Scenario A 50 year old female has had











 remodel the bone by dissolving or resorbing")










, an 84 amino acid -long polypeptide")






 Vitamin D itself is inactive, it requires")




















 – Lowers Ca++ in the blood – Inhibits osteoclasts")





 a. Hyperparathyroidism b) b.")
- Slides: 59
Scenario A 50 year old female has had three vertebral fractures. She has also had a number of kidney stones. Routine labs revealed hypercalcemia.
Effects of Parathyroid Hormone on Bone Mineral Metabolism
Lecture Objectives At the end of the lecture students will be able to • Define the importance of calcium in bone mineral metabolism • Explain the action of Parathyroid Hormone on gut, bone and kidney. • Describe the role of 1, 25 -dihydroxy vitamin D and calcitonin in calcium homeostasis • List the symptoms of hyper and hypoparathyroidism
Physiological Importance of Calcium • Ca salts in bone provide structural integrity of the skeleton. • Ca ions in extracellular and intracellular fluids is essential for biochemical processes like: – Neuoromuscular excitability and signal transduction – Blood coagulation – Hormonal secretion – Enzymatic regulation – Neuron excitation
Three Forms of Circulating Ca 2+
Regulation of Calcium • The important role that calcium plays in so many processes dictates that its concentration, both extracellularly and intracellularly, be maintained within a very narrow range. • This is achieved by an elaborate system of controls
Calcium and phosphorous • Calcium is tightly regulated with Phosphorous in the body. • Phosphorous is an essential mineral necessary for ATP, c. AMP second messenger systems, and other roles • Ca 2+ normally ranges from 8. 5 -10 mg/dl in the plasma. • PO 4 normal plasma concentration is 3. 0 -4. 5 mg/dl.
Extracellular Calcium • When extracellular calcium falls below normal, the nervous system becomes progressively more excitable because of increase permeability of neuronal membranes to sodium. • Hyperexcitability causes tetanic contractions – Hypocalcemic tetany
Bone Composition
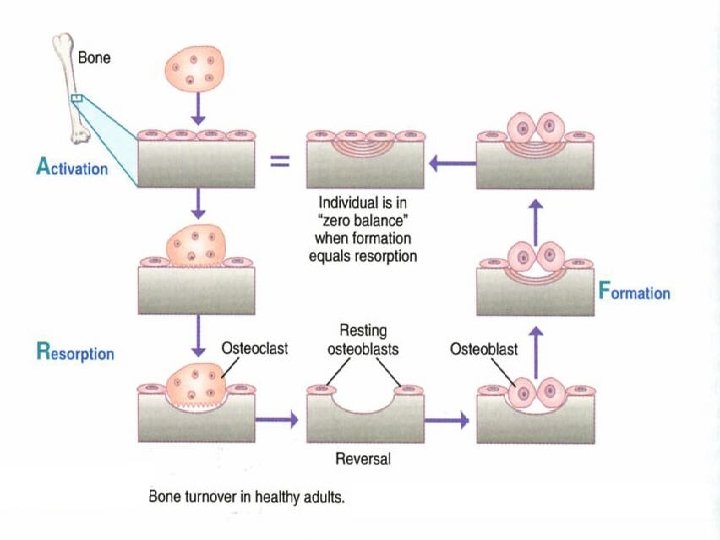
Bones • 99% of the Calcium in our bodies is found in our bones which serve as a reservoir for Ca++ storage. • 10% of total adult bone mass turns over each year during remodeling process • During growth rate of bone formation exceeds resorption and skeletal mass increases. • Once adult bone mass is achieved equal rates of formation and resorption maintain bone mass until age of about 30 years when rate of resorption begins to exceed formation and bone mass slowly decreases.
Bone cell types • Osteoclasts (bone cells) remodel the bone by dissolving or resorbing bone • Osteoblasts (bone forming cells) synthesize new bone to replace the resorbed bone - Found on the outer surfaces of the bones and in the bone cavities - Osteocytes the mature bone cells are enclosed in bone matrix.
Bone formation • Active osteoblasts synthesize and extrude collagen • Collagen fibrils form arrays of an organic matrix called the osetoid. • Calcium phosphate is deposited in the osteoid and becomes mineralized • Mineralization is combination of Ca. P 04, OH-, and H 3 CO 3– hydroxyapatite.
Osteoblast and Osteoclast Function Osteoblasts Osteoclasts • Bone formation • Synthesis of matrix protein • Mineralization • Bone resorption – Degradation of proteins by enzymes – Acidification
Calcium, bones and osteoporosis • The total bone mass of humans peaks at 25 -35 years of age. • Men have more bone mass than women. • A gradual decline occurs in both genders with aging, but women undergo an accelerated loss of bone due to increased resorption during perimenopause. • Bone resorption exceeds formation.
Calcium, bones and osteoporosis • Reduced bone density and mass: osteoporosis • Susceptibility to fracture. • Earlier in life for women than men but eventually both genders succumb. • Reduced risk: – Calcium in the diet – habitual exercise – avoid drinking carbonated soft drinks
Vertebrae of 40 - vs. 92 -year-old women Note the marked loss of trabeculae with preservation of cortex.
Calcium Homeostasis 1. 2. 3. Parathyroid Hormone Calcitonin 1, 25 -dihydroxy vitamin D
Calcium regulates PTH
Key Organs Involved • Gut • Bone • Kidneys
Parathyroid glands which are embedded in the thyroid tissues in many vertebrate species.
PARATHYROID HORMONE • A polypeptide secreted from the parathyroid glands in response to a decrease in the plasma concentration of ionized calcium
Parathyroid Hormone Structure • Parathyroid hormone (PTH), an 84 amino acid -long polypeptide
Regulation of PTH • PTH secretion responds to small alterations in plasma Ca 2+ within seconds. • An acute decrease of Ca results in marked increase of PTH m. RNA increase of PTH synthesis • PTH secretion also is stimulated by low levels of 1, 25 dihydroxy vitamin D
PTH increases Ca concentration by: 1: Action on the Bone Increased PTH secretion leads to an increase in bone resorption by stimulating osteoclasts and promotes the release of calcium and phosphate into the circulation
PTH increases Ca concentration by: 2: Action on the Kidney At the kidney, PTH acts to limit calcium excretion at the distal convoluted tubule via an active transport mechanism. It augments renal calcium reabsorption PTH also inhibits phosphate reabsorption (at the Proximal convoluted tubule) and bicarbonate reabsorption.
PTH and Kidney PTH acts on the distal tubule
PTH increases Ca concentration by: 3: Action on the Gut PTH also stimulates renal 1 - Hydroxylase activity, leading to an increase in 1, 25 -dihydroxy vitamin D, which Stimulates the absorption of Ca in the intestine
1, 25 -dihydroxy-Vitamin D 3 UV Cholesterol precursor 7 -dehydrocholesterol Vitamin D 3 25 Vitamin D 3 1, 25 Vitamin D 3 Low plasma Ca++ increase kidney enzymes
1, 25 -dihydroxy-vitamin. D 3 ( Calcitriol) Vitamin D itself is inactive, it requires modification to the active metabolite, 1, 25 -dihydroxy-D 3 is one of the principal regulator of Ca++. The first hydroxylation reaction takes place in the liver yielding 25 -hydroxy D 3. Then 25 -hydroxy D 3 is transported to the kidney where the second hydroxylation reaction takes place.
1, 25 -dihydroxy-vitamin D 3 promotes intestinal calcium absorption • 1, 25 -dihydroxy-D 3 acts via steroid hormone like receptor to increase transcriptional and translational activity • One gene product is calcium-binding protein (Ca. BP) • Ca. BP facilitates calcium uptake by intestinal cells • calbindin (calcium-binding protein) – regulated by the active form of vitamin D
1, 25 -dihydroxy-Vitamin D Actions on Bones • Another important target for 1, 25 -(OH)2 -D 3 is the bone. • Osteoblasts, but not osteoclasts have vitamin D receptors. • 1, 25 -(OH)2 -D 3 acts on osteoblasts which produce a paracrine signal that activates osteoclasts to resorb Ca++ from the bone matrix. • 1, 25 -(OH)2 -D 3 also stimulates osteocytic osteolysis.
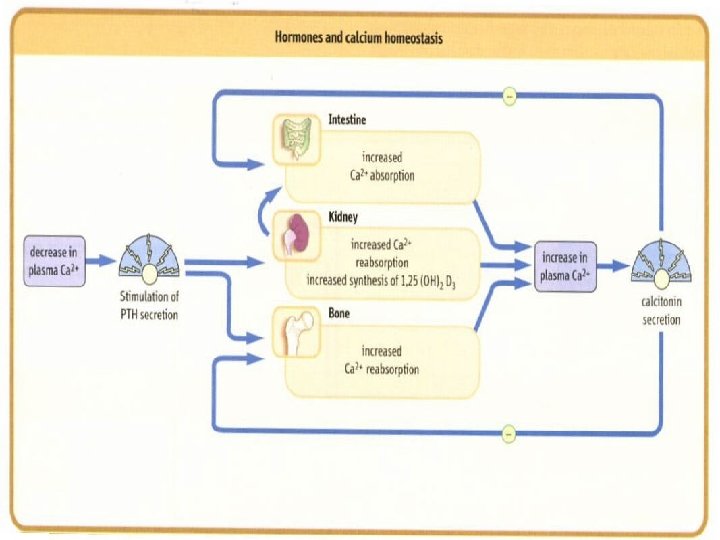
PTH functions to regulate calcium levels via its actions on three target organs, the bone, kidney, and gut.
Calcitonin Parathyroid glands Calcitonin is produced by the parafollicular or C cells of the thyroid interstitium; these cells do not play a role in thyroid hormone production.
Calcitonin • Calcitonin is a 32 amino acid peptide • Inhibits osteoclast mediated bone resorption • Promotes renal excretion of Ca 2+
Calcitonin • The major stimulus of calcitonin secretion is a rise in plasma Ca 2+ levels • PTH and vitamin D act to increase plasma Ca 2+ only calcitonin causes a decrease in plasma Ca 2+. • Calcitonin is a physiological antagonist to PTH with regard to Ca 2+ homeostasis
PTH Actions • The overall action of PTH is to increase plasma Ca++ levels and decrease plasma phosphate levels. • PTH acts directly on the bones to stimulate Ca++ resorption and kidney to stimulate Ca++ reabsorption in the distal tubule of the kidney and to inhibit reabosorptioin of phosphate (thereby stimulating its excretion). • PTH also acts indirectly on intestine by stimulating 1, 25 -(OH)2 -D synthesis.
Disorders of the Parathyroid Glands
¡ Hypofunction ¡ Hyperfunction - hypercalciemia hypophosphatemia hyperphosphaturia osteoporosis Accumulation of Са in tissues - hypocalciemia hyperphosphatemia hypophosphaturia tetanus
Hyperparathyroidism • Enlargement of a single gland or parathyroid adenoma in approximately 80% of cases, multiple adenomas or hyperplasia in 15 to 20% of patients and parathyroid carcinoma in 1% of patients
Hyperparathyroidism – Most people are asymptomatic – Classically affects skeleton, kidneys, and GI tract • Triad of complaints: bones, stones, and abdominal groans – Renal stones are most common single presenting complaint – Usually due to an adenoma (tumor)
Hyperparathyroidism • The disorder is characterized by hypercalcemia, hypercalcuria, hypophosphatemia, and hyperphosphaturia • Most common complication are renal stones made of calcium phosphate • Most serious complication is the deposition of calcium in the kidney tubules resulting in impaired renal function
Normal bone Hyperparathyroid
Primary Hyperparathyroidism • Calcium homeostatic loss due to excessive PTH secretion • Due to excess PTH secreted from adenomatous or hyperplastic parathyroid tissue • Hypercalcemia results from combined effects of PTHinduced bone resorption, intestinal calcium absorption and renal tubular reabsorption • Surgery is the most common treatment for primary hyperparathyroidism.
Secondary Hyperparathyroidism Secondary hyperparathyroidism occurs as a result of another disease that initially causes low levels of calcium in the body and over time, increased parathyroid hormone levels occur. This is due to chronic stimulation of the parathyroid glands by a chronic decrease in the ionic calcium level in the blood
Secondary Hyperparathyroidism • In pts with chronic renal failure • Deficiency of 1, 25 -dihydroxy vitamin D as a result of loss of renal tissue, low calcium intake, decreased calcium absorption, and abnormal parathyroid cell response • Normally treated medically
Congenital Hypoparathyroidism • Hypoplasia of the teeth, shortened roots, and retarded eruption
Hypoparathyroidism • Deficient secretion of PTH which manifests itself biochemically by hypocalcemia, hyperphospatemia diminished or absent circulating PTH and , often causing cramping and twitching of muscles or tetany. • The condition can be inherited, but it is also encountered after thyroid or parathyroid gland surgery, and it can be caused by immune system-related damage
Pseudohypoparathysoidism A rare familial disorders with target tissue resistance to PTH. There is hypocalcaemia, hyperphosphataemia, with increased parathyroid gland function. There is also a variety of congenital defects in the growth and development of skeleton including: • Short statue • Short metacarpal and metatarsal bones
Pseudohypoparathyroidism Elfin facies, short stature, enamel hypoplasia
Hormonal Regulators • Calcitonin (CT) – Lowers Ca++ in the blood – Inhibits osteoclasts and reabsorbtion through kidney • Parathormone (PTH) – Increases Ca++ in the blood – Stimulates osteoclasts • 1, 25 dihydroxy Vitamin D 3 – Increases Ca++ in the blood – Increase Ca++ uptake from the gut – Stimulates osteoclasts
PRACTICE QUESTIONS
Q 1. Secretion of which hormone is stimulated by hypercalciemia and it acts to lower the serum levels of calcium: a) b) c) d) 1, 25 -dihydroxy vitamin D Calcitonin Parathyroid hormone Thyroid hormone Correct Answer: B • Explanation • 1, 25 -dihydroxy vitamin D: It stimulates the absorption of Calcium in the intestine. • Calcitonin: It acts to decrease plasma Calcium levels. • Parathyroid hormone: It increases Calcium concentration by the action on gut, bone and kidney. • Thyroid hormone: Primarily responsible for regulation of body metabolism
Q 2. Which hormone increases the resorption of bone by stimulating osteoclasts and promoting the reabsorption of calcium by the kidneys? a. 1, 25 -dihydroxy vitamin D b. Calcitonin c. Parathyroid hormone d. Thyroid hormone Correct Answer: C Explanation a. 1, 25 -dihydroxy vitamin D: It stimulates the absorption of Calcium in the intestine and Calcium resorption from the bone b. Calcitonin: It acts to decrease plasma Calcium levels. c. Parathyroid hormone: It increases Calcium concentration by bone resorption, renal reabsorption and act indirectly on intestine by stimulating 1, 25 -dihydroxy vitamin D synthesis. d. Thyroid hormone: Primarily responsible for regulation of body metabolism.
Q 3. The major effect of which hormone is a rapid fall in Calcium caused by inhibition of bone resorption: a) 1, 25 -dihydroxy vitamin D b) Calcitonin c) Parathyroid hormone d) Thyroid hormone Correct Answer: B Explanation a. 1, 25 -dihydroxy vitamin D: It stimulates the absorption of Calcium in the intestine. b. Calcitonin: It inhibits osteoclast mediated bone resorption and promotes renal excretion of Calcium c. Parathyroid hormone: It increases Calcium concentration by the action on gut, bone and kidney. d. Thyroid hormone: Primarily responsible for regulation of body metabolism.
Q 4. A 45 year old female has had three vertebral fractures. She has also had a number of kidney stones. Routine labs revealed hypercalcemia. Select the most likely diagnosis: a. Hyperparathyroidism b. Hypoparathyroidism c. Osteomalacia d. Ricket • Correct Answer: A • Explanation A. Hyperparathyroidism: It is characterized by hypercalcemia, hypercalcuria, hypophosphatemia, and hyperphosphaturia with renal stones made of calcium phosphate B. Hypoparathyroidism: It is characterized by hypocalcemia, hyperphospatemia and diminished circulating PTH C. Osteomalacia: It is the softening of the bones caused by impaired bone metabolism primarily due to inadequate levels of available phosphate, calcium, and vitamin D D. Rickets: It is defective mineralization of bones due to deficiency or impaired metabolism of vitamin D, phosphorus or calcium, potentially leading to fractures and deformity.
Q 5. Which disorder is characterized by hypocalcemia, hyperphosphatemia? a) a. Hyperparathyroidism b) b. Hypoparathyroidism c) c. Osteomalacia d) d. Ricket Correct Answer: B Explanation A. Hyperparathyroidism: It is characterized by hypercalcemia, hypercalcuria, hypophosphatemia, and hyperphosphaturia with renal stones B. Hypoparathyroidism: It is characterized by hypocalcemia, hyperphospatemia and diminished circulating PTH C. Osteomalacia: It is the softening of the bones caused by impaired bone metabolism primarily due to inadequate levels of available phosphate, calcium, and vitamin D D. Rickets: It is defective mineralization of bones due to deficiency or impaired metabolism of vitamin D, phosphorus or calcium, potentially leading to fractures and deformity.