Schizophrenia A severe mental condition in which there









 or waking")
 • loose association or derailment: slips from")
 – Child like silliness to unpredictable agitation")



 v. Disturbed")



 – Mannerism:")
 – Rigidity:")


 • Hallucinations • Delusions Disorganized • Disorganized speech")










- Slides: 37
Schizophrenia
A severe mental condition in which there is disorganization of the personality, deterioration in social functioning, and loss of contact with, or distortion of, reality. There may be evidence of hallucinations and delusional thinking. Psychosis can occur with or without the presence of organic impairment.
Schizophrenia Spectrum and Other Psychotic Disorders Schizotypal personality disorder Delusional Disorder Brief Psychotic disorder Schizophreinform Disorder Schizophrenia Schizoaffective disorder Substance / medication – induced psychotic disorder Psychotic disorder due to another medical condition Catatonia
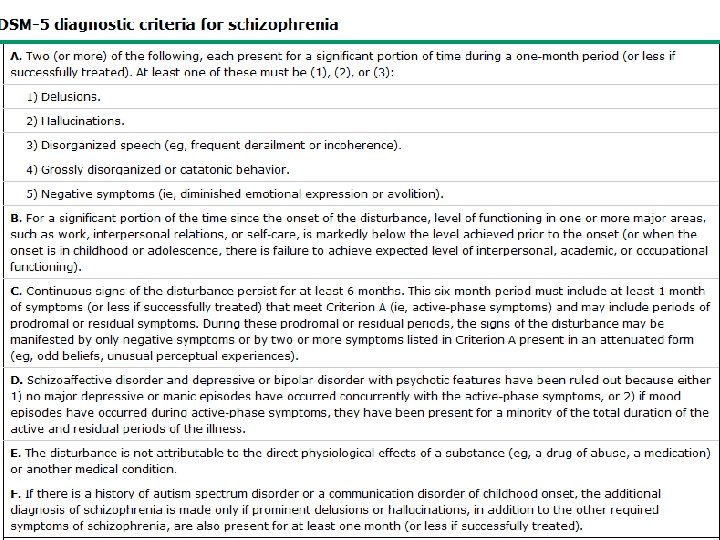
Diagnostic Criteria A. Two or more of the following almost all day most days of the month: at least one of these must be 1, 2, or 3 1. Delusions – Bizarre delusions such as: – Example » A person’s belief that a stranger has removed his or her internal organs and has replaced it with someone else’s organs without leaving any wounds or scars • • • Thought broadcasting Thought insertion Delusion of being controlled Thought withdrawal Paranoid delusions
Delusion Types • Persecutory delusion: the person believes he or she is being tormented, followed, tricked, spied on, or ridiculed. • Referential delusions: the person believes certain gesture, comments, passage from a book, newspapers, songs or other environmental cues are specially directed towards him or her • Thought broadcasting • The person believes that his thoughts are being broadcasted by TV, Radio, or being read by other people
Delusion Types • Thought withdrawal: a person’s belief that his or her thought have been taken away by some outside force (or stolen) • Thought insertion: alien thoughts have been put into his or her mind (thoughts are implanted in their minds from outside source) • Delusion of being controlled: the person’s body or actions are being acted upon or manipulated by some outside force
Delusion Types • Erotomanic: With this type of delusion, the individual believes that someone, usually of a higher status, is in love with him or her. • Grandiose: Individuals with grandiose delusions have irrational ideas regarding their own worth, talent, knowledge, or power. • Somatic: Individuals with somatic delusions believe they have some physical defect, disorder, or disease.
Delusion Types • Jealousy: The content of jealous delusions centers on the idea that the person’s sexual partner is unfaithful. • Nihilistic: The individual has a false idea that the self, a part of the self, others, or the world is nonexistent (e. g. , “The world no longer exists, ” “I have no heart. ”). • Mixed
Diagnostic Criteria 2. Hallucinations: are perception like experiences that occur without an external stimuli. • They are vivid and clear • With full force and impact of normal perceptions, and not under voluntary control • Mostly auditory – Two talking about the patient as a third person, – Voices conversing together – One voice running commentaries on the patient’s thoughts or behaviors
Diagnostic Criteria • Note: Those hallucination that occur while falling asleep (hypnagogic) or waking up (hypnopompic) are considered within normal. Hallucination may be a normal part of religious experience in certain cultural contexts. • Types of Hallucination 1. Auditory: are false perceptions of sound or voices 2. Visual: These are false visual perceptions. 3. Gustatory: are false perceptions of the sense of touch, often of something on or under the skin. 4. Tactile: This type of hallucination is a false perception of taste. 5. Olfactory: are false perceptions of the sense of smell.
Diagnostic Criteria 3. Disorganized Speech: (impaired communication) • loose association or derailment: slips from the track from one topic to another • Answers to questions obliquely related or completely unrelated (Tangentiality, circumstantiality) • Incoherent or ward salad, neologisms
Diagnostic Criteria 4. Odd behaviors (disorganized behavior) – Child like silliness to unpredictable agitation – May be noted in any form of goal-directed behaviors, leading to difficulties in performing ADL, such as maintaining hygiene, the person may dress in an unusual manner (wearing multiple overcoats, scarves, and gloves in a hot day) – Inappropriate sexual behavior (masturbation in public) – Unpredictable and un-triggered agitation (shouting and swearing) – Strange grimaces, sniffing, blowing out cheeks, wrinkling the forehead, or ritualistic activities– – Mannerism or catatonic--stupor, negativism, rigidity, excitement, waxy flexibility, or posturing – – Immobility, adopting odd postures for long periods of time.
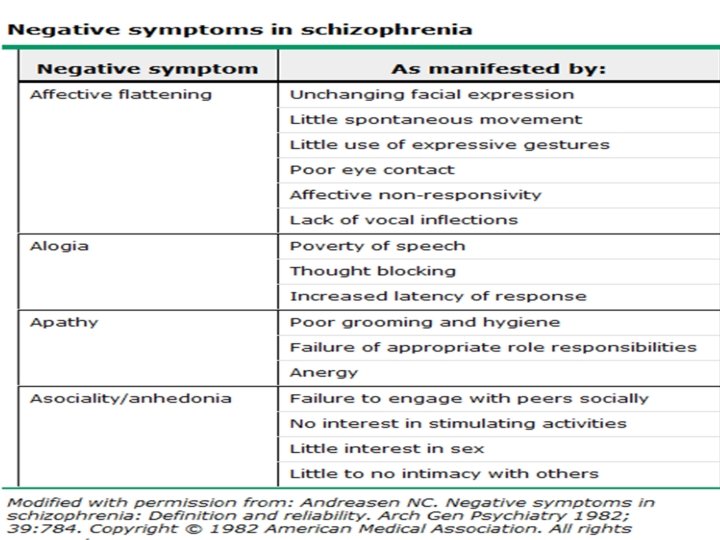
Diagnostic Criteria 5. Negative symptoms: – Affective flattening (face immobile, unresponsive, poor eye contact, and reduce and language) – Alogia (poverty of speech lacks content, diminshed ) – Avolition (inability to initiate and persist in goal directed activities) absence of interest in usual routines (grooming, hygiene – Anhedonia-inability to experience pleasure (relationships, sex) – Asociality: refers to the apparent lack of interest in social interaction
Diagnostic Criteria v B. Social Occupational Dysfunction: v Marked deterioration in role functioning in one or more of major areas; work or school, interpersonal relations, self care activities. v. C. Duration: v. Continuous signs persist for at least 6 months. (includes at least one month of acute symptoms, the other period there will be prodromal signs)
Diagnostic Criteria D. Exclusion of affective disorders v if affective disorder occur during acute period. it’s period of presence must be short as related to the acute period. E. Exclusion to any medical or drug use disorder v. Such as Alcohol, Cocaine, LSD, Anesthesia, Anti. Cholinergic agents, Chemotherapy, Carbon monoxide, Volatile substances such as Fuel and Paint F. Not related to any developmental disorder vsuch as autistic disorder.
Associated Features with Schizophrenia v. Inappropriate affect v. Dysphoria Mood (depressed, anxiety) v. Disturbed sleep pattern v. Lack of interest in eating or food refusal v. Depresonalization v. Derealization v. Somatic concern (Delusional proportions) v. Anxiety and Phobias are common v. Deficits in memory (working)
Associated Features with Schizophrenia v. Deficits in language functions v. Abnormalities in sensory processing and inhibitory capacity v. Reduction in attention v. Social cognition deficits (inability to infer the intentions of other people) v. Lack of insight v. Hostility and aggression
Functional Consequences of Schizophrenia v. Schizophrenia is associated with significant social or occupational dysfunction. v. Individuals with schizophrenia have impaired educational progress and are unable to maintain employment (due Avolition or other symptoms) v. Most individuals are employed at a lower level than their parents. v. Most of them don’t marry or have limited contacts outside of their family.
CATATONIA • The clinical picture is dominated by three or more of the following symptoms: • One or two of the following symptoms are present for at least two weeks: – Stupor: (marked decrease in reactivity to the environment the person might seem as in coma but still aware about the environment). – Excitement (purposeless motor activity, not influenced by external environment). – Posturing (voluntary assumption and maintenance of inappropriate or bizarre positions) 21
CATATONIA – Negativism: (motiveless resistance to any attempt to move the patient) – Mannerism: (odd movement, goal directed ) – Stereotypy: (repetitive, abnormal frequent- not goal directed) – Agitation: not influenced by external stimuli – Echolalia: mimicking another speech – Echopraxia: mimicking another movement • Tends to be severe and quite rare 22
CATATONIA – Posturing: (spontaneous and active maintenance of a posture against gravity) – Rigidity: (maintenance of rigid posture against efforts to be moved) – Waxy flexibility: Slight resistance to positioning by examiner – Catalepsy: (Passive induction of a posture held against gravity – Mutism: (No or very little verbal response exclude aphasia. 23
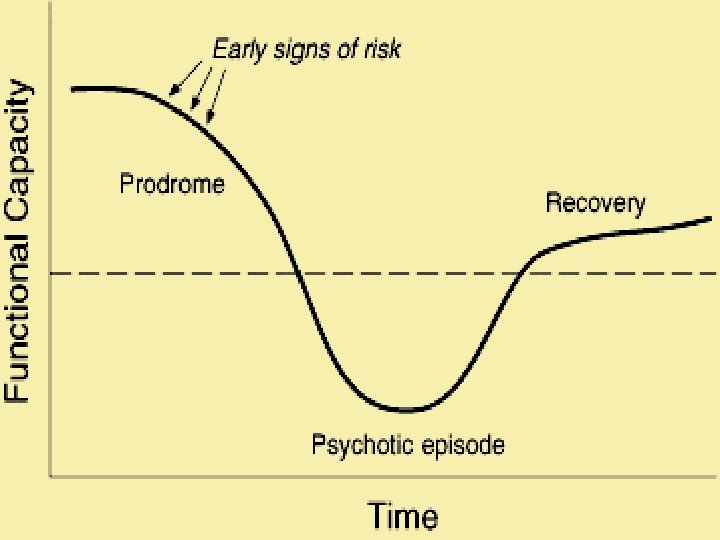
Schizophrenia: Phases • Phase I: Schizoid personality – Emotional coldness (limited range of emotional expression), Do not enjoy relationships, prefers solitary activities – Not all client who develop schizophrenia has schizoid personality • Phase II: The prodromal phase – Social withdrawal, neglect of hygiene & grooming, blunted or inappropriate affect, bizarre ideas, lack of initiatives, interest or energy. – May last for many years (gradual onset)
Schizophrenia: Phases • Phase III: Schizophrenia – Acute episode of signs & symptoms • Phase IV: Residual phase – Periods of remission & exacerbation – Similar to prodromal phase
Symptoms of Schizophrenia Positive (Type I) • Hallucinations • Delusions Disorganized • Disorganized speech • Disorganized thought • Disorganized or catatonic behavior Negative (Type II) • Affect - blunted or flat • Alogia - little speech • Avolition • Anhedonia • Agnosia (inability to recognize familiar situations, persons, …) • Social withdrawal
Associated features • Acute onset • Normal pre-morbid functioning • No family history • Normal functioning during remission • Absence of intellectual impairment • Slow onset • Pre-morbid emotional problems • Family history • Chronic deterioration in social functioning • Intellectual impairments
Associated features • Normal CT • Cerebellar atrophy • Normal neuro • Abnormal psychological testing neuropsychological tests • Good response to antipsychotic medications • Poor response to antipsychotic medications
PREVALENCE • The lifetime prevalence of schizophrenia appears to be 0. 3% 0. 7%. • Schizophrenia occurs in 1 person from 1000 person in the society. • The psychotic features of schizophrenia usually emerge between the late teens and the mid-30 s. • The peak onset of schizophrenia is early to mid 20 s for males and in the late-20 s for females
RISK FOR SUICIDE • Approximately 5%-6% of individuals with schizophrenia die by suicide, about 20% attempt suicide on one or more occasions. • Suicidal behavior is sometimes in response to command hallucinations • High risk for young male with comorbid substance use. • Other risk factor include having depressive symptoms or feelings of hopelessness and being unemployed, and the risk is higher, also, in the period after psychotic episode or hospital discharge.
OTHER PSYCHOTIC DISORDERS: SCHIZOPHRENIFORM • Two or more of the following, each present for a significant portion of time during a 1 month period. At least one of these must be (1), (2), or (3) • Prodromal, acute, & residual occur at least for one month & less than 6 months • Specify: – Without good prognostic feature – With good prognostic features Ø Onset of prominent psychotic symptoms within 4 weeks of the first noticeable change in usual functioning Ø Confusion or perplexity at the height of the psychotic episode Ø Good pre-morbid personality Ø Absence of blunted affect
OTHER PSYCHOTIC DISORDERS: SCHIZOAFFECTIVE DISORDER • Uninterrupted period of illness during which the person shows symptoms of mood disorder (depression or mania or mixed) concurrent with Criterion A of schizophrenia • During the period of illness the person has delusions or hallucinations at least 2 weeks in the absence of a major mood episode (manic or depressive) • The person experience symptoms of mood disorder that is relatively brief compared to the total duration of delusion or hallucination episodes • Exclude physical disorder or substance use • Specify: – Bipolar type – Depressive
OTHER PSYCHOTIC DISORDERS: Delusional disorder • A. the presence of one or more delusions with a duration of 1 month or longer. • B. Criterion A for schizophrenia has never been met • C. Functioning is not markedly impaired, and behavior is not obviously bizarre or odd • D. if manic or depressive episodes have occurred, these have been brief and relative to the duration of the delusional periods. • E. the disturbance is not attributable to the physiological effects of a substance or another medical condition and is not better explained by another mental disorder.
Other psychotic disorders: Delusional disorder • Delusions involve situation that occur in real life and has a specific theme such as: – – – Erotomanic Grandiose Jealousy Persecutory Somatic – Mixed
OTHER PSYCHOTIC DISORDERS: Brief psychotic Disorder • Presence of 1 or more of the following symptoms. At least one of these must be (1), (2), or (3). – – Delusion Hallucination Disorganized speech Grossly disorganized or catatonic behavior • Duration of an episode is at least 1 day but less than 1 month with full return to normal function level • Exclude other psychiatric disorders, substance use or physical problems • Specify: – With marked stressors (brief reactive psychosis) – Without marked stressor – With postpartum onset
Schizophrenia Co-morbid Conditions • • Depression Anxiety Aggression Substance use disorder 37