SARS Evaluation of the Debriefing Group Experience SARS

壓力簡報團體經驗之成效評估 -以SARS經驗為例 Evaluation of the Debriefing Group Experience - SARS 2003 贊助單位:台北市衛生局 Taipei Health Dept. 執行單位:台北市衛生局心理衛生中心 Taipei City Mental Health Center 執行期間: 92年 10月至 93年 12月 Oct. 2003 till Dec. 2004 研究主持人:李開敏 Kai Ming Lee A. C. S. W. 研究助理:林小雅、張蘭心 S. Y. Lin, L. S. Chang 統計分析:鄒平儀、林小雅 Prof. P. Y. Tzou, S. Y. Lin
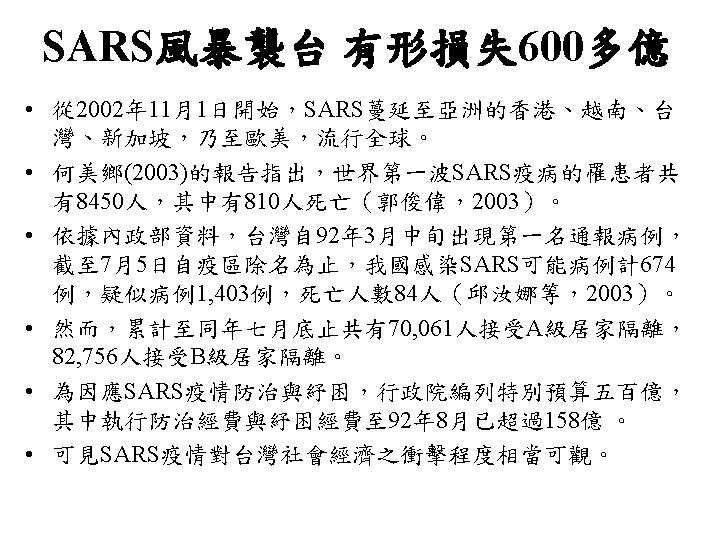

SARS Raided Taiwan • Since 2002 Dec. , SARS swept through H. K. , Vietnam, Taiwan, Singapore, North America and Europe. • There were 8450 patients being reported world-wide, among whom 810 deaths followed. • The first patient in the island was reported around mid March, 2003. • Till July 5 th, as Taiwan was taken off the list of international travel alert. There had been 674 probable cases, 1403 suspected, 84 deaths. • Over 150, 000 were kept in isolation and quarantine. • The administrative Yuan approved 50, 000, 000 NT relief for prevention and treatment.

 movement, founded by Dr. Jeffrey Mitchell,")
CISD • The Critical Incident Stress Debriefing (CISD) movement, founded by Dr. Jeffrey Mitchell, has completed its first decade of crisis intervention service to emergency service organizations worldwide. CISD's seven phase educational and intervention process was designed to mitigate the harmful effects of stress and to accelerate the normal recovery process of emergency personnel who were experiencing normal reactions to abnormally stressful events. • A documented turnover rate of 56% among paramedic personnel over a five to seven year time frame helped to drive the development of Critical Incident Stress Management.
 • CISD teams are composed of peer debriefers and mental health professionals")
CISD (cont’d) • CISD teams are composed of peer debriefers and mental health professionals trained in the unique debriefing process developed by the psychologist and former firefighter, Dr. Jeffrey Mitchell, in response to his experiences and observations in the fire department. • A debriefing is confidential; it is not therapy, not a critique of work performance. The process often lasts 2 -3 hours
 • Dr. Jeffrey T. Mitchell is a Clinical Associate Professor in the")
CISD (cont’d) • Dr. Jeffrey T. Mitchell is a Clinical Associate Professor in the Department of Emergency Health Services at the University of Maryland, Baltimore County. He developed the Critical Incident Stress Debriefing (CISD) process which is utilized by over 300 communities throughout the United States and in five other nations. He founded the International CISD network. He is a well-known speaker who has lectured to emergency personnel in all fifty states and seven countries. • He is the senior author of the following books: Human Elements Training; CISD: An Operations Manual, Second Edition (Revised); Emergency Response to Crisis and Emergency Services Stress. • He has over sixty other publications on critical incident stress, crisis intervention and the treatment of stress in emergency personnel.
 A Critical Incident has been defined by Dr. Jeffrey Mitchell as: \"Any")
CISD (cont’d) A Critical Incident has been defined by Dr. Jeffrey Mitchell as: "Any situation faced by emergency service personnel that causes them to experience unusually strong emotional reactions which have the potential to interfere with their ability to function either at the scene or later. . . All that is necessary is that the incident, regardless of the type, generates unusually strong feelings in the emergency workers. "
 • A debriefing is scheduled 24 -72 hours after the critical incidence")
CISD (cont’d) • A debriefing is scheduled 24 -72 hours after the critical incidence including seven phases: 1. Introduction 2. Fact-finding 3. Immediate Thoughts 4. Personal Reactions 5. Symptoms Experienced 6. Skills and Strategies 7. Re-entry

CISD - Seven Steps 1. Introduction 7. Re-entry 2. Fact-finding 6. Skills and Strategies 3. Immediate Thoughts 5. Symptoms Experienced 4. Personal Reactions

壓力簡報團體經驗之成效評估 -以SARS經驗為例 Evaluation of the Debriefing Group Experience - SARS 2003 贊助單位:台北市衛生局 Taipei Health Dept. 執行單位:台北市衛生局心理衛生中心 Taipei City Mental Health Center 執行期間: 92年 10月至 93年 12月 Oct. 2003 till Dec. 2004 研究主持人:李開敏 Kai Ming Lee A. C. S. W. 研究助理:林小雅、張蘭心 S. Y. Lin, L. S. Chang 統計分析:鄒平儀、林小雅 Prof. P. Y. Tzou, S. Y. Lin

成員基本特質 Characteristics of Subjects 變 項 Variable 性別 Gender 男 M 女 F 年齡 Age 20 -30 歲 31 -40 歲 41 歲 以上 above 未填答 unanswered 人數 N=64 % 5 59 7. 8 92. 2 33 9 16 6 51. 6 14. 1 25. 0 9. 4

成員基本特質 Characteristics of Subjects 變 項 Variable 人數 N=64 作類型 type of occupation 護士 nurse 輔導老師 school counselor 社會 作 social worker 家管 housewife 其他 others 15 22 4 8 % 23. 4 34. 4 6. 3 12. 5

成員基本特質 Characteristics of Subjects 變 項 Variable 人數 N=64 % 團體性質 type of group 社區媽媽 community women self help 社會局身心障礙社 團體 social welfare rehab 董氏基金會教師團體 teachers training group 家庭照顧者總會 family carers asso. 和平醫院員 減壓團體 Ho Ping Hosp. staff 紅十字中正區老人中心 red cross senior center 3 4. 7 16 25. 0 17 26. 6 9 14. 1 13 20. 3 6 9. 4

成員基本特質 Characteristics of Subjects 變 項 Variable 人數 N=64 % 團體位置 position in group 內圈參與減壓者 in debriefing circle 30 46. 9 外圈觀察學習者 out group observer 32 50. 0 未填答 unanswered 2 3. 1

Position in the Group Inner Debriefing Circle Outer Observation Group

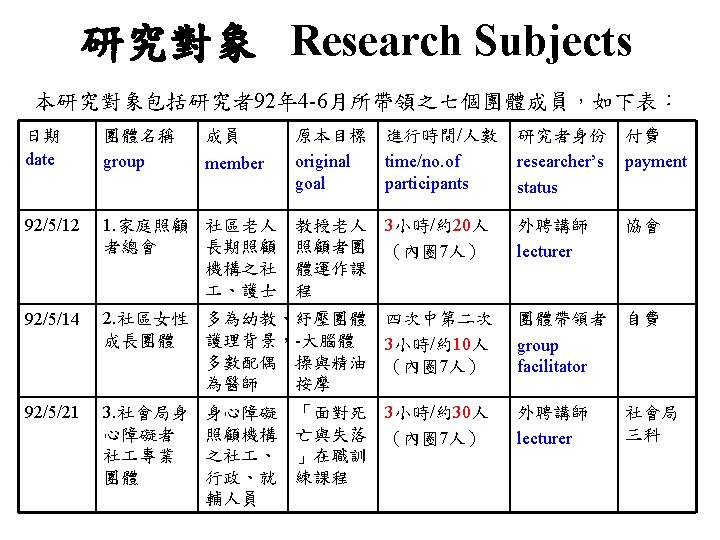
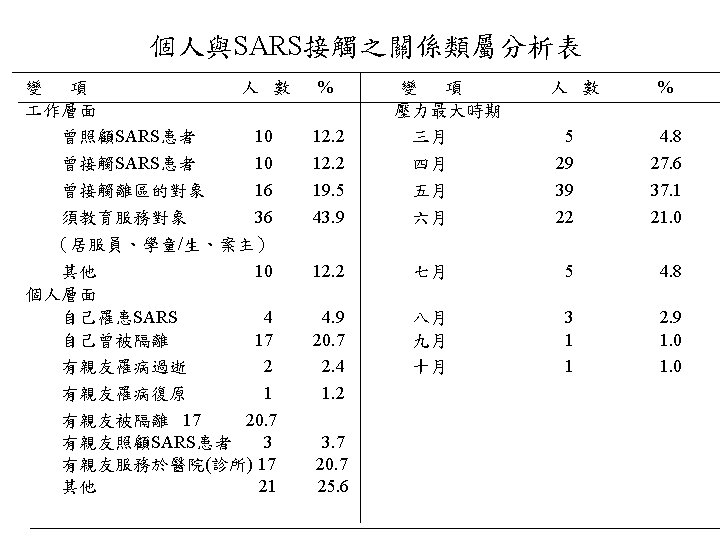
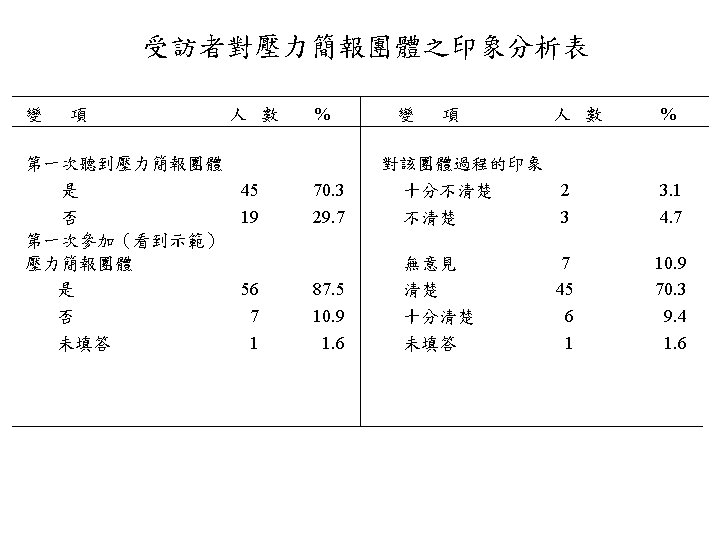
Result The study applies semi-structured questionnaire to collect data regarding professionals’ reaction towards SARS, also to evaluate Mitchell model debriefing as a group intervention. 64 subjects in the study were members who attended the 7 debriefing groups led by the author during April to June, 2003 The Result Shows: 1. 2. 3. 90% of the subjects are considered either primary or secondary victims. ( 9% of the subjects or of the families contracted SARS) Only 30% of the subjects had heard about debriefing, 12. 5% had taken part in debriefing. 80 -90% of the subjects reported positive experience with debriefing, especially found the following aspects helpful: emotional release, group sharing and integrating of the SARS experience, Mitchell model itself and the education.
 4. 5. 6. 7. 8. SARS impact seems to be short term,")
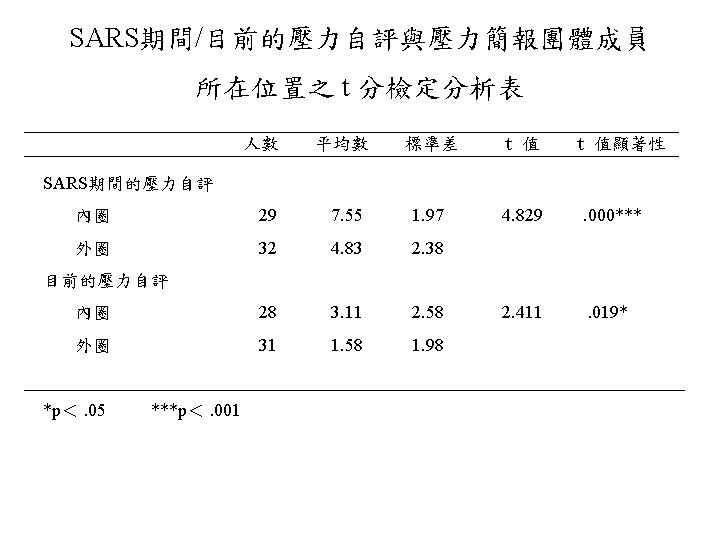
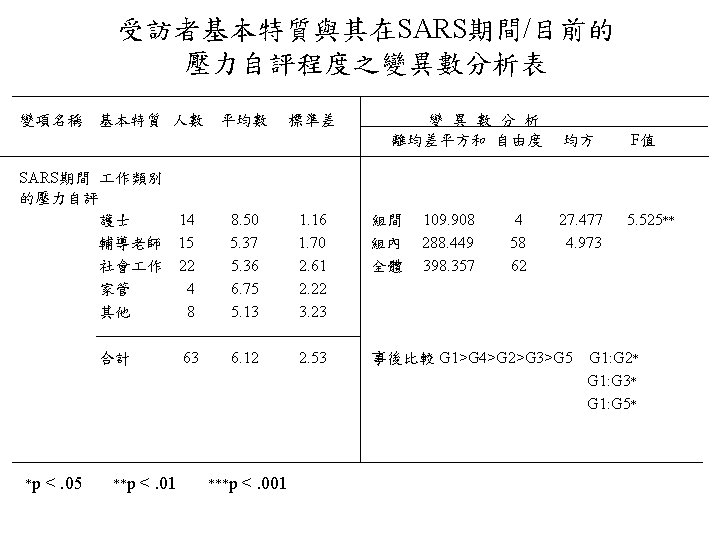
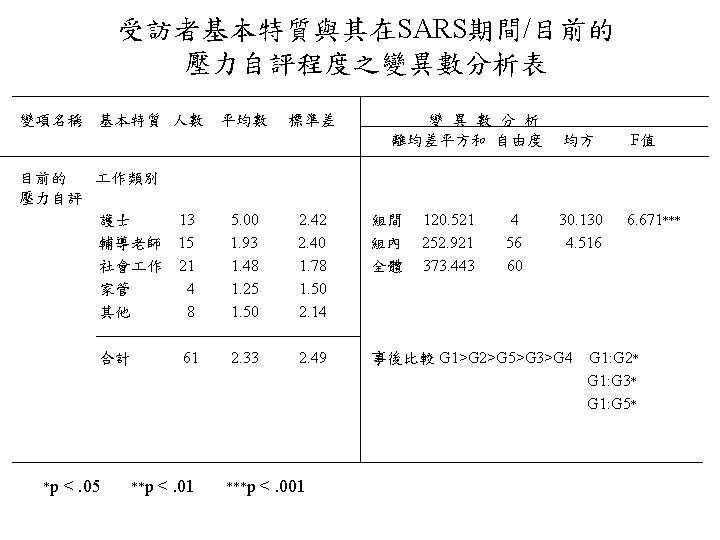
Result (cont’d) 4. 5. 6. 7. 8. SARS impact seems to be short term, acute in nature. Perceived stress level of the subjects was significantly lower after 6 months. (α=. 001) May was the reported highest point of stress by majority. Stress included health/life being threatened, alienation, break down of trust, increase in workload, inconvenience, change in life style ………etc. Nurses reported higher level of stress than counselors, social workers and others. (p<. 05) Ho Pin Hospital group reported higher stress than other groups. (p<. 05) Inner debriefing circle members reported higher stress levels than outer group. (p<. 001) The most remembered parts of the debriefing experience are group sharing, self-disclosure, facilitator factor, stress managing activity, uniqueness of the Mitchell Model.

Recommendation • On practice level---using the Mitchell Model Debriefing 1. Participants need to be informed of the process and take part on voluntary basis. 2. In step 6, it is more empowering to ask members to share how they have coped instead of relying on the facilitator to do all the teaching. It is also beneficial to do a 10 -15 minute relaxation to expand the integrative process and also to prepare for ending. 3. When in large groups, it seems workable to have inner and outer groups to fulfill both intervention and teaching goals.
 • On theoretical level---adapting the model as a group crisis intervention 1.")
Recommendation (cont’d) • On theoretical level---adapting the model as a group crisis intervention 1. The model should be used as psycho-educational rather psychotherapeutic. 2. The model should incorporate more salutogenesis (健康之源 論) rather than pathogenesis (受苦之源論) teaching and information.
 • Future promotion of the model 1. To be taught in college")
Recommendation (cont’d) • Future promotion of the model 1. To be taught in college course of “group work” “ disaster mental health”. 2. To be taught in related organizations: hospitals, mental health center, private sectors. 3. Further research needed. • Understanding SARS and for future crisis 1. Mental health of the professional helper should be emphasized. Job stress of the first line nurses need to be looked at with more support from the system. 2. Mass media’s report on disasters has great impact and needs to be regulated. 3. Governmental intervention needs to be reexamined.

Limitation 本研究屬初步之探索性研究,本研究計畫提出時,七個團體早已完成,正如 同許多災難事件的相關研究,因為事發突然,事先難有完善的規劃,因此, 多半只能針對已完成之服務方案,進行回溯性的單組評估與檢討,這是本研 究調查在測量效度上的最大限制。 1. Geographic limitation Other than Family Carers Asso. , all other groups are located in Taipei. 2. Retrospective nature limits internal validity The survey was done 6 months after SARS. 3. Research method Some questions in the semi-open questionnaire seem overlapping. 4. Variations in intervention Due to the different groups, intervention was not standardized.

Re-entry What did we learn from SARS?



Thank You!
- Slides: 39