – Also follow: plt count, LDH, Hb, haptoglobin, LDH for resolution of intravascular hemolysis – Indefinite continuation of ACE for bp control
ACE Inhibitors – Retrospective & case-control studies show no efficacy in prevention of SRC – Prospective cohort study- treated vs. untreated: treated w/↑ recovery of renal fxn & ↑ survival at 1 yr (76% vs 15%)
Long-term Outcomes of Scleroderma Reanl Crisis • Steen V, et al, Annals of Int Med, 2000 – Prospective observational cohort w 5 -10 yr f/u – 145 pts with SRC who received continuous ACE-I, and 662 pts with SCL who did not have renal crisis – Results: • At time of renal crisis, 75% pts had SCL sxs for <4 yrs • 61 % pts with SRC had good outcomes (55 received no HD, 34 received temp HD). Only 4% of later group progressed to ESRD • >1/2 of pts who began HD could dc it 3 to 18 mths later • Survival of pts in good outcome group was similar to pts with diffuse SCL without renal crisis
Autologous non-myeloablative hematopoietic stem cell transplantation in pts with systemic sclerosis • Burt RK, et al 2007 Bone Marrow Transplantation Phase I non-myeloablative autologous HSCT 10 pts with SSc and poor prognostic features PBCS mobilized with CY and G-CSF PBSC graft re-infused after tx with non-myeloablative conditioning regimen – statistically significant improvement of modified Rodnan skin score, however cardiac, pulmonary function, and creat remained unchanged – F/U: 25 mths, overall and progression free survival rates are 90 and 70% – Concl: Autologous HSCT with non-myeloablative conditioning regimen may lead to improved skin flexibility similar to a myeloablative TBI , but without the toxicity and risks – –