Sample Collection Physical Examination 1 st Specimen Collection





 Useful for routine screening but")

 Routine + Microscopic includes the examination of")
 1. Appearance: (color and")



. ² RBCs ²")





 ² Specific gravity measures urine density, or the ability of")










- Slides: 30
Sample Collection & Physical Examination
1 st : Specimen Collection Sample Containers ² Specimen must be collected in a clean dry, disposable a wide mouth container, flat bottom to prevent overturning and properly applied screw top lids. ² Made of clear material to allow for determination of color and clarity. ² Capacity of the container is 50 m. L, which allows 12 m. L of specimen needed for microscopic analysis, additional specimen for repeat analysis.
² Sterile containers are also suggested if more than 2 hours elapse between specimen collection and analysis. ² Container must be properly labeled with patient name, date, and time of collection. ² The labels should be applied to the container and not to the lid. Label here
Note that : ² The specimen must be delivered to the lab & must be delivered within 1 hr ² If you expect the specimen to stay for a long time, it should be Refrigerated or have an appropriate chemical preservative added. eg. (Toluene, thymol, formalin or boric acid).
Changes in unpreserved urine: ² Transformation of urea to ammonia which increase p. H. ² ² ² ² ² Decrease glucose due to glycolysis and bacterial utilization. Decrease ketones because of volatilization. Decrease bilirubin from exposure to light. Decrease urobilinogen as it oxidized to urobilin. Increase bacterial number. Increase turbidity caused by bacteria & amorphous. Increase nitrite due to bacterial reduction of nitrate. Disintegration of RBCs casts, particularly in diluted alkaline urine. Changes in color due to oxidation or reduction of metabolic.
Types of specimens 1. Random specimen (at any time) Useful for routine screening but may give false results due to dietary intake or physical activity just prior to the collection of the specimen It’s not useful for quantitative analysis. 2. First morning specimen Valuable as it’s concentrated to reveal abnormalities and formed elements It’s free of dietary influences and changes due to physical activities Prevents false negative pregnancy test Useful in evaluation of orthostatic proteinuria. 3. 24 hr’s collection Used for quantitative determination and for evaluation the kidney function.
Post. Prandial sample : It taken at specified 4. time after specific meal to know the normal excretion. 5. 6. 7. Clear catch sample (midstream urine ): Best for bacteriological work it’s collected by cleaning the genitalia then the patient takes the midstream urine which is suppose to be the most sterile one. Catheterized urine: Collected form pediatric or adult that can’t give urine. Supra - pubic samples: For bacteriological samples and taken from pediatric mainly.
Routine Urinalysis A routine urine analysis (R+M) Routine + Microscopic includes the examination of physical & chemical characteristics of microscopic studies of some cellular & non-cellular elements.
2 nd : Physical examination of Urine (Macroscopic, Gross analysis) 1. Appearance: (color and clarity) Normal urine color has a wide range of variation ranging from pale yellow, straw, light yellow, dark yellow amber due to urochrome pigment (it’s an end product of endogen metabolism), trace of urobilin and uroerythrin. The color is affected By : ² Concentration of urine, p. H, Metabolic activity, Diet intake and Some Drugs
Abnormalities in color 1. Colorless or pale yellow 2. Dark yellow, Amber, orange ² High fluid intake ² Low fluid intake. ² Using of diuretic. ² Carrots or vitamin (A) ² Reduction in perspiration. ² Nervousness ² Alcohol ingestion ² Diabetes Mellitus. ² Excessive sweating ² Dehydration (burns, fever). ² Pyridium and nitrofurantoin (drugs). ² Diabetes Insipidus (Low level of antidiuretic hormone).
3. Brownish yellow ²Bilirubin ²Urobilin on shaking yellow foam will appear. on shaking the foam has no color. 4. Yellow – green ²Bilirubin oxd. Biliverdin (greenish). ²Which give a yellow foam & (- ve) test for bilirubin 5. Blue – Green ²Pseudomonas Infection
5. Pink – Red Due to the presence of fresh blood or Hb, fresh blood will give smoky color while Hb gives clear reddish urine. Both may be due to ²Trauma ²Calculi ²Urinary tract infection ²Menstrual contamination. 6. Dark brown ²Met hemoglobin if bloody sample long standed, Hb will be oxidized. ²Melanin 7. Black Urine ²Alkaptonurea, a disease of tyrosine metabolism.
Normal urine clear or transparent, any turbidity will indicate. WBCs (pus). ² RBCs ² Epithelial cells ² Bacteria ² Casts ² Crystals ² Lymph ² Semen. ²
2. Odor Fresh normal urine has a faint aromatic odor due to the presence of some volatile acids. In some pathological conditions, certain metabolites may be produced to give a specific odor such as: ² Fruity odor is due to Diabetic urine acetone. ² Ammoniac odor urine standing long time ² Offensive odor Bacterial action of pus (UTI). ² Apple odor Asparagus ² Mousy odor Phenylalanine (phenyl keto urea “PKU” ).
3. Volume Adult urine volume = 600 – 2500 ml /24 hr. Children urine volume = 200 – 400 ml /24 hr. (4 ml / kg / hr). Volume of urine depends on 1. 2. 3. 4. Water intake External temperature. Mental and physical state. Intake of fluid and diuretics (Drugs, alcohol – tea).
Abnormalities ² Oligouria: marked decrease in urine flow < 400 ml. ² Polyuria : Marked increase in urine flow > 2500 ml. ² Anuria : complete stoppage of urine flow. ² Nocturia: excessive urination during night. Causes of polyuria ² Increased fluid in take (polydipsia Polyuria). ² Increased salt intake ad protein diet, which need more water to excrete. ² Diuretics intake (drugs, drinks) ² Intravenous saline or glucose. ² Diabetes Mellitus. ² Diabetes Insipidus. ² Renal disease. ² Hypoaldasteronism.
Causes of oligouria 1 Water deprivation 2 Dehydration 3 - 4 - Renal Ischemia Renal Disease 5 Obstruction by Prolonged vomiting heart failure Calculi Diarrhea Hypotension Tumor Transfusion Reaction Prostatic hyper trophy Excessive sweating . .
Causes of Anuria No Urination 1. Sever Renal Defect and loss of urine formation mechanism. 2. Due to the presence of stone or tumor. 3. Post transfusion hemolytic reaction.
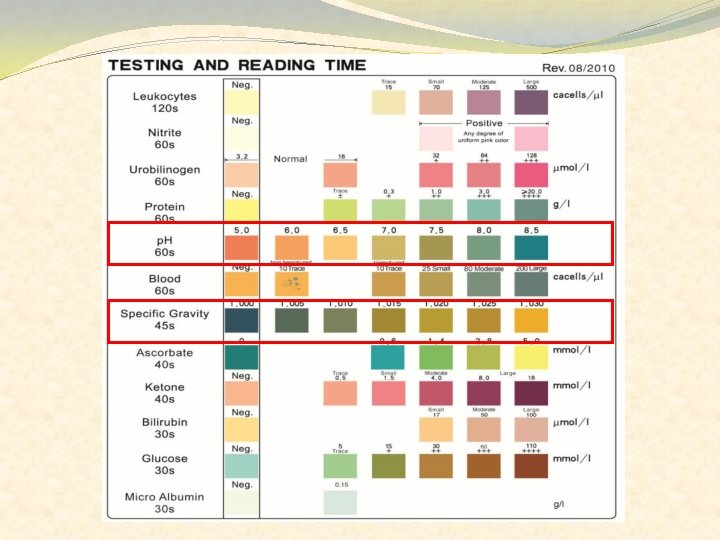
4. Specific Gravity (spg) ² Specific gravity measures urine density, or the ability of the kidney to concentrate or dilute the urine over that of plasma. ² It is directly proportional to urine osmolality which measures solute concentration ² It’s a measure of number and size of molecules ² Hence, large molecules such as urea will contribute to reading more than the small molecules, such as Na+ and K+ ² Hence, osmolality may express this function with more effectively because it’s the number of particles / kg of substance.
²Specific gravity between 1. 002 and 1. 035 on a random sample should be considered normal if kidney function is normal. Since the spg of the glomerular filtrate in Bowman's space ranges from 1. 007 to 1. 010, any measurement below this range indicates hydration and any measurement above it indicates relative dehydration. ²
Low specific gravity ²Diabetes Insipidus ²Glomerulonephritis ²Sever renal damage (diminish the concentration ability of the kidney) ²Excessive water intake. High specific gravity ²Diabetes mellitus. ²Nephrosis ²Fever since urine is conc. ²Urine preservative substance ²X ray contrast media
Measurement of spg 1. Urinometer: ² ² ² Consists of a weighted float a hatched to a scale that has been calibrated in terms of urine spg. (1. 00 – 1. 040) The weighted float displaces a volume of liquid equal to its weight and has been designed to sink to a level of 1. 000 in distilled water. The additional mass by the dissolved substances in urine causes the float to displace a volume of urine smaller than of D. W. , the level to which the urinometer sinks represent the specimen spg.
Disadvantages of urinometer: • The minimum amount of urine to be measured is about 15 ml. • If the urine is so turbid it is difficult to read the result. 2. Refractometer Determine spg by measuring the refractive index of urine
3. Reagent strip: Which contain polyelectrolyte, when ions increase in urine, more acidic groups are released, the change in p. H will take place which change the color of bromothymol blue indicator. (ions in low spg urine) C – OO – H+ Less H+ release because less urine ions is present so increased p. H (ions in high spg urine) C – OO – H+ H+ replaced by urine ions & released in urine so decreased p. H
5. PH ² One of the important functions of the kidneys is p. H regulation, the glomerular filtrate of blood plasma is usually acidified by renal tubules and collecting ducts from a p. H of 7. 4 to about 6 in the final urine to keep blood p. H about 7. 4. ² Urine p. H must vary to compensate for diet and products of metabolism, this function takes place in the distal convoluted tubule with the secretion of both H+ & NH 3+ and reabsorption of bicarbonate. ² In cases of alkalosis, urinary p. H will be alkaline by stop H+ excretion. Normal urine p. H is (4. 6 – 8. 0) as average (6. 0) ²
Clinical significance of p. H 1. Determine the existence of metabolic acid base disorder 2. Precipitation of crystals to from stone requires specific p. H for each type. Hence, p. H control may inhibit the formation of these stones by control diet. ² High protein will give acidic urine. ² High vegetable will give alkaline urine ² In addition to some drugs which control p. H. ² Crystals found in alkaline urine: Ca carbonate, Ca phosphate, Mg phosphate, and amorphous phosphate. ² Crystals found in acidic urine: Ca oxalate, Uric acid, Cystine, Xanthine and amorphous urate.
3. May indicate the presence of urinary tract infection caused by urea splitting organisms. 4. Defects in renal tubular secretions and reabsorption of acid & base. 5. Determination of unsatisfactory specimens. Even in abnormal conditions, urine p. H mustn’t reach 9, if so or more this will indicate that urine is stand for along time & must be rejected.
Test for p. H Reagent strip which has an indicator (methyl red – bromothymol blue indicator) or other indicators. Alkaline urine is found in: Patient with alkalemia, UTI, diets high with citrus fruits or vegetables. Acidic urine is found in: Patient with acidemia, starvation, dehydration, high diets with meat products
The End