Salivary Gland Neoplasms Mucoepidermoid Carcinoma Most common salivary




















- Slides: 21
Salivary Gland Neoplasms
Mucoepidermoid Carcinoma • • Most common salivary gland malignancy 5 -9% of salivary neoplasms Parotid 45 -70% of cases Palate 18% 3 rd-8 th decades, peak in 5 th decade F>M Caucasian > African American
Mucoepidermoid Carcinoma • Presentation – Low-grade: slow growing, painless mass – High-grade: rapidly enlarging, +/- pain – Minor salivary glands: may be mistaken for benign or inflammatory process • Hemangioma • Papilloma • Tori
Mucoepidermoid Carcinoma • Gross pathology – Well-circumscribed to partially encapsulated to unencapsulated – Solid tumor with cystic spaces
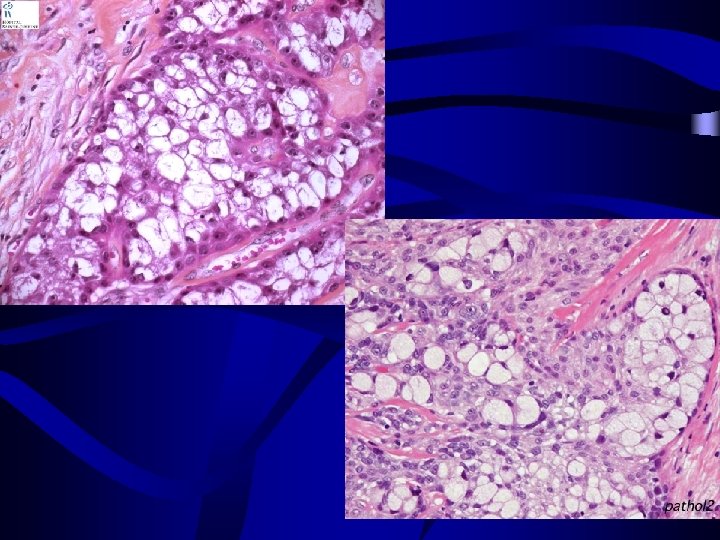
Histopathology: • Mucous secreting cells • Epidermoid cells • Intermediate cells
• Mucous cells- Abundant foamy cytoplasm that stains positively with mucin stain • Epidermoid cells- Squamoid features, polygonal in shape, intercellular bridges, rarely keratinization. • Intermediate cells- Basaloid cells Progenitor ?
Mucoepidermoid Carcinoma Histology—Low-grade – – Mucus cell > epidermoid cells Sparse clusters of intermediate cells Prominent cysts Mature cellular elements
Mucoepidermoid Carcinoma • Histology—Intermediate- grade – epidermoid > mucous cells – Fewer and smaller cysts – Increasing pleomorphism and mitotic figures • Mucus production is scant and may be difficult to document without sp. Stains
Mucoepidermoid Carcinoma • Histology—High-grade – Epidermoid > mucus – Solid tumor cell proliferation – Mistaken for SCC • Mucin staining
• Sclerosing mucoepidermoid carcinoma • Intraosseous mucoepidermoid carcinoma
Treatment – Influenced by site, stage, grade – Stage I & II • Wide local excision – Stage III & IV • Radical excision • +/- neck dissection • +/- postoperative radiation therapy
Adenoid Cystic Carcinoma • Overall 2 nd most common malignancy • Most common in parotid, submandibular and minor salivary glands – palate and tongue • M=F • 5 th decade • Presentation – Asymptomatic enlarging mass – Pain, paresthesias, facial weakness/paralysis
Adenoid Cystic Carcinoma • Gross pathology – Solid, rarely with cystic spaces – infiltrative
Histopathology: • Small dark myoepithelial cells and cells resembling the lining of normal ducts. • These cells may be arranged in double layered, duct like structures which often contain eosinophilic PAS- positive material.
Histopathology • Tumor composed sheets of basaloid cells with scant cytoplasm arranged in a cribiform/ tubular / solid
• Histology—cribriform pattern – Most common - Small darkly staining cells arranged around microcystic spaces. – “swiss cheese” / honey comb appearance
• Histology—tubular pattern – Layered cells forming duct-like structures – Basophilic mucinous substance • Histology—solid pattern – Solid nests of cells without cystic or tubular spaces
Perineural invasion is characteristic
The most commonly used grading system for adenoid cystic carcinoma is based on the proportion of the tumor with a solid pattern. • Grade I ; tumors Show cribriform and tubular patterns and lack any solid component. • Grade II ; lesions are mixed tumors with cribriform and tubular architecture with less than 30% of solid areas. • Grade III; lesions are tumors with 30% or more of solid areas.
Treatment – Complete local excision – Tendency for perineural invasion: facial nerve sacrifice – Postoperative XRT Prognosis – Local recurrence: 42% – Distant metastasis: lung – Indolent course: 5 -year survival 75%, 20 -year survival 13%