SCHIZOPHRENIA Dr Nadira Khamker Senior Consultant Department Psychiatry



 Eugen Bleuler ( 1857 -1939) “Dementia")













 Thought withdrawal Thought insertion Thought broadcasting Thought control")



 Affective blunting / flat affect Alogia –relative absence in amount/ content")



 Irrelevant")




















- Slides: 50
SCHIZOPHRENIA Dr Nadira Khamker Senior Consultant Department Psychiatry Weskoppies Hospital University of Pretoria , Faculty of Health & Science
SCHIZOPHRENIA Schizophrenia is a psychiatric disorder with unknown aetiology. It is characterized by psychotic symptoms which incapacitate the patient’s level of functioning. It is a chronic condition with a prodromal, acute and residual phase, or remission.
Psychosis ? ill-defined, generic term Lack of insight is a core feature Delusions and hallucinations are often present
History of schizophrenia Emil Kraepelin ( 1856 -1926) Eugen Bleuler ( 1857 -1939) “Dementia precox” Bleuler coined the term “schizophrenia”
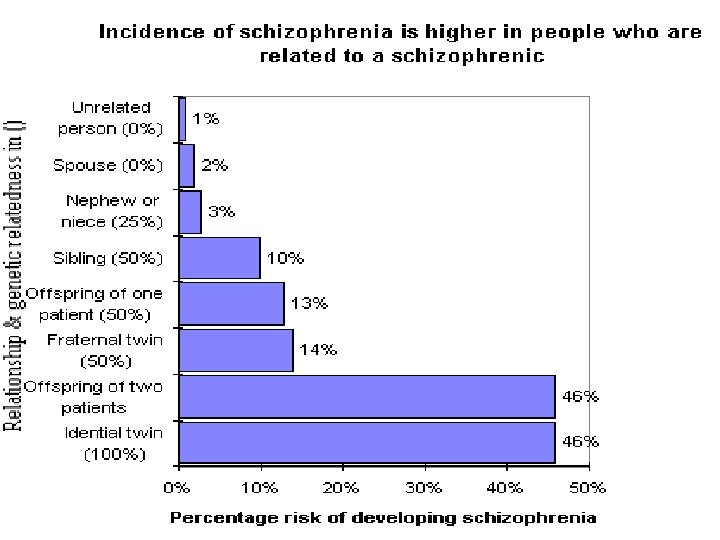
Epidemiology 0, 5 -1% of population Genetic predisposition Women=men Women : mean age of 1 st episode is 26, 8 years Men : mean age of 1 st episode is 21, 4 years
Epidemiology contd Genetic factors- 10 x ↑ risk in persons with 1 st degree relatives for developing the disease. Medical illnesses- c – comorbid conditions , – upto 50% may be undiagnosed Substance abuse- – common in schizophrenia, – association between cannabis and schizophrenia Infection and Birth Season
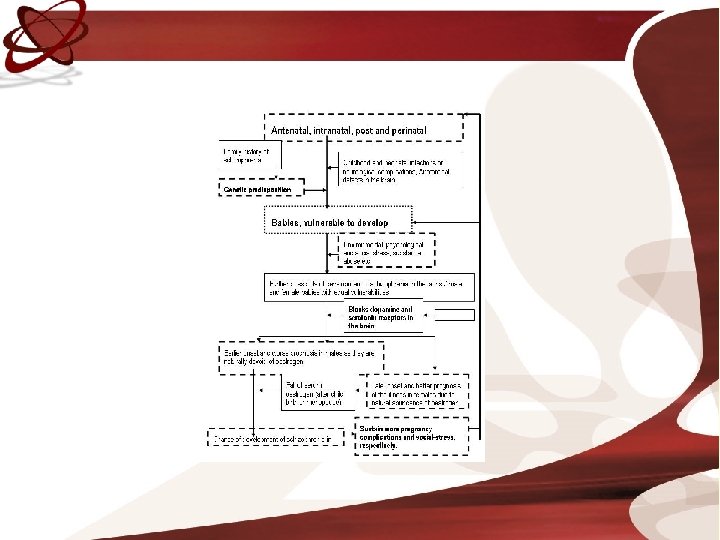
Aetiology Unknown Diathesis-vulnerability Eco-genetic factors Dopaminergic hypothesis
CLINICAL FEATURES POSITIVE SYMPTOMS NEGATIVE SYMPTOMS COGNITIVE SYMPTOMS AFFECTIVE SYMTOMS AGGRESSIVE SYMPTOMS
Symptom clusters Reality distortion Psychomotor poverty Disorganisation Cognitive domain
POSITIVE SYMPTOMS NEGATIVE SYMPTOMS COGNITIVE SYMPTOMS REALITY DISTORTION PSYCHMOTOR POVERTY DISORGANISATION DELUSIONS LACK OF AFFECTIVE RESPONSIVENESS INAPPROPRIATE AFFECT HALLUCINATIONS LOSS OF DRIVE OR VOLITION INCOHERENT SPEECH POVERTY OF SPEECH AND MOVEMENT DISORGANISED BEHAVIOUR SOCIAL WITHDRAWAL
Reality distortion Hallucinations Delusions
Hallucination : definition False sensory perception not associated with real external stimuli; there may or may not be a delusional interpretation of the hallucinatory experience. Auditory, visual, olfactory, tactile and somatic hallucinations.
Hallucinations in Schizophrenia Ask the patient if he / she is hearing voices, other people can’t hear and ask in detail about the quality, frequency, intensity and reaction towards these voices
Delusions : definition False, fixed belief, based on incorrect inference about external reality, not consistent with patient’s intelligence and cultural background; cannot be corrected by reasoning. Somatic, paranoid ( persecutory and of reference), erotomania, of control / poverty/self-accusation
Delusions Overvalued idea is NOT a delusion but an unreasonable, sustained false belief maintained less firmly than a delusion. Bizarre delusion is absurd and implausible Nihilistic delusion is the false feeling that self, others or the world is nonexistent or coming to an end
Delusions of poverty : they believe they are bereft or will be deprived from all property Somatic delusions: involving body (brain is rotting) Persecutory delusions: being harassed, cheated, or percecuted Delusion of grandeur: exaggerated concept of power or intelligence
Delusions of reference: the behaviours of others refers to them, people are talking about him / her. Delusions of self-accusation: feelings of remorse and guilt. Delusions of control: their thoughts, will or feelings are controlled by external forces
Delusions of control (bizarre) Thought withdrawal Thought insertion Thought broadcasting Thought control
Form of thought disturbances Neologism : new words by combining syllabes Word salad: inhorent mixture of words Perseveration: persisting response to previous stimulus Verbigaration: meaningless repetition of words Echolalia: repeating of words Blocking: abrupt interruption in train of thinking
Thought content in schizophrenia Delusions Preoccupation Ideas of reference and influence phobias Poverty of content Obsessions and compulsions Suicidal or homicidal ideas
Psychomotor poverty Lack of affective responsiveness Loss of drive or volition Poverty of speech and movement Social withdrawal
Negative symptoms(5 As) Affective blunting / flat affect Alogia –relative absence in amount/ content of speech Avolition-inability to initiate and persist in activities Anhedonia-loss of enjoyment for activities Attention impaired
Disorganisation Inappropriate affect Disorganised behaviour
Grossly disorganized or catatonic behavior Aggressive, violent outbursts Bizarre clothing appearance Inappropriate social / sexual behavior Catatonic behavior , ranging from extreme excitement to stupor
Cognitive domain Impaired attention and concentration Impaired memory and learning Impaired executive functioning ( e. g. abstract thinking, problem solving)
Disorganized speech Disturbance in form of thought: Circumstantiality ( delays in reaching answer) Irrelevant answer Derailment (deviates from train of thought) Tangentially( never gets back to desired goal) Loosening of associations(shift in unrelated manner) Incoherence(thoughts not understandable)
SCHIZOPHRENIA: SYMPTOLOGY DSM IV CRITERIA A : TWO OR MORE OF THE FOLLOWING: Delusions Hallucinations Disorganized speech Grossly disorganized behavior Negative symptoms Present for at least one month
CRITERIA A If the delusion is bizarre, only one of the A Criteria is required. For example if you believe the microchip in your front tooth controls world’s events A voice keeping up a running commentary on the person’s behavior or thoughts or…. . Two or more voices conversing with each other.
DIAGNOSIS B. C D E Social and occupational dysfunction Duration Exclusion criteria Substance abuse
Schizophrenia sub types Paranoid Catatonic Residual Undifferentiated Disorganized
CLINICAL FEATURES No symptom or sign is definitive for schizophrenia Careful history important as symptoms change with time Premorbid symptoms and signs appear before the prodromal phase Patients may have shcizoid or schizotypal personalities May be quiet, passive and introverted children Few friends, solitary activities May present with somatic complaints Family and friends may notice changes in social, occupational, personal activities May then present with peculiar behaviour, abnormal affect, unusual speech, bizarre ideas, perceptual disturbances
MENTAL STATE EXAMINATION GENERAL APPEARANCE AND BEHAVIOUR – May be unkempt, poor self-care – Psychomotor activity SPEECH – Monotonous, poverty of speech – Disorganised speech MOOD AND AFFECT – Reduced emotional responsiveness – Inappropriate emtions PERCEPTUAL DISTURBANCES – Hallucinations THOUGHT FORM DISTURBANCES – Loosening of associations – Tangentiality THOUGHT CONTENT DISTURBANCE Delusions IMPULSIVENESS, VIOLENCE, SUICIDE, HOMICIDE SENSORIUM AND COGNITION – Memory, JUDGEMENT AND INSIGHT
Good prognosis in schizophrenia Obvious precipitating factors Acute onset Good premorbid history / later onset Mood symptoms or family history of moodsx Married and / or good support system Positive symptoms
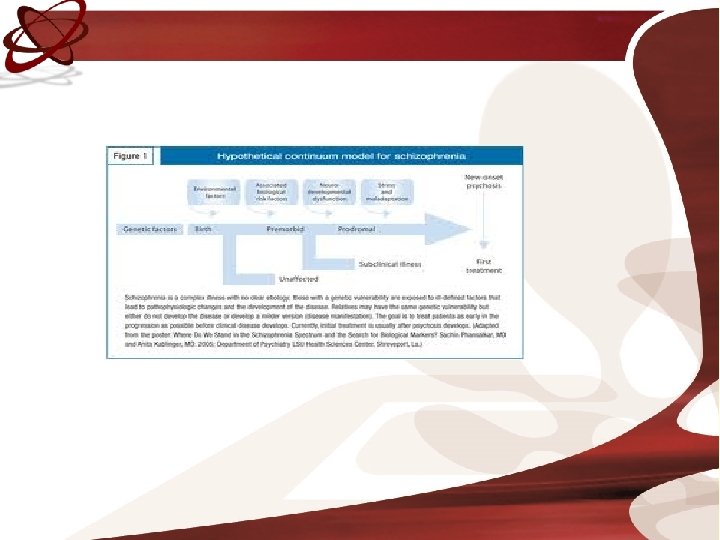
Longitudinal course Symptoms start in adolescence Prodromal symptoms may last for 1 year Exacerbations and remissions Baseline functioning deteriorates Positive symptoms less severe with age but negative symptoms may increase in severity
Chronic illness Premorbid symptoms Relapsing and remitting course Deterioration in functioning over time
Course and prognosis 10 -20% suffer one episode and remain symptom free 60% follow a course of relapses and remissions, of which half achieve full remission and half partial remission.
Indications for referral Frequent relapses Resistance to treatment Co-morbid conditions Lack of sufficient support / resources at primary level
Psychoeducation It is a biological disease of the brain The precise etiology is unknown Genetic vulnerability Environmental factors Long-term treatment Rehabilitation necessary
Psychological interventions Cognitive behavioural therapy Psychoeducation Family therapy Social skills training
Social interventions Halfway houses / step down facilities Supervised group houses Unsupervised houses Day centres Supported employment Disability grants
Other Psychotic Disorders Psychotic disorders due to GMC Substance-induced psychotic disorders Shared psychotic disorder Psychotic disorder not otherwise specified Delusional disorder Schizophreniform disorder Schizoaffective disorder Brief Psychotic Disorder
Compared with schizophrenia Sx <1 month = brief psychotic disorder ……………. . >1<6 months= Schizophreniform ……………. . >6 months= schizophrenia
Delusional disorder Nonbizarre delusions No marked impairment in functioning Types include: erotomania, grandiose, jealous, persecutory, somatic and mixed
Schizoaffective disorder Substantial period of illness also mood symptoms Bipolar type versus depressive type Better prognosis than schizophrenia
Differential diagnosis of PSYCHOTIC symptoms Substance-related disorders Epilepsy- TLE Cerebral tumours / trauma AIDS, Neurosyphilis, herpes encephalitis Porphyria SLE, Wilson’s disease, B 12 deficiency
Conclusion Psychotic disorders cause extreme distress and diability over periods of time Disorder is treatable and relapses can be limited Primary health care worker has an important role to play