SALIVARY GLAND TUMORS Dr GITANJALI KHULBE MDS OMDR
")
SALIVARY GLAND TUMORS - Dr GITANJALI KHULBE MDS (OMDR)

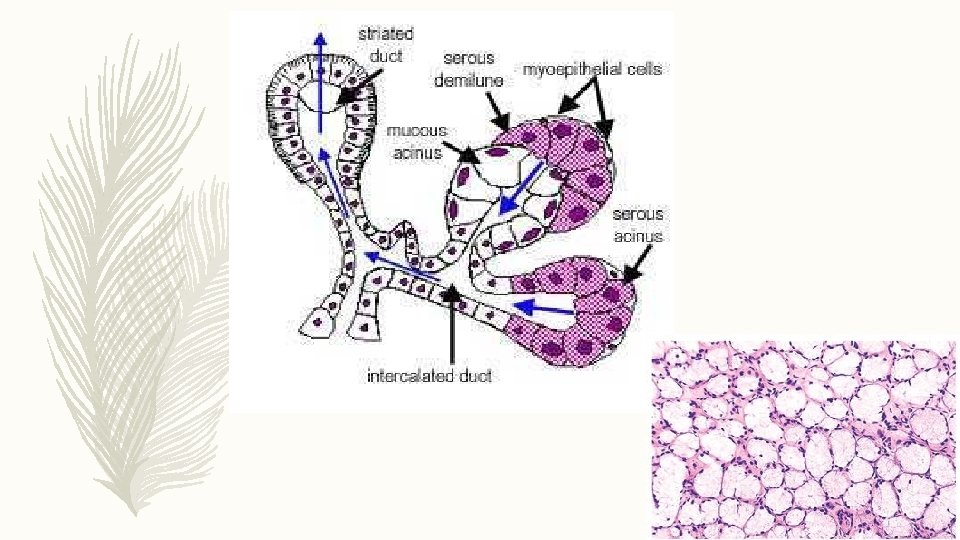
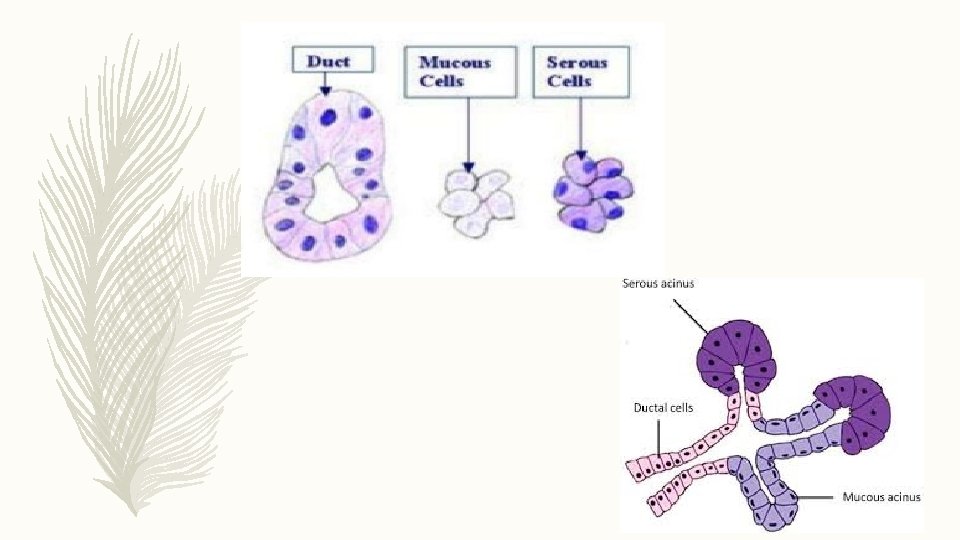
INTRODUCTION: – Saliva is produced by the three major salivary glands – parotid, submandibular and sublingual. – There also 600 to 1000 minor salivary glands which produce saliva. – Saliva-producing acinar cells can be classified into – serous, mucous or a mix of the two types. – Tumors of the salivary glands are relatively uncommon and best distinguished by their histologic patterns.

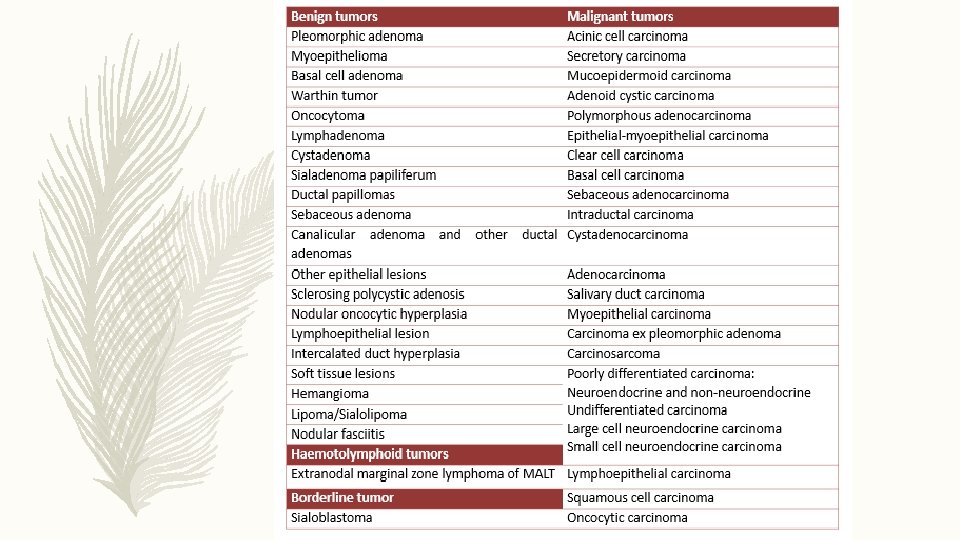
BENIGN TUMORS MALIGNANT TUMORS – Slow growing Sometimes fast growing – Soft or rubbery consistency Sometimes hard consistency – Do not ulcerate May ulcerate and invade bone – No associated nerve signs May cause cranial nerve palsies – Form 85% of parotid tumors 45% of minor gland tumors are malignant.

– Salivary gland neoplasms arise most commonly in the parotid glands followed by submandibular, sublingual and minor glands. – The presentation of malignant neoplasm includes ulceration of the overlying mucosa, fixation of mass to deeper tissues, induration, invasion and cervical lymphadenopathy. – Otalgia, dysphagia, odynophagia, trismus, paresthesia, or cachexia may also be present.
:")
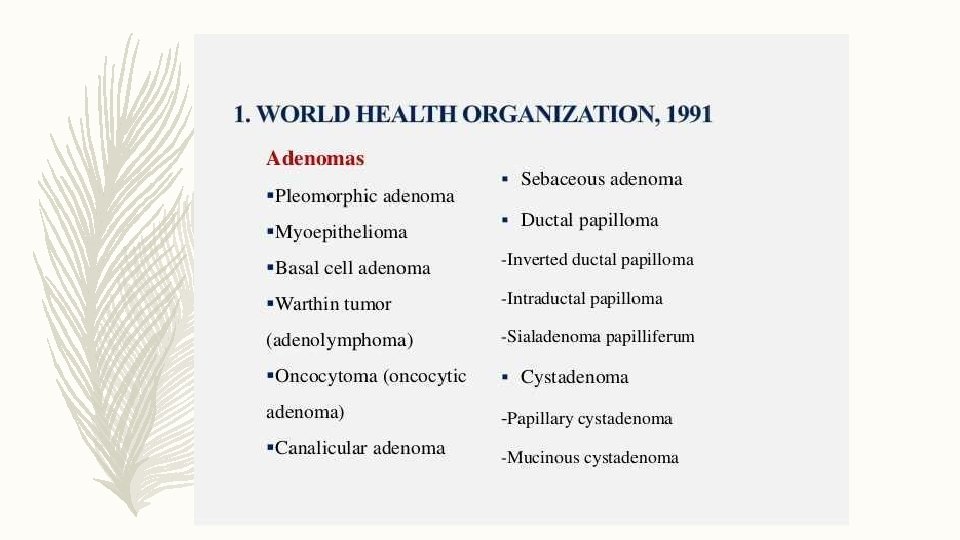
HISTOLOGIC CLASSIFICATION (WHO 1991):

PLEOMORPHIC ADENOMA: – It is the most common tumor of the salivary gland, commonest site being the parotid gland. – The tumor cells exhibit the ability to differentiate to epithelial as well as mesenchymal cells. – Majority are found in fourth to sixth decades of life, female to male ratio being 6: 4. – Myoepithellial cells are a major component, mucoid material and foci of hyalinization are noted in the stroma.

– Most often presents in the lower pole of the superficial lobe. – It is an irregular nodular lesion firm in consistency, areas of cystic degeneration may sometimes be palpated. – Local discomfort is frequently present. – Surgical excision is the treatment, radiation therapy is contraindicated.

MYOEPITHELIOMA: – Coined by Sheldon, it is an uncommon salivary gland tumor accounting for less than 1% of all salivary tumors. – Parotid gland is most commonly involved, the most frequent intraoral site being the palate. – Neoplastic myoepithelial cells are predominantly spindle-shaped or plasmacytoid. – Treatment is by surgical excision.

BASAL CELL ADENOMA: – It is a neoplasm composed of basaloid epithelial cells arranged in solid, trabecular, tubular or membranous patterns. – Occurs primarily in the major salivary glands, particularly the parotid. – There is a 2: 1 female predilection with peak incidence seen in 6 th decade. – Tumors are usually painless, are characterized by slow growth. – It appears as a firm swelling which may be cystic and compressible. – Treatment is by excision.
: – The second most common tumor in the salivary")
WARTHIN’S TUMOR (PAPILLARY CYSTADENOMA LYMPHOMATOSUM): – The second most common tumor in the salivary glands. – It is generally superficial, lying just beneath the parotid capsule or protruding through it. – It is not painful and firm to palpation. – Surgical excision is the treatment.

ONCOCYTOMA: – It is a rare benign tumor composed of oncocytes with granular eosinophilic cytoplasm. – It is more common in women, occurs almost exclusively in elderly. – Measuring 3 -5 cm in diameter, it appears as a discrete, encapsulated mass which is sometimes nodular. – It may show recurrence and appear as clear-cell oncocytoma. – Surgical excision is the management.

DUCTAL PAPILLOMA: – These are adenomas with unique papillary features and arise from salivary gland duct system. – Histologically, are divided into three types: • Inverted ductal papilloma • Intraductal papilloma • Sialadenoma papilliferum – Surgical excision is curative.

CYSTADENOMA: – It is a neoplasm in which the epithelium demonstrates adenomatous proliferation characterised by formation of multiple cystic structures. – If mucous cells predominate in the lining epithelium, the tumor is termed ‘mucinous cystadenoma’. – It is widely distributes among major and minor salivary glands. – Female-to-male ratio is 2: 1, most common in the 8 th decade. – Conservative surgical excision is the treatment.

ACINIC CELL CARCINOMA: – It is a malignant epithelial neoplasm in which the cells express acinar differentiation. – More than 80% of the cases occur in the parotid gland, most common intraoral sites are lips and buccal mucosa. – Female-to-male ratio is 3: 2, mean age of occurrence being 44 years.

– The treatment is surgical. – Lymph node dissection is indicated only in case of clinical involvement.

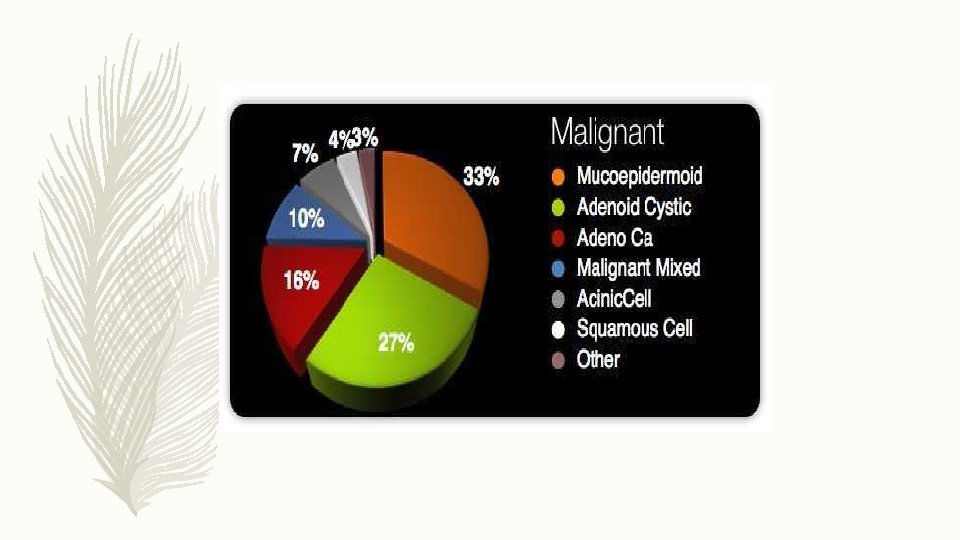
MUCOEPIDERMOID CARCINOMA: – It represents 29 -34% of malignant tumors originating in the salivary glands. – The tumor is composed of both mucus-secreting cells and epidermoidtype cells. – It has a slight female predilection, can occur in all decades. – Based on malignancy, it is graded as – tumor of low-grade, intermediategrade, or high-grade.

– Conservative excision with preservation of facial nerve, is recommended for low- and intermediate-grade tumors. – Radical neck dissection is performed in case of a T 3 lesion or cervical node metastasis. – Post-operative radiation for high-grade malignancies is indicated.

ADENOID CYSTIC CARCINOMA: – It is a slow-growing but aggressive neoplasm with a remarkable capacity for recurrence. – Parotid, submandibular and accessory glands in the palate and tongue, are most commonly involved. – Occurs most commonly in the 5 th and 6 th decades and is more common in females. – Treatment is chiefly surgical, X-ray radiation can also be used as adjuvant.

BASAL CELL ADENOCARCINOMA: – It is a low-grade malignant neoplasm but has a small potential for metastasis. – Occurs predominantly in the 7 th decade, without gender preference. – Swelling is typically the only sign or symptom experienced. – Wide surgical excision is the primary treatment.

SALIVARY DUCT CARCINOMA: – It is a rare, high-grade malignant neoplasm composed of structures which resemble expanded salivary gland ducts. – Approx. 75% of the patients are males, more than 85% of cases involve the parotid gland. – Parotid swelling is the most common sign, facial nerve paralysis may also occur. – Complete local excision with radical neck dissection and post-operative radiation therapy, offers maximum benefit.

SQUAMOUS CELL CARCINOMA: – Primary SCC of the ‘major’ salivary glands is composed of squamous/epidermoid cells. – It accounts for about 1. 6% of salivary gland neoplasms. – There is a 2: 1 male-to-female ratio of occurrence and patients are usually over age 60. – Presents as firm, enlarging mass often fixed to surrounding tissue and associated with pain or facial weakness. – Treatment consists of surgical resection, neck dissection and postoperative radiation.

MALIGNANT LYMPHOMAS: – Salivary glands are affected in only 5% of all primary extra-nodal malignant lymphomas. – Lymphomas of the major salivary glands are characteristically of the non. Hodgkin’s type. – The most commonly involved salivary gland is parotid, followed by the submandibular gland minor salivary glands. – Primary NHLs of the salivary glands have been reported to occur in a background of chronic immune-mediated diseases, such as Sjogren's syndrome and benign lymphoepithelial lesion.

THANK YOU….
- Slides: 28