Schizophrenia Spectrum and Other Psychotic Disorders Dr Layali




 of the following, each present")






























 delusions with")



- Slides: 48
Schizophrenia Spectrum and Other Psychotic Disorders Dr. Layali Abbasi Psychiatrist Yarmouk University 5 th year/Faculty of Medicine September, 2017
Schizophrenia Spectrum and Other Psychotic Disorders DSM-5 Delusional Disorder Brief Psychotic Disorder Schizophreniform Disorder Schizophrenia Schizoaffective Disorder Substance/Medication-Induced Psychotic Disorder • Psychotic Disorder Due to Another Medical Condition • • •
Schizophrenia
• • • Eugen Beuler coined the term schizophrenia. Is a serious mental illness. Lifetime prevalence is about 1%. Is equally prevalent in men and women. The peak ages of onset are 10 to 25 years for men and 25 to 35 years for women.
DSM-5 Diagnostic Criteria for Schizophrenia A. Two (or more) of the following, each present for a significant portion of time during a 1 month period (or less if successfully treated). At least one of these must be (1), (2), or (3): 1. Delusions 2. Hallucinations 3. Disorganized speech (e g, frequent derailment or incoherence) 4. Grossly disorganized or catatonic behavior 5. Negative symptoms (i e, diminished emotional expression or avolition).
DSM-5 Diagnostic Criteria for Schizophrenia B. For a significant portion of the time since the onset of the disturbance, level of functioning in one or more major areas of functioning, such as work interpersonal relations, or self-care, is markedly below the level achieved before the onset (or when the onset is in childhood or adolescence, there Is failure to achieve expected level of interpersonal, academic, or occupational functioning).
DSM-5 Diagnostic Criteria for Schizophrenia C. Continuous signs of the disturbance persist for at least 6 months. This 6 -month period must include at least 1 month of symptom (or less if successfully treated) that meet Criterion A (i e , active-phase symptoms) and may include periods of prodromal or residual symptoms. During these prodromal or residual periods, the signs of the disturbance may be manifested by only negative symptoms or by two or more symptoms listed In Criterion A present in an attenuated form (e. g. , odd beliefs, unusual perceptual experiences).
DSM-5 Diagnostic Criteria for Schizophrenia D. Schizoaffective disorder and depressive or bipolar disorder with psychotic features have been ruled out because either (1) no major depressive or manic episodes have occurred concurrently with the active phase symptoms, or (2) if mood episodes have occurred during active-phase symptoms, they have been present for a minority of the total duration of the active and residual periods of the illness. E. The disturbance is not attributable to the physiological effects of a substance (e. g. , a drug of abuse, a medication) or another medical condition. F. if there is a history of autism spectrum disorder or a communication disorder of childhood onset, the additional diagnosis of schizophrenia is made only if prominent delusions or hallucinations, in addition to the other required symptoms of schizophrenia, are also present for at least 1 month (or less if successfully treated).
Positive symptoms of psychosis and schizophrenia
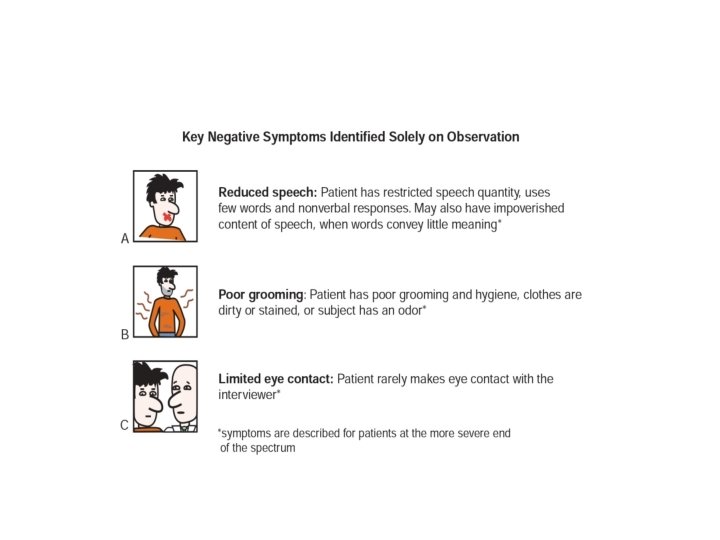
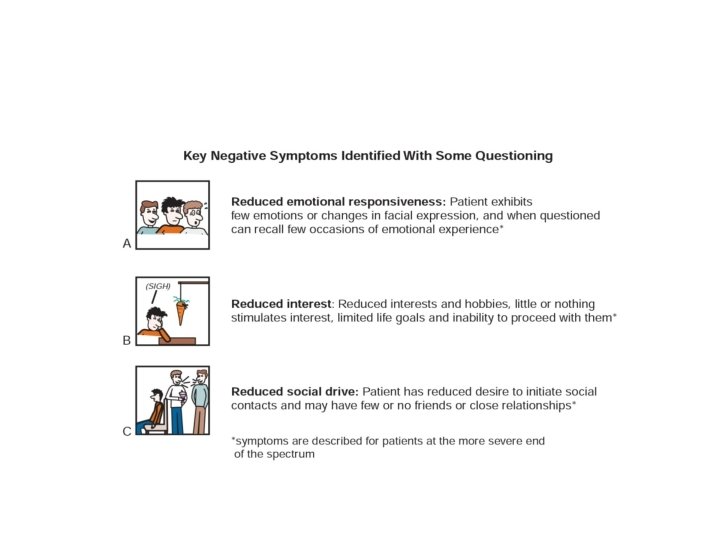
Negative symptoms of schizophrenia
What are negative symptoms?
Cognitive symptoms of schizophrenia
Etiology • Genetic factors: -Concordance rate for monozygotic twins is approximately 50%. -First-degree biological relatives of persons with schizophrenia have a ten times greater risk for developing the disease than the general population. -In a family with one parent diagnosed with schizophrenia, children have a 12% risk of schizophrenia.
• Biochemical factors -Dopamine Hypothesis -Serotonin -GABA -Glutamate
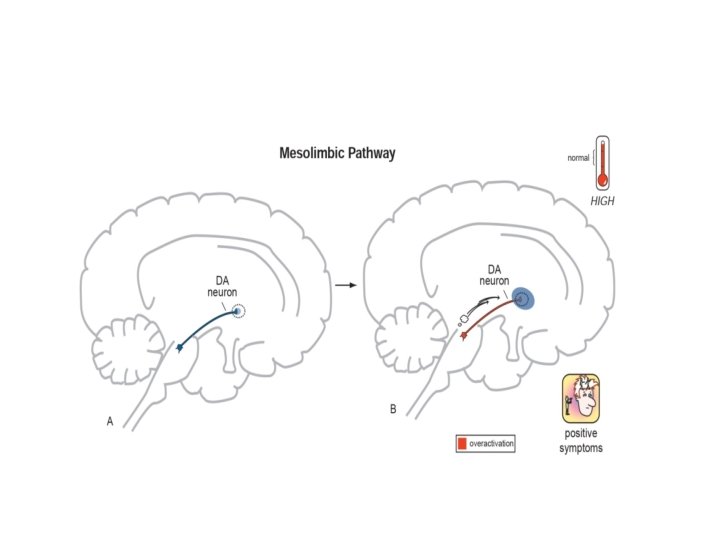
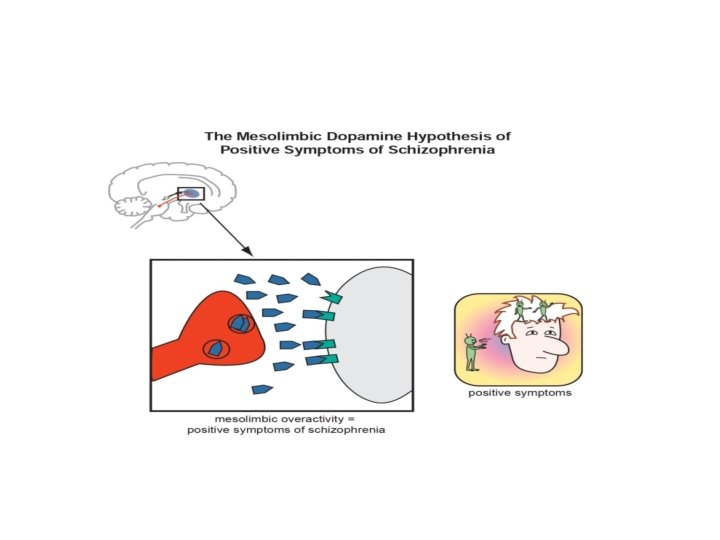
The dopamine hypothesis of schizophrenia
Key dopamine pathways in the brain • • • Mesolimbic dopamine pathway. Mesocortical dopamine pathway. Nigrostriatal dopamine pathway. Tuberoinfundibular dopamine pathway. Thalamic dopamine pathway.
The mesolimbic dopamine pathway and positive symptoms of schizophrenia • Projects from dopaminergic cell bodies in the ventral tegmental area of the brainstem to axon terminals in one of the limbic areas of the brain, namely the nucleus accumbens in the ventral striatum. • This pathway is thought to have an important role in several emotional behaviors, including the positive symptoms of psychosis, such as delusions and hallucinations. The mesolimbic dopamine pathway also is important for motivation, pleasure, and reward.
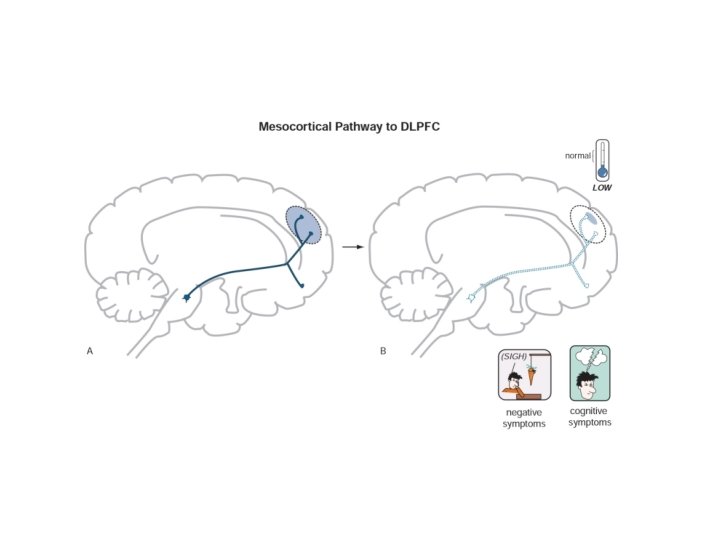
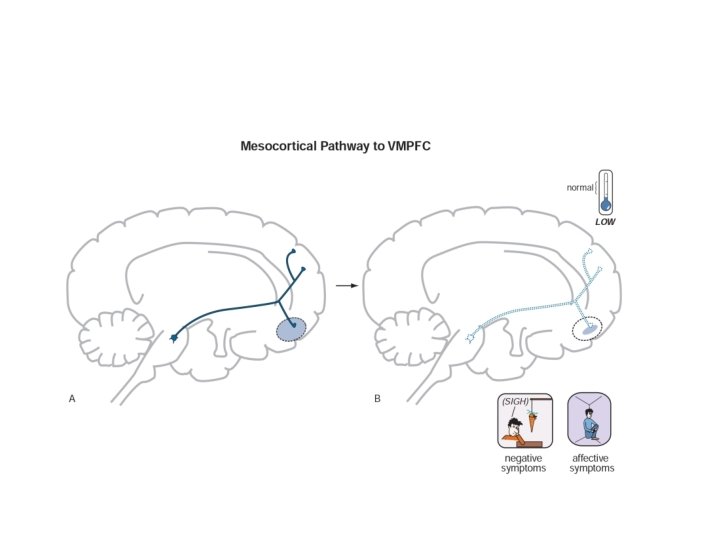
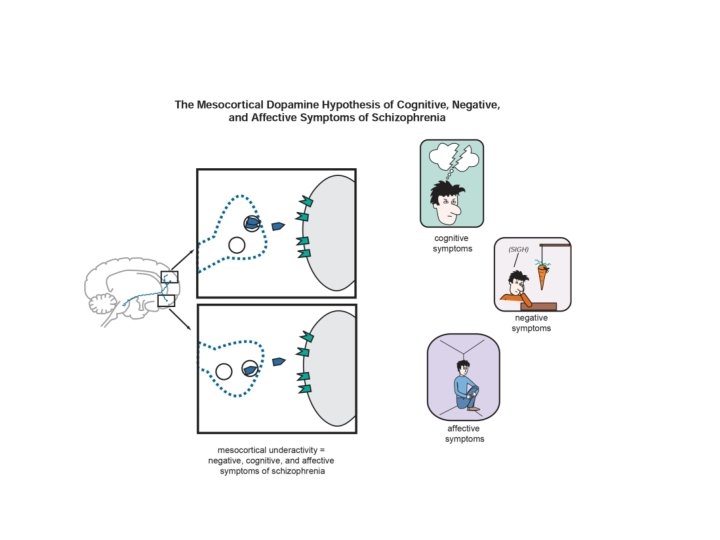
The mesocortical dopamine pathway and cognitive, negative, and affective symptoms of schizophrenia • Projects from dopaminergic cell bodies in the ventral tegmental area of the brainstem to areas of the prefrontal cortex. • Branches of this pathway into the dorsolateral prefrontal cortex are hypothesized to regulate cognition and executive functions, whereas branches of this pathway into the ventromedial parts of the prefrontal cortex are hypothesized to regulate emotions and affect.
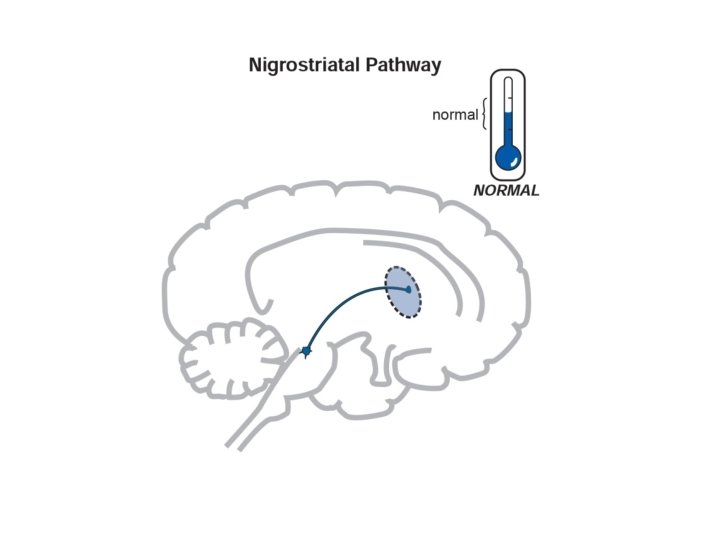
Nigrostriatal dopamine pathway • Projects from dopaminergic cell bodies in the brainstem substantia nigra via axons terminating in the basal ganglia or striatum. • In untreated schizophrenia, activation of this pathway is believed to be “normal. ” • When dopamine is deficient, it can cause parkinsonism with tremor, rigidity, and akinesia/bradykinesia. • When DA is in excess, it can cause hyperkinetic movements such as tics and dyskinesias.
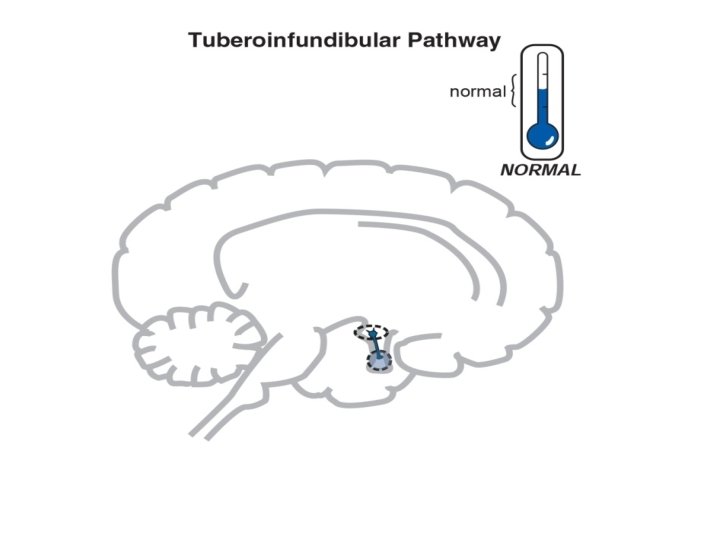
Tuberoinfundibular dopamine pathway • Projects from the hypothalamus to anterior pituitary. • Normally, these neurons are active and inhibit prolactin release • Dopamine inhibits prolactin secretion. • In untreated schizophrenia, activation of this pathway is believed to be “normal. ”
Serotonin hypothesis • An excess of serotonin can induce psychotic symptoms. Supporting this hypothesis is the finding that hallucinogens acting as partial 5 -HT 2 A receptor agonists (e. g. , lysergic acid diethylamide (LSD) ) can produce psychotic symptoms indistinguishable from those of the active phase of schizophrenia.
Glutamate • Glutamate has been implicated because ingestion of phencyclidine, a glutamate antagonist, produces an acute syndrome similar to schizophrenia.
• Neuropathology -Lateral and third ventricular enlargement. -Reduced symmetry in several brain areas, including the temporal, frontal, and occipital lobes. -Decreased size of the hippocampus.
Suicide • Is the single leading cause of premature death among people with schizophrenia. • Suicide attempts are made by 20 to 50 % of the patients, with long term rates of suicide estimated to be 10 to 13 %. • According to DSM-5, approximately 5 to 6 % of schizophrenic patients die by suicide. • The most important factor is the presence of major depressive disorder. • Epidemiological studies indicate that up to 80 percent of schizophrenia patients may have a major depressive episode at some time in their lives.
Suicide • Patients with the best prognosis (few negative symptoms, preservation of capacity to experience affects, better abstract thinking) can paradoxically also be at highest risk for suicide. • Other possible contributors to the high rate of suicide include command hallucinations and drug abuse. • Clozapine may have particular efficacy in reducing suicidal ideation in schizophrenia patients with prior hospitalizations for suicidality. • Adjunctive antidepressant medications have been shown to be effective in alleviating co-occurring major depression in schizophrenia.
Homicide • Despite the sensational attention that the news media provides when a patient with schizophrenia murders someone, the available data indicate that these patients are no more likely to commit homicide than is a member of the general population. • When a patient with schizophrenia does commit homicide, it may be for unpredictable or bizarre reasons based on hallucinations or delusions. • Possible predictors of homicidal activity are a history of previous violence, dangerous behavior while hospitalized, and hallucinations or delusions involving such violence.
Prognosis Factors Good prognosis Poor prognosis Gender Female Male Prodromal functioning Good Poor Symptom onset Acute Gradual Precipitating stressor Present Absent Symptom profile Predominantly positive symptoms Predominantly negative symptoms Presence of mood symptoms Yes No (blunted affect) Family history of mood disorders Yes No Family history of schizophrenia No Yes
Prognosis Factors Good prognosis Poor prognosis Onset Later in life Earlier in life Interepisode functioning Good Poor Duration of active-phase symptoms Short Long Residual symptoms Minimal Many Insight into having an illness Good Poor Support system Good Poor Substance use Absent Present
Schizophreniform Disorder • Is an acute psychotic disorder that has a rapid onset and lacks a long prodromal phase. • The initial symptom profile is the same as that of schizophrenia in that two or more psychotic symptoms must be present. • An episode of the disorder last at least one month but less than 6 months. • Although many patients may experience functional impairment at the time of an episode, they are unlikely to report a progressive decline in social or occupational functioning.
Schizophreniform Disorder Course and prognosis • The real issue is what happens to persons with this illness over time. • Most estimates of progression to schizophrenia range between 60 and 80 percent. What happens to the other 20 to 40 percent is currently not known. Some will have a second or third episode during which they will deteriorate into a more chronic condition of schizophrenia. A few, however, may have only this single episode and then continue on with their lives.
Brief Psychotic Disorder • Is a psychotic condition that involves the sudden onset of psychotic symptoms, which lasts one day but less than one month. • Remission is full, and the individual returns up the premorbid level of functioning.
Good Prognostic Features for Brief Psychotic Disorder: Good premorbid adjustment. Few premorbid schizoid traits. Severe precipitating stressor. Sudden onset of symptoms. Affective symptoms. Confusion and perplexity during psychosis Little affective blunting. Short duration of symptoms. Absence of relatives with schizophrenia.
DSM-5 Diagnostic Criteria for Schizoaffective Disorder A. An uninterrupted period of illness during which there is a major mood episode (major depressive or manic) concurrent with Criterion A of schizophrenia. Note: The major depressive episode must include Criterion A 1: Depressed mood. B. Delusions or hallucinations for 2 or more weeks in the absence of a major mood episode (depressive or manic) during the lifetime duration of the illness. C. Symptoms that meet criteria for a major mood episode are present for the majority of the total duration of the active and residual portions of the illness. D. The disturbance is not attributable to the effects of a substance (e. g. , a drug of abuse, a medication) or another medical condition.
Schizoaffective Disorder Epidemiology • The lifetime prevalence is less than 1%, possibly in the range of (0. 5 to 0. 8 %)
Schizoaffective Disorder Prognosis • Patients with schizoaffective disorder have a better prognosis than patients with schizophrenia and a worse prognosis than patients with mood disorders.
Delusional Disorder DSM-5 Diagnostic Criteria A. The presence of one (or more) delusions with a duration of 1 month or longer. B. Criterion A for schizophrenia has never been met. Note: Hallucinations, if present, are not prominent and are related to the delusional theme (e. g. , the sensation of being infested with insects associated with delusions of infestation). C. Apart from the impact of the delusion(s) or its ramifications, functioning is not markedly impaired, and behavior is not obviously bizarre or odd. D. It manic or major depressive episodes have occurred, these have been brief relative to the duration of the delusional periods. E. The disturbance is not attributable to the physiological effects of a substance or another medical condition and is not better explained by another mental disorder, such as body dysmorphic disorder or obsessive compulsive disorder.
Delusional Disorder Epidemiology • Is much rarer than either schizophrenia and the mood disorders. • The mean age of onset is about 40 years. • A slight preponderance of female patients exists. • Men are more likely to develop paranoid delusions than women, who are more likely to develop delusions of erotomania. • Many patients are married and employed.
Delusional Disorder Good prognostic factors • High levels of occupational, social, and functional adjustments. • Female sex. • Onset before age 30 years. • Sudden onset. • Short duration of illness. • The presence of precipitating factors.
THE END